Role of lung ultrasound in diagnosis of critical clinical conditions
Reading File
search_medical_text
lung ultrasound diagnosis critical conditions ICU
search_medical_text
lung ultrasound findings pneumothorax pleural effusion pulmonary edema pneumonia
search_medical_image
lung ultrasound B-lines A-lines pleural sliding signs
GradeResponse
GradeResponse
GradeResponse
search_medical_text
BLUE protocol lung ultrasound acute respiratory failure algorithm
search_medical_image
lung ultrasound pleural effusion consolidation pneumonia ultrasound image
GradeResponse
I now have solid material to compose a comprehensive answer. Here is a detailed synthesis.
Lung Ultrasound in the Diagnosis of Critical Clinical Conditions
Lung ultrasound (LUS) has transformed bedside assessment in emergency and critical care. It is rapid, radiation-free, repeatable, and — when performed by a trained clinician — achieves diagnostic accuracy exceeding 90% for the most common etiologies of acute respiratory failure in the ICU (Bedside General and Cardiac Ultrasonography in the Evaluation of Critically Ill Patients, p. 13).
Principles and Basic Signs
Ultrasound interacts with the lung through its pleural interface. The key artifacts and signs form the diagnostic language of LUS:
| Sign | Appearance | Significance |
|---|---|---|
| Lung sliding | Shimmering movement of pleural line with respiration | Normal aerated lung; rules out pneumothorax at that site |
| A-lines | Horizontal, equidistant, hyperechoic reverberation artifacts below pleural line | Normal aeration or pneumothorax (in absence of sliding) |
| B-lines (comet tails) | Vertical, laser-like hyperechoic artifacts from pleura to screen edge, erasing A-lines | Interstitial fluid / thickened subpleural septa |
| Consolidation | Tissue-like ("hepatization") appearance replacing air | Pneumonia, atelectasis, infarction |
| Pleural effusion | Anechoic or echogenic fluid above diaphragm | Transudate, exudate, hemothorax, empyema |
The spectrum runs from normal (A-lines + sliding) → interstitial syndrome (B-lines) → consolidation → effusion, with each pattern pointing to specific pathology.
Critical Conditions: Findings and Diagnostic Approach
1. Pneumothorax
- Loss of lung sliding at the affected zone is the hallmark finding.
- A-lines persist without B-lines (air in the pleural space reflects the ultrasound beam).
- The lung point — the transition between sliding and non-sliding pleura — is pathognomonic for pneumothorax and can be used to estimate size.
- In M-mode: loss of the normal "seashore sign," replaced by the "barcode/stratosphere sign".
- LUS is more sensitive than supine chest X-ray for pneumothorax — critical in mechanically ventilated patients.

2. Acute Pulmonary Edema / Cardiogenic Pulmonary Congestion
- Diffuse bilateral B-lines (≥3 per intercostal space, in ≥2 bilateral zones) indicate interstitial-alveolar edema.
- Coalescent B-lines < 3 mm apart suggest pulmonary edema or confluent bronchopneumonia.
- Absence of consolidation and presence of preserved sliding favors cardiogenic over infectious etiology.
- Combined with cardiac ultrasound (reduced LV function, dilated IVC) increases specificity dramatically.
- LUS can monitor response to diuretic therapy in real time.
3. Pneumonia / Consolidation
- Affected lung appears hepatized — solid, tissue-like, with irregular borders.
- Air bronchograms (dynamic or static hyperechoic foci within consolidation) help distinguish pneumonia from atelectasis (dynamic bronchograms = patent airways = pneumonia).
- Irregularly spaced B-lines (not evenly 7 mm apart) alongside focal consolidation are typical.
- Sensitivity and specificity for alveolar consolidation >90% (Bedside Ultrasonography, p. 13).
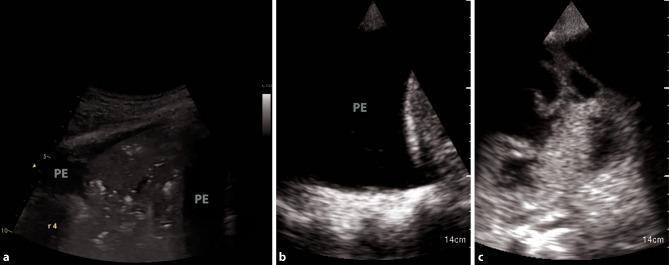
4. Pleural Effusion
LUS distinguishes between effusion types based on echogenicity and internal architecture:
| Type | Appearance | Likely Etiology |
|---|---|---|
| Simple / Transudative | Uniformly anechoic (black), no internal echoes | Heart failure, hepatic/renal disease |
| Exudative / Complex | Heterogeneous, internal echoes | Parapneumonic effusion, malignancy |
| Empyema | Septations, fibrinous strands, loculations | Infection |
| Hemothorax | Echogenic, swirling particulate matter | Trauma, aortic dissection |
LUS guides safe and accurate thoracentesis — far superior to clinical landmarks alone.
