Acute pyogenic haematogenous osteomyelitis
Reading File
Finding Sources
Searching PubMed
"acute hematogenous osteomyelitis" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Searching Images
acute pyogenic haematogenous osteomyelitis metaphysis pathology
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full response.
Acute Pyogenic Haematogenous Osteomyelitis
Definition
Osteomyelitis is inflammation of bone and marrow, virtually always secondary to infection. In the haematogenous form, organisms reach bone via the bloodstream from a distant focus — a seemingly trivial mucosal injury, minor skin infection, or bacteraemia from another site. — Robbins & Kumar Pathologic Basis of Disease
Epidemiology & Predisposing Factors
| Feature | Detail |
|---|---|
| Age | Most common in children (3 months – 16 years); distinct patterns in neonates |
| Sex | Male predominance (M:F = 2:1 to 3:1) |
| Skeleton | Long bones ~80% of cases; distal metaphysis is the typical site |
| Risk factors | Diabetes, open fractures, orthopaedic surgery, IV drug use, immunosuppression, sickle cell disease, malnutrition, indwelling catheters |
— ROSEN's Emergency Medicine; Rockwood & Green's Fractures in Adults
Pathophysiology & Why the Metaphysis?
The metaphysis is the classic site in children because:
- Terminal metaphyseal arterioles make sharp loops just beyond the physis
- Blood flow is sluggish at these loops
- Phagocytic activity is poor in this region
- S. aureus cell wall proteins bind directly to bone matrix collagen, facilitating bacterial adherence
In neonates, metaphyseal vessels still penetrate the growth plate → infection can spread to the epiphysis and adjacent joint (septic arthritis in ~50% of neonatal cases).
In adults, growth plate closure creates anastomoses between metaphyseal and epiphyseal vessels, so subchondral and epiphyseal regions become more commonly involved.
— Miller's Review of Orthopaedics; Robbins & Kumar PBD; Grainger & Allison's Diagnostic Radiology
Causative Organisms
| Setting | Most Likely Organisms |
|---|---|
| Children (all ages) | S. aureus (80–90% of culture-positive cases); MRSA now most common in AHO |
| Neonates | Group B Streptococcus, E. coli |
| Sickle cell disease | Salmonella spp. (areas of osteonecrosis act as nidus) |
| HIV/AIDS | S. aureus + opportunistic fungi; also Bartonella (bacillary angiomatosis) |
| Open fractures / surgery | Mixed bacterial infections |
| Older adults | S. aureus, gram-negatives (urinary source) |
