Histology of astrocytoma, Glioblastoma Oligodendroglioma, medulloblastoma, Meningioma Easy ways to remember
Brain Tumor Histology - Quick Reference with Memory Tricks
1. ASTROCYTOMA (IDH-mutant, Grade 2-4)
Histology
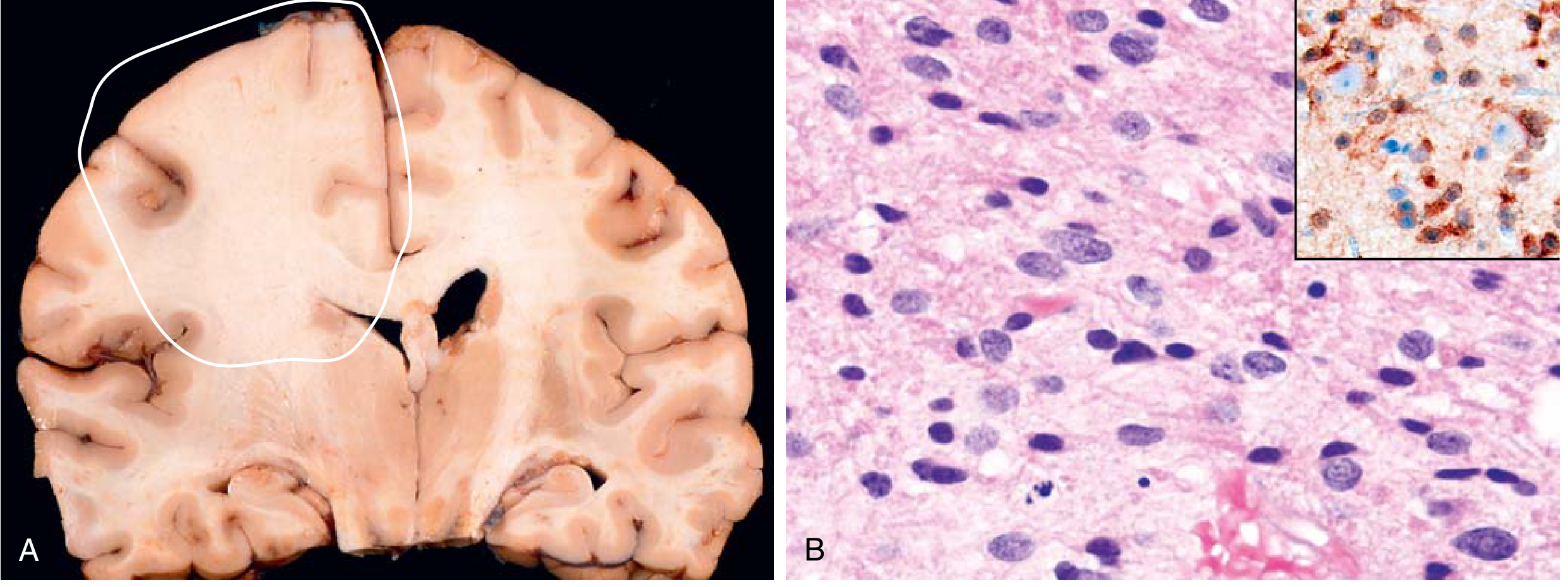
- Gross: Poorly defined, gray, infiltrative mass - no discrete border. Expands without forming a nodule
- Micro (Grade 2): Mild to moderate increase in glial nuclei; nuclear pleomorphism; background has a fibrillary (cobweb-like) appearance from GFAP-positive astrocytic processes
- Micro (Grade 3): Denser cellularity + mitotic figures
- Micro (Grade 4 IDH-mutant): Cytological atypia, brisk mitoses, microvascular proliferation and/or necrosis - but less hemorrhage than GBM
- IHC: GFAP-positive; IDH1 mutant immunostain positive (shown in inset)
🧠 Memory Trick
"A for Astrocytes = A for Airy fibrillar background" Grade 2 = Fine fibers, few nuclei | Grade 3 = add Mitoses | Grade 4 = add Necrosis + Vessels IDH-mutant = better prognosis than GBM (think: IDH = I'm Doing better)
2. GLIOBLASTOMA (GBM, IDH-wild type, WHO Grade 4)
Histology
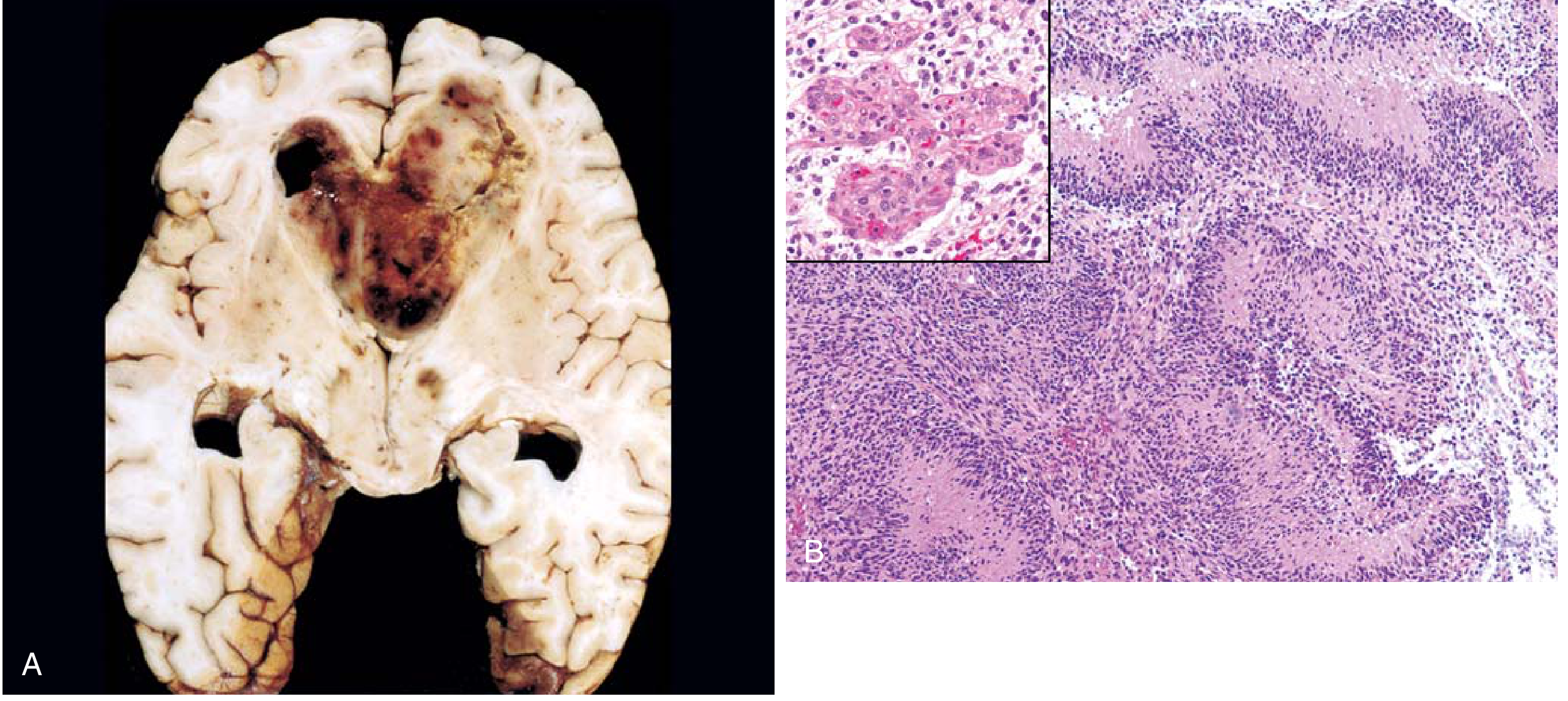
- Gross: Variegated - firm white areas + soft yellow necrotic areas + cystic/hemorrhagic zones = "butterfly glioma" when crosses corpus callosum
- Micro (the 4 hallmarks):
- High cellularity - pleomorphic, poorly differentiated cells
- Nuclear atypia + brisk mitotic activity
- Palisading necrosis - serpiginous (zigzag) bands of necrosis with tumor nuclei lined up ("palisaded") around the dead zones
- Microvascular (endothelial) proliferation - glomeruloid tufts of vessels
🧠 Memory Trick
"GBM = Gone Bad Maximally" - the 4 H's: High cellularity + Hemorrhage/necrosis + Hyperplastic vessels + HyperatypiaPalisading necrosis = think of soldiers in a trench (palisades) surrounding a war zone of dead cellsMGMT = Makes GBM Mild To chemo (methylated = responds to temozolomide)
3. OLIGODENDROGLIOMA (IDH-mutant + 1p/19q-codeleted, Grade 2-3)
Histology
- Gross: Gelatinous gray mass; may show cysts, hemorrhage, and calcification