5. Acute Respiratory Distress Syndrome (ARDS)
- Bilateral, non-homogeneous B-line distribution (spared areas with A-lines interspersed).
- Subpleural consolidations, pleural line irregularities.
- Differentiates ARDS from cardiogenic pulmonary edema (latter shows homogeneous bilateral B-lines with normal pleural line).
- Guides lung recruitment maneuvers and PEEP titration — LUS can demonstrate real-time aeration changes.
6. Pulmonary Embolism
- LUS itself cannot directly visualize emboli in central vessels, but subpleural wedge-shaped consolidations (triangular, pleura-based) suggest peripheral infarction.
- Combined with DVT ultrasound (bilateral leg compression), forms a bedside diagnostic package.
- Used within multimodal POCUS protocols (cardiac RV dilation, DVT + subpleural lesions) to raise pre-test probability.
The BLUE Protocol (Bedside Lung Ultrasound in Emergency)
The BLUE protocol is the most validated systematic algorithm for acute respiratory failure, achieving >90% diagnostic accuracy in the ICU:
| LUS Pattern | Diagnosis |
|---|---|
| Bilateral anterior A-lines + lung sliding + no DVT | Asthma / COPD |
| Bilateral anterior A-lines + lung sliding + DVT | Pulmonary embolism |
| Bilateral anterior B-lines (diffuse) | Pulmonary edema |
| Unilateral B-lines / anterior consolidation | Pneumonia |
| Absent lung sliding + A-lines ± lung point | Pneumothorax |
| Posterior consolidation / effusion | Pneumonia / pleurisy |
Interstitial Syndrome Pattern Summary
As described in the retrieved literature (Bedside Ultrasonography, p. 13):
| B-line Spacing | Pattern | Interpretation |
|---|---|---|
| 7 mm apart, well-defined | Regular interstitial syndrome | Interstitial lung disease |
| Irregularly spaced | Focal interstitial involvement | Pneumonia |
| < 3 mm apart, coalescent | White lung pattern | Pulmonary edema / confluent bronchopneumonia |
Advantages Over Conventional Imaging in Critical Care
| Feature | LUS | Chest X-ray | CT Chest |
|---|---|---|---|
| Radiation | None | Low | High |
| Portability | Fully bedside | Portable (limited) | Requires transport |
| Real-time guidance | Yes | No | No |
| Pneumothorax sensitivity (supine) | High | Low | Reference standard |
| Pleural effusion quantification | Yes | Approximate | Precise |
| Repeat monitoring | Unlimited | Limited | Very limited |
| Cost | Low | Low | High |
Limitations
- Operator-dependent: requires structured training; competence and experience significantly affect accuracy.
- Subcutaneous emphysema: air in soft tissue abolishes pleural visualization.
- Obesity / dressings: poor acoustic windows.
- Central pathology: central consolidation or mediastinal lesions are not accessible.
- Bony structures: ribs limit field of view; intercostal scanning is required.
- Evidence base for some patterns (e.g., B-line subtypes) contributed largely by single research groups — graded moderate quality evidence (Bedside Ultrasonography, p. 13).
Summary
Lung ultrasound is a powerful first-line diagnostic modality in critical care for:
- Pneumothorax (absent sliding + A-lines + lung point)
- Pulmonary edema (diffuse coalescent B-lines)
- Pneumonia / consolidation (hepatization + air bronchograms)
- Pleural effusion (anechoic/echogenic fluid + morphology characterization)
- ARDS (heterogeneous B-lines + subpleural consolidations)
- Pulmonary embolism (subpleural infarcts + DVT assessment)
Integrated with clinical assessment and cardiac POCUS, LUS forms the backbone of point-of-care ultrasound (POCUS) in the ICU and emergency department, enabling rapid, accurate, and repeatable diagnosis without radiation or patient transport.
This is a shared conversation. Sign in to Orris to start your own chat.