Organisms are only identified microbiologically in ~50% of cases; blood cultures are positive in ~40% of paediatric AHO cases but tissue cultures yield organisms 86% of the time.
— Robbins & Kumar PBD; ROSEN's Emergency Medicine
Pathological Sequence
Acute Phase (first 48 hours)
- Bacteria proliferate → neutrophilic infiltrate
- Bone cell and marrow necrosis within 48 hours
- Bacteria + inflammatory response spread via Haversian canals → periosteum
- In children, subperiosteal abscesses dissect along the bone surface (loose periosteal attachment)
- Periosteal lifting → further impairment of blood supply → more necrosis
- Subperiosteal abscess may rupture → soft tissue abscess → draining sinus tract
Transition to Chronic
After the first week, chronic inflammatory cells release cytokines that:
- Stimulate osteoclastic bone resorption
- Drive fibrous tissue ingrowth
- Deposit reactive bone at the periphery
Key structural consequences:
- Sequestrum — devitalised dead bone fragment
- Involucrum — shell of new reactive periosteal bone surrounding the sequestrum
- Brodie abscess — chronic walled-off intraosseous abscess with a sclerotic rim (subacute form)
— Robbins & Kumar PBD; Grainger & Allison's
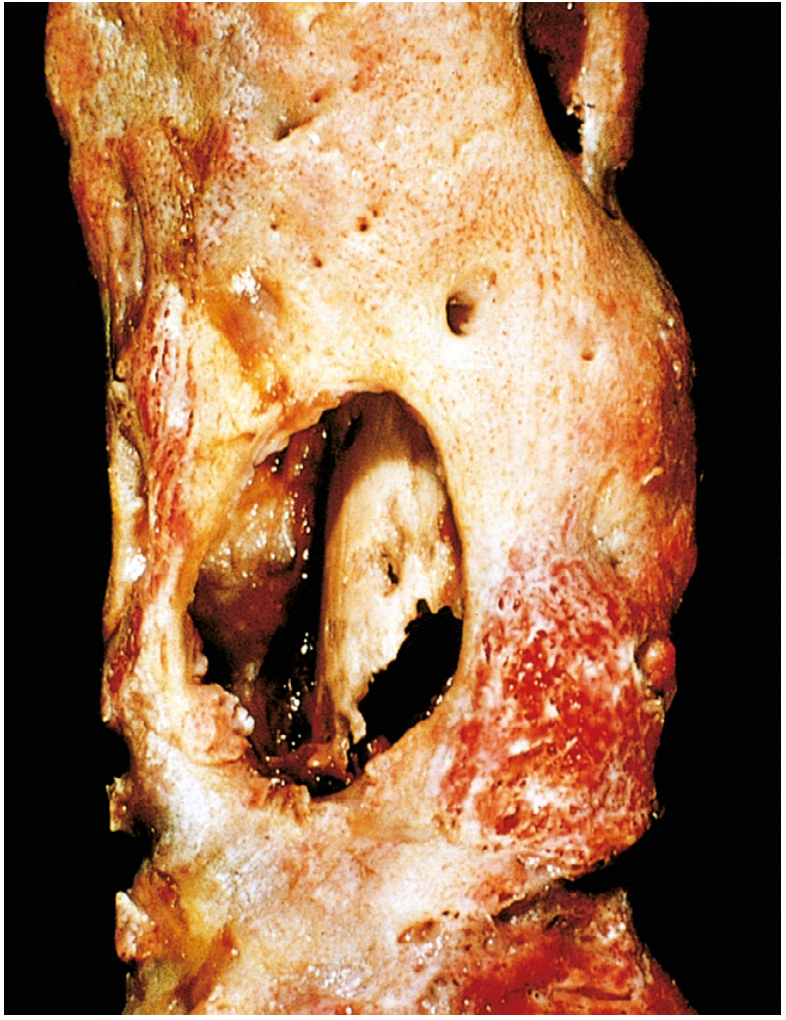
Resected femur in established osteomyelitis. The drainage tract in the subperiosteal involucrum reveals the inner necrotic cortex (sequestrum). — Robbins & Kumar PBD, Fig. 26.16
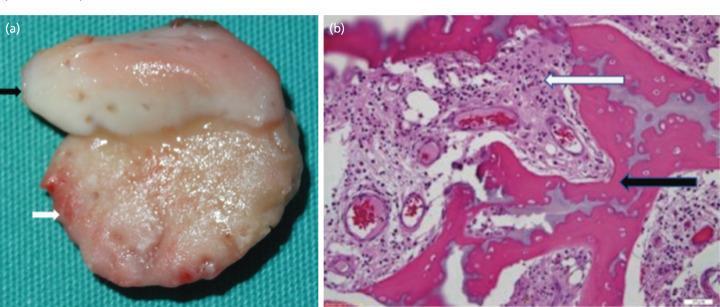
Gross and microscopic appearance of acute osteomyelitis: (a) pathological growth plate cleavage; (b) H&E showing necrotic trabeculae and acute inflammatory infiltrate in marrow
Clinical Features
Systemic:
- Fever, rigors, malaise, anorexia, headache
- Children may appear moderately unwell but not usually "toxic"
- Neonates may have minimal systemic signs — paucity of findings is characteristic
Local:
- Point tenderness over the infected metaphysis — the most consistent finding
- Swelling, warmth, erythema (variable)
- Sudden limp or refusal to bear weight in children
- Sympathetic joint effusion (without joint infection)
— ROSEN's Emergency Medicine
Investigations
Laboratory
| Test | Finding |
|---|---|
| WBC | Usually elevated |
| ESR | Elevated |
| CRP | Elevated; best marker for monitoring treatment response |
| Blood cultures | Positive in ~40% of paediatric AHO; up to 77% yield in some series |
| Bone/tissue cultures | Positive ~86% of cases |
CRP that fails to decline within 48–72 hours of appropriate antibiotics warrants treatment reassessment.
Imaging
| Modality | Findings / Role |
|---|---|
| Plain X-ray | First-line; often normal in first 10–14 days of acute infection. Early: soft tissue swelling. Late: cortical irregularity, periosteal reaction, osteolysis (requires 30–50% mineral loss). Periosteal new bone appears at 5–7 days |
| Ultrasound | Early subperiosteal fluid, useful in neonates/children; guides aspiration |
| MRI | Highest sensitivity and specificity; modality of choice. Identifies intramedullary signal change, soft tissue/subperiosteal abscesses, extent of disease. Penumbra sign in subacute infection = peripheral high-signal ring (granulation tissue) around low-signal abscess centre |
| CT | Best for cortical destruction detail, sequestra identification, preoperative planning; radiation cost |
| Bone scintigraphy (Tc-99m) | Useful for multifocal disease in neonates; whole-body MRI preferred when available |
— Grainger & Allison's; Miller's Review; Rockwood & Green's
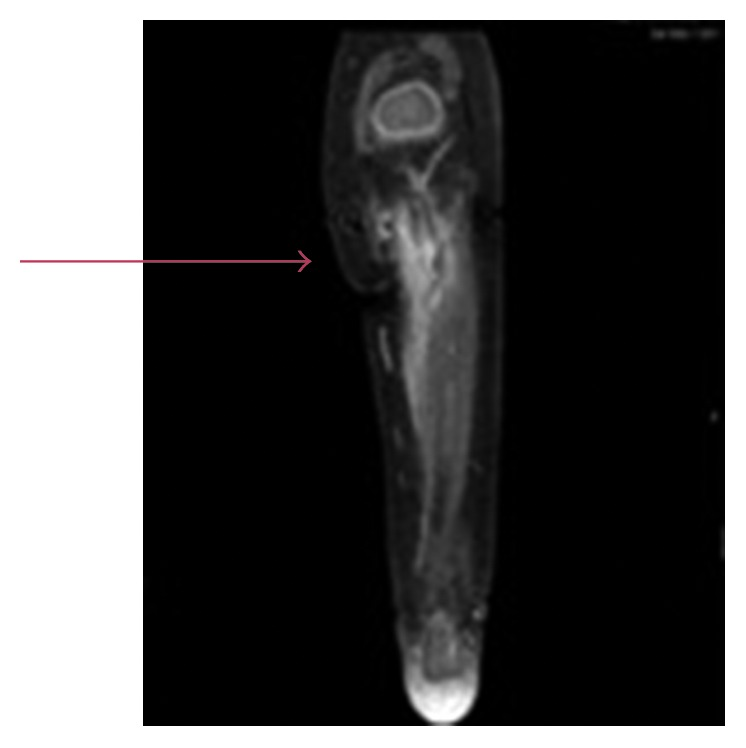
MRI (T1 fat-saturated post-contrast), coronal view of proximal tibia: intramedullary enhancement with periosteal/soft tissue involvement (arrow) — early acute osteomyelitis
Management
Antibiotic Therapy
- IV antibiotics are the best initial treatment when diagnosed early and no abscess is present
- Empirical broad-spectrum cover → narrow once organism and sensitivities identified from aspiration/culture
- MRSA must be covered empirically in communities with high prevalence
- CRP is the preferred marker to monitor antibiotic response
- Duration: typically 4–6 weeks total (IV transitioning to oral once CRP improving and no surgical indication)
Surgical Indications
- Failure to respond to antibiotics within 48–72 hours
- Frank pus on MRI or subperiosteal/intraosseous abscess not amenable to percutaneous drainage
- Sequestered abscess (Brodie abscess not accessible to antibiotics)
- Metaphyseal drilling can assist drainage
Outcome
- When treated promptly: usually curative
- In 5–25% of acute cases, infection fails to resolve → chronic osteomyelitis
- Worse outcomes with: delayed diagnosis, extensive bone necrosis, inadequate debridement, or immunocompromise
— Miller's Review of Orthopaedics; Robbins & Kumar PBD; Rockwood & Green's
Complications
| Complication | Notes |
|---|---|
| Chronic osteomyelitis | Spontaneous flares after years of dormancy |
| Septic arthritis | Especially in neonates and infants (joint capsule attachments at metaphysis) |
| Growth disturbance | Epiphyseal involvement → limb shortening or deformity in children |
| Pathological fracture | Through infected/necrotic bone |
| Bacteraemia / sepsis | From haematogenous dissemination |
| Secondary amyloidosis | Reactive (AA) amyloid from chronic inflammation |
| Squamous cell carcinoma | Malignant transformation in long-standing draining sinus tracts (Marjolin's ulcer equivalent) |
| Brain abscess / meningitis | From contiguous or haematogenous spread |
— ROSEN's Emergency Medicine; Robbins & Kumar PBD
Summary Algorithm (Paediatric AHO)
Clinical suspicion (fever + point tenderness + limited limb use)
↓
Blood cultures + WBC/ESR/CRP
↓
Plain X-ray (may be normal early)
↓
If X-ray equivocal/normal → MRI (preferred) or Bone scan
↓
MRI confirms: start IV antibiotics empirically (anti-MRSA cover)
↓
Percutaneous aspiration/biopsy → culture-directed therapy
↓
CRP monitoring every 48–72 h
↓
No improvement → surgical drainage/debridement
Sources: Robbins & Kumar Pathologic Basis of Disease; Robbins, Cotran & Kumar PBD; ROSEN's Emergency Medicine; Grainger & Allison's Diagnostic Radiology; Miller's Review of Orthopaedics; Rockwood & Green's Fractures in Adults 10e
This is a shared conversation. Sign in to Orris to start your own chat.