Bone and Cartillage from General Anatomy full chapter
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the core content and images. Let me compile the full chapter presentation.
Bone and Cartilage
General Anatomy and Musculoskeletal System - THIEME Atlas of Anatomy
1.7 Primordial Skeleton, Prenatal Skeletal Development, and Ossification Centers
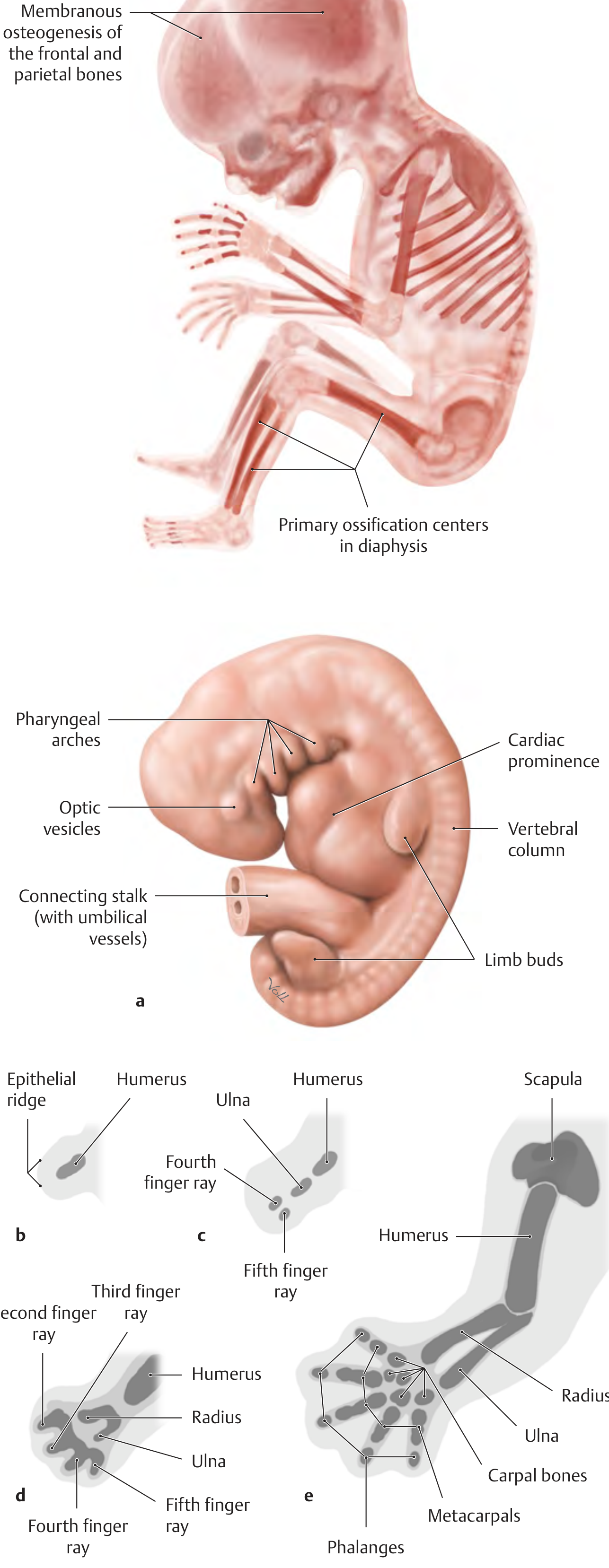
The supporting tissue of the human skeleton (mainly cartilage and bone tissue) arises from embryonic connective tissue (mesenchyme), derived from the middle germ layer (mesoderm). Mesenchymal cells initially differentiate into chondroblasts, which form a miniature model of the skeleton from hyaline cartilage - the "primordial skeleton." This cartilage template is later replaced by bone tissue - a process called endochondral osteogenesis, which forms the largest part of the human skeleton (torso, limbs, and skull base).
Timeline of ossification:
- Ossification of the primordial skeleton begins at the end of the 8th embryonic week
- Starts from primary ossification centers in the diaphyseal region of long bones (perichondral/desmal osteogenesis)
- Then endochondral ossification forms primary ossification centers in the diaphysis
- By the 12th week, ossification centers exist in all long bones
- Secondary ossification centers (in the epiphyses) only appear after birth - exception: the distal femur and proximal tibial epiphysis exist at birth
- At birth, most tarsal bones and all carpal bones are entirely cartilaginous
- Only the bones of the cranial roof, parts of the facial bones, and the clavicle ossify directly (membranous osteogenesis - mesenchyme cells become osteoblasts directly)
Limb development: Limb buds appear at the end of the 4th embryonic week as paddle-shaped outpouches of the lateral trunk. The humerus develops first, followed by the ulna, then the radial and carpal elements. Fingers and toes form through interdigital apoptosis - programmed cell death separating the five rays. Failure of apoptosis causes syndactyly (fused digits). Absence of entire limbs = amelia; partial absence = meromelia.
Note: Achondroplasia - a genetic disorder disrupting endochondral ossification - is one of the most frequent causes of disproportionate short stature (short limbs, large skull). Cell division and maturation of chondrocytes in the growth plates is disrupted, meaning all bones produced by endochondral osteogenesis are affected.
1.8 Bone Development and Remodeling
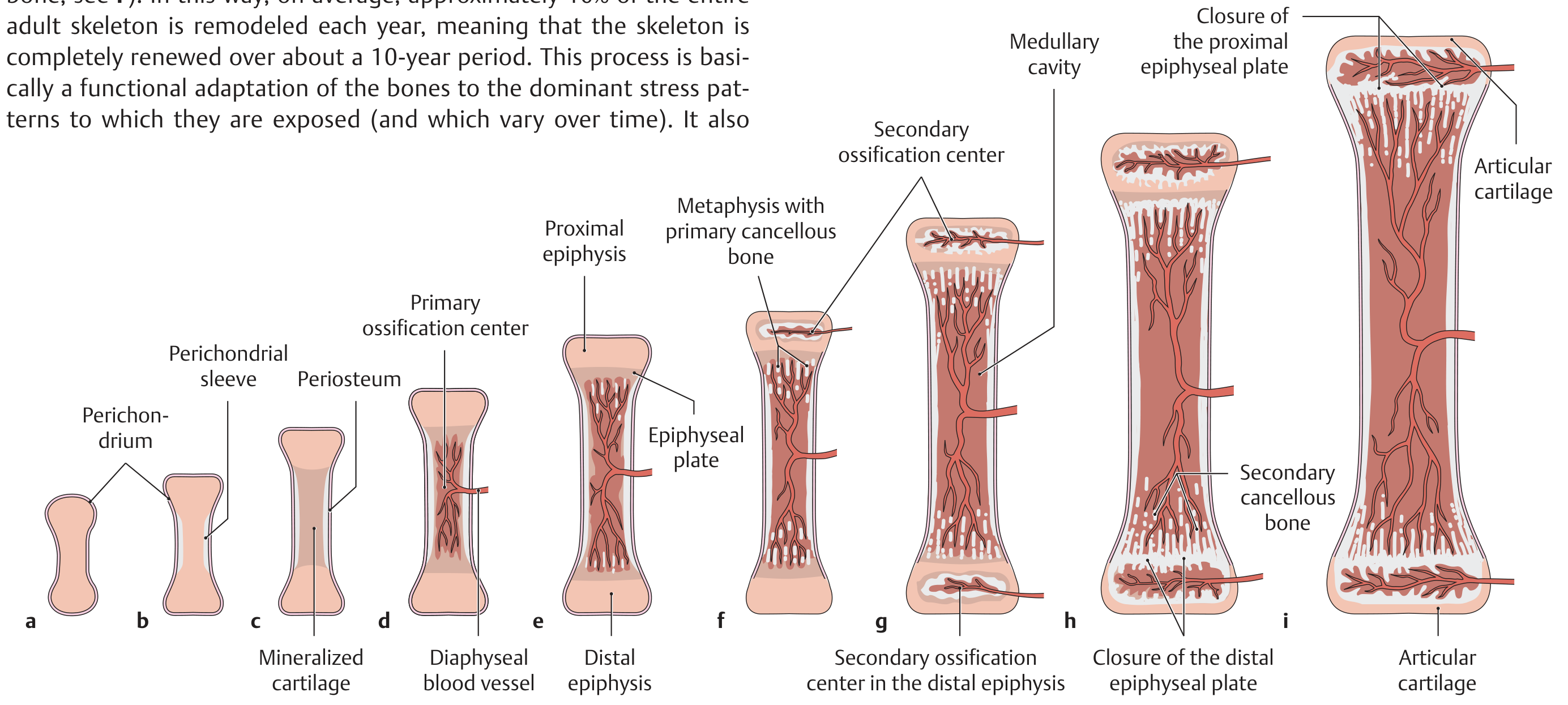
Bone development and remodeling are closely interrelated. During growth, immature woven bone (fiber bone) is constantly replaced by lamellar bone. In the mature skeleton, approximately 10% of the entire adult skeleton is remodeled each year - the skeleton is completely renewed over roughly a 10-year period. This process is a functional adaptation to dominant stress patterns. It also prevents material fatigue, repairs microinjuries, and provides a rapidly available source of calcium.
A - Development of a Long Bone (Endochondral Osteogenesis)
Long bones (humerus, tibia, etc.) form primarily by indirect bone formation - replacing a pre-existing cartilaginous model. However, portions still form by direct bone formation (the perichondrial bone collar allowing growth in thickness).
| Stage | Event |
|---|---|
| a | Cartilaginous model of bone in embryonic skeleton |
| b | Formation of a perichondrial bone collar (directly from mesenchyme) |
| c | Differentiation to hypertrophic chondrocytes; mineralization of cartilaginous ECM |
| d | Ingrowth of a diaphyseal vessel; formation of a primary ossification center |
| e | Development of proximal and distal growth centers (epiphyseal plates) |
| f | Appearance of the proximal epiphyseal ossification center (secondary ossification center) |
| g | Formation of the distal epiphyseal ossification center |
| h | Closure of the distal epiphyseal plate |
| i | Closure of the proximal epiphyseal plate (end of skeletal growth, ~18-23 years for most tubular bones) |
Key distinction: Osteogenesis = formation of an individual bone. Ossification = formation of bone tissue.
B - Structure of the Epiphyseal Plate
The epiphyseal plate (growth plate) has distinct zones from deep to superficial:
- Resting zone - reserve cartilage, adjacent to secondary ossification center
- Proliferative zone - active cell division, chondrocytes arranged in columns
- Hypertrophic zone - enlarged chondrocytes, matrix mineralization
- Zone of calcified cartilage - mineralized matrix, vascular invasion
- Zone of ossification - osteoblasts deposit bone on calcified cartilage scaffolding
C - Two Pathways of Osteogenesis (Schematic)
Membranous (direct) osteogenesis:
Mesenchymal fibrous tissue → directly to woven bone → membranous bone formation (positional growth in thickness)
Endochondral (indirect) osteogenesis:
Hyaline cartilage → woven bone → functional remodeling (in response to greater stresses, e.g., increasing body weight) → Lamellar (mature) bone
Note: Most bones form by indirect osteogenesis. The few exceptions (clavicle, bones of the calvaria) still have portions that develop from direct mesenchyme transformation.
D - Development of an Osteon (after Hees)
The process of functional remodeling begins when blood vessels and osteoclasts invade woven bone:
- a Longitudinal section through a resorption canal (osteoclasts drill a vascularized channel equal in diameter to the future osteon)
- b Cross section at the resorption canal level
- c Transformation zone: osteoprogenitor cells → osteoblasts
- d Osteogenic zone: osteoblasts produce bony lamellae concentrically around the vascular canal
- e Newly formed osteon
F - Growth and Remodeling in Cancellous (Lamellar) Bone
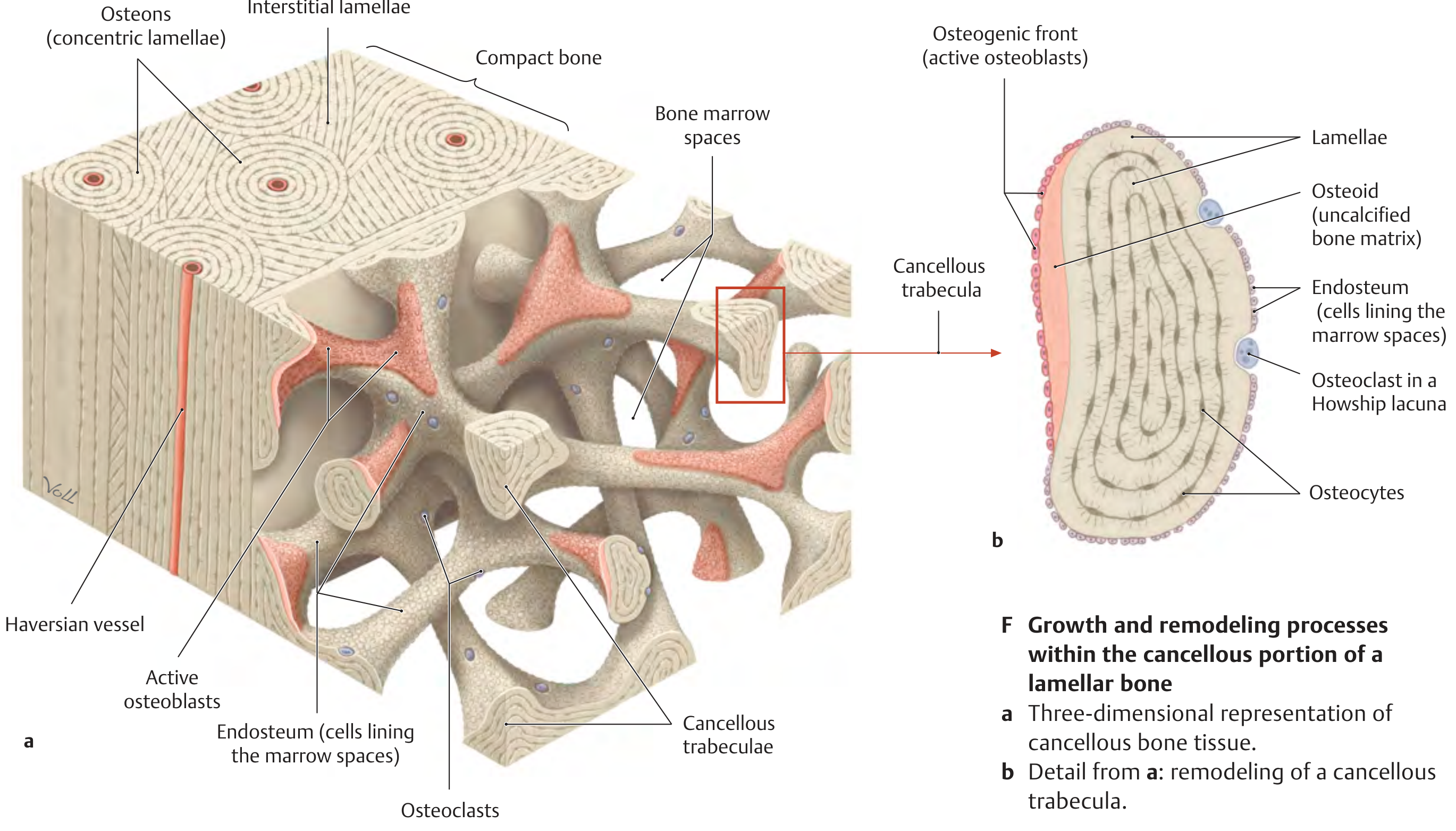
Cancellous trabeculae have no direct vascular supply - they are nourished by diffusion from the adjacent medullary cavity. This limits their thickness to only about 200-300 µm. Remodeling of a trabecula involves:
- Osteoclasts sitting in Howship lacunae, resorbing bone
- Osteoid (uncalcified bone matrix) laid down by osteoblasts
- Endosteum lining the marrow spaces
- Osteocytes embedded in lamellae, connected by cytoplasmic processes
4.1 The Bony Skeleton and Structure of Tubular Bones
C - Types of Bone
| Type | Examples |
|---|---|
| Long bones (tubular) | Limb bones (femur, humerus, tibia, etc.) |
| Short bones | Carpal and tarsal bones |
| Flat bones | Scapula, ilium, bones of the calvaria |
| Irregular bones | Vertebrae |
| Pneumatic bones | Facial skeleton and paranasal sinuses (air-filled) |
| Sesamoid bones | Patella (incorporated in tendons) |
| Accessory bones | Anomalous supernumerary bones (calvaria and foot); result from failure of fusion of certain ossification centers |
D - Structure of a Typical Tubular Bone (illustrated for the Femur)
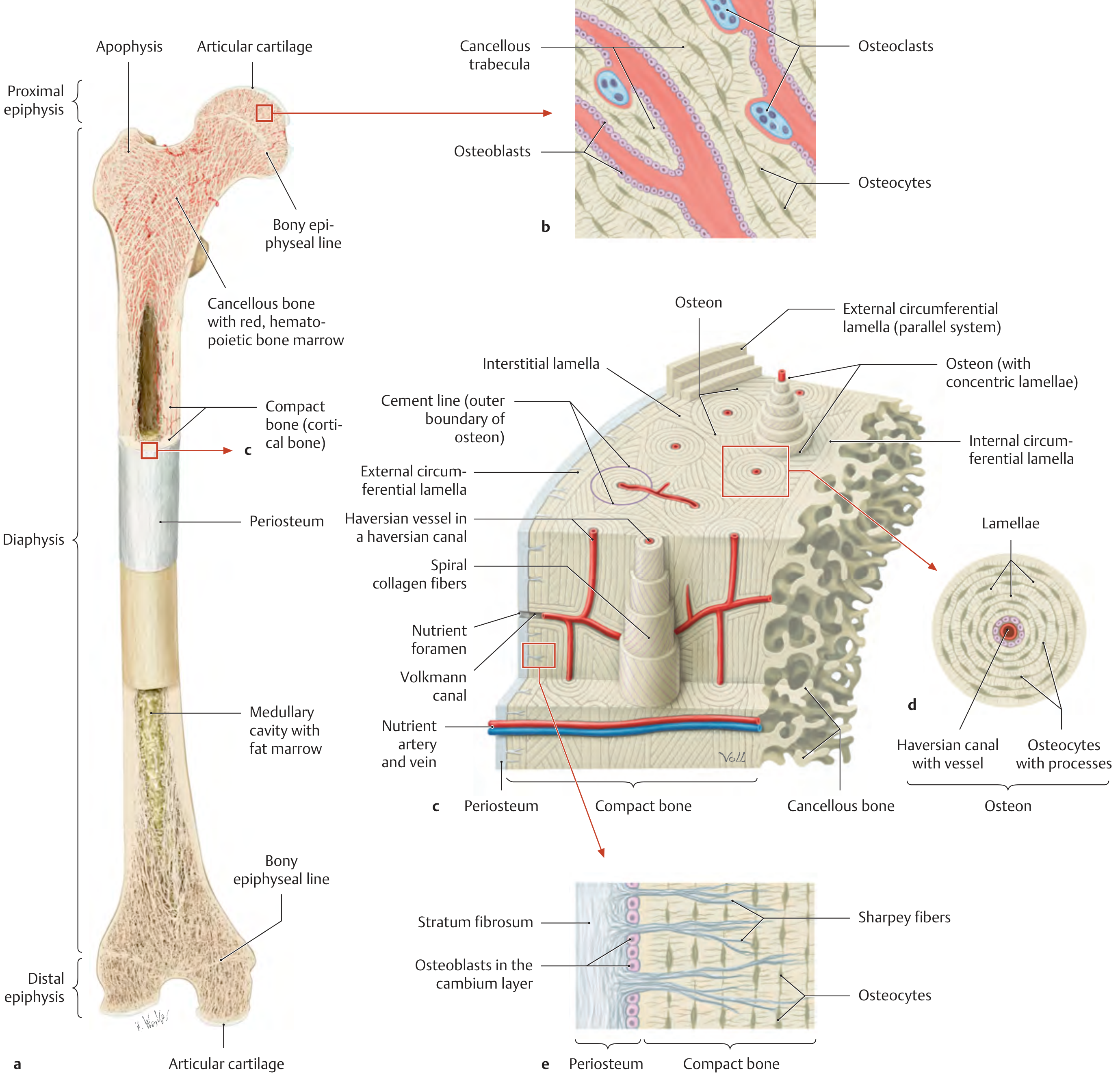
Gross structure:
- Proximal and distal epiphyses - covered by articular cartilage; contain cancellous bone with red (hematopoietic) bone marrow; the bony epiphyseal line marks where the growth plate closed
- Diaphysis - the shaft; contains the medullary cavity (yellow/fat marrow in adults) surrounded by compact bone
- Apophysis - a bony projection (non-articular eminence) at the epiphysis
Cancellous (spongy) bone (section b):
- Lamellar architecture with trabeculae arranged like plywood contiguous plates
- Nourished by diffusion from the medullary cavity
- Trabeculae are ~200-300 µm thick
- Contains active osteoblasts and osteoclasts on trabecular surfaces
Compact bone (section c - 3D diagram):
- Structural units = osteons (~1 cm long, 250-350 µm diameter)
- Each osteon has a central Haversian canal (longitudinally oriented, carries vessels)
- Haversian canals are interconnected by short transverse/oblique Volkmann canals and also connect to vessels of the periosteum and medullary cavity
- Each osteon: central Haversian canal surrounded by ~5-20 concentric lamellar systems of osteocytes + ECM
- Osteocytes are interconnected by numerous fine cytoplasmic processes
- Interstitial lamellae = remnants of old osteons between new ones
- External/internal circumferential lamellae = parallel lamellae at the outer and inner surfaces
Periosteum (section e):
- Stratum fibrosum (outer fibrous layer) - dense connective tissue
- Cambium layer (inner layer) - contains osteoblasts
- Sharpey fibers - collagen fibers that anchor the periosteum into the bone matrix
4.4 True Joints: Structure of the Joint Capsule and Hyaline Cartilage
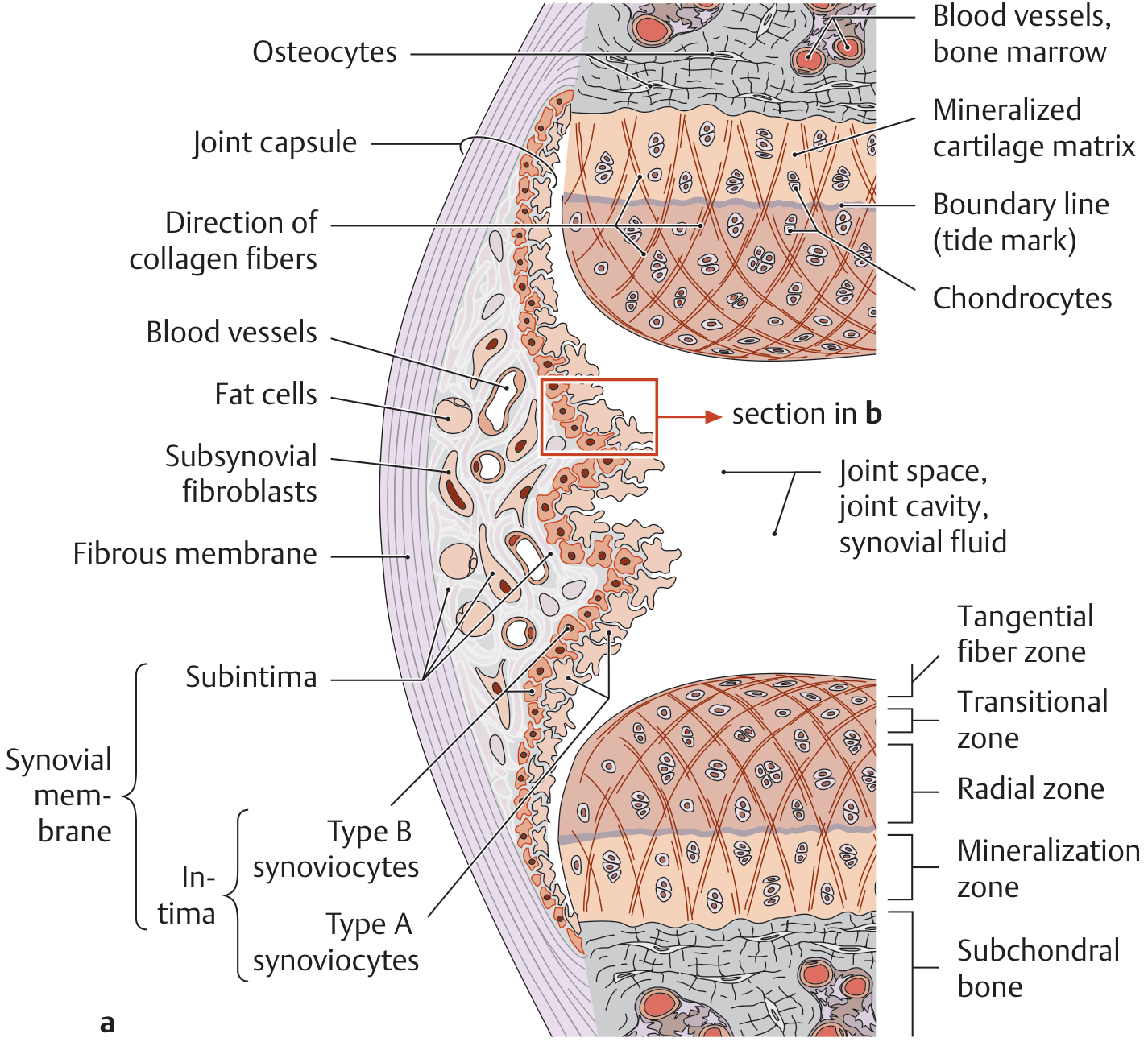
The joint cavity of true joints is enclosed by a joint capsule with two distinct layers:
Joint Capsule Layers
Fibrous membrane (outer layer - Stratum fibrosum):
- Dense connective tissue
- Reinforced by ligaments
- Mechanically stabilizes the joint
Synovial membrane (inner layer - Stratum synoviale):
- Intima (innermost layer): contains 1-3 layers of synoviocytes:
- Type A synoviocytes - macrophage-like, phagocytic
- Type B synoviocytes - fibroblast-like, secrete synovial fluid components
- Subintima: loose connective tissue containing fat cells, blood vessels, subsynovial fibroblasts
- Produces synovial fluid (viscous, rich in hyaluronic acid) for lubrication and cartilage nutrition
Key clinical note: The synovial membrane can regenerate into old age, even after complete removal (synovectomy - necessary in cases of chronic rheumatoid arthritis). The hyaline cartilage, however, cannot regenerate.
Synovial reactions: The synovial membrane reacts to stimuli by increased secretion (articular effusion). Depending on the stimulus:
- Mechanical or allergic: clear, thin effusion
- Infectious: turbid, pus-filled
- Injury (e.g., cruciate ligament rupture): hemarthrosis (bloody effusion)
- Pain results from overstretching of the joint capsule and release of inflammatory mediators (prostaglandins, histamine, bradykinin, cytokines)
Hyaline Cartilage
With the exception of the jaw (TMJ) and sternoclavicular joint (which are covered by fibrous cartilage), all articular surfaces are covered by hyaline cartilage. Its thickness ranges from:
- 1-2 mm in phalangeal joints
- 5-7 mm in the femoropatellar joint
Hyaline cartilage consists of:
- Extracellular matrix (ECM): ~95% of volume - water, collagen type II, proteoglycans
- Chondrocytes: ~5% of volume
Zones of hyaline cartilage (determined by the arcade-like collagen fibril arrangement):
| Zone | Description |
|---|---|
| Zone I (tangential) | Collagen fibrils run parallel to the surface; chondrocytes flattened |
| Zone II (transitional) | Fibrils transition, chondrocytes rounded |
| Zone III (radial) | Collagen fibrils run almost vertically (radially); columns of chondrocytes |
| Zone IV (mineralization) | Calcified cartilage, connected to subchondral bone; the tide mark (boundary line) separates zones III and IV |
| Subchondral bone | The underlying bone plate |
Collagen fibril details: Visible only under transmission electron microscopy. In light microscopy they appear "masked" (refractive index matches surroundings). After enzymatic liberation with hyaluronidase, TEM shows empty "cartilage holes" surrounded by a thick collagen fibril mesh.
Proteoglycans - Aggrecan: The most important proteoglycan of hyaline cartilage. Aggrecan consists of a core protein with multiple glycosaminoglycan (GAG) chains (chondroitin sulfate and keratan sulfate) that bind to a hyaluronan backbone via link proteins, forming huge aggregates that attract water and give cartilage its compressive stiffness.
Biphasic viscoelastic model (after Mow): Hyaline cartilage behaves as a biphasic material:
- Solid phase = collagen fibril network + proteoglycans
- Fluid phase = interstitial water Under compression, fluid is squeezed out; upon release, it flows back in. This biphasic behavior accounts for the viscoelastic (time-dependent) properties of cartilage.
Important limitation: Hyaline cartilage (outside the primordial skeleton) has no perichondrium and no blood vessels. Chondrocytes must be nourished exclusively by synovial fluid (via diffusion and convection). This is why hyaline cartilage has virtually no regenerative capacity following injury - a major reason articular cartilage defects progress to osteoarthritis.
1.9 Ossification of the Limbs
Epi- and apophyseal ossification centers follow a predictable timetable:
Upper limb ossification centers (approximate timing):
- Appear at different times (fetal months through postnatal years)
- Females typically ossify earlier than males
- Synostosis (closure) also occurs earlier in females
Lower limb:
- Distal femoral and proximal tibial epiphyseal ossification centers are present at birth (unique among epiphyseal centers)
- Other lower limb centers appear in the months/years following birth
1.10 Basic Skeletal Structure and Position of the Limbs
The human limb follows the basic pentadactyl tetrapod pattern:
| Segment | Name | Upper Limb | Lower Limb |
|---|---|---|---|
| Proximal | Stylopodium | Arm - Humerus | Thigh - Femur |
| Middle | Zygopodium | Forearm - Radius + Ulna | Leg - Tibia + Fibula |
| Distal | Autopodium | Hand | Foot |
| - | Basipodium | Carpus | Tarsus |
| - | Metapodium | Metacarpals | Metatarsals |
| - | Acropodium | Phalanges | Phalanges |
Common congenital malformations:
- Polydactyly - extra digits
- Syndactyly - fused digits (failure of interdigital apoptosis)
Source: General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy (ISBN 9781626237186)
This is a shared conversation. Sign in to Orris to start your own chat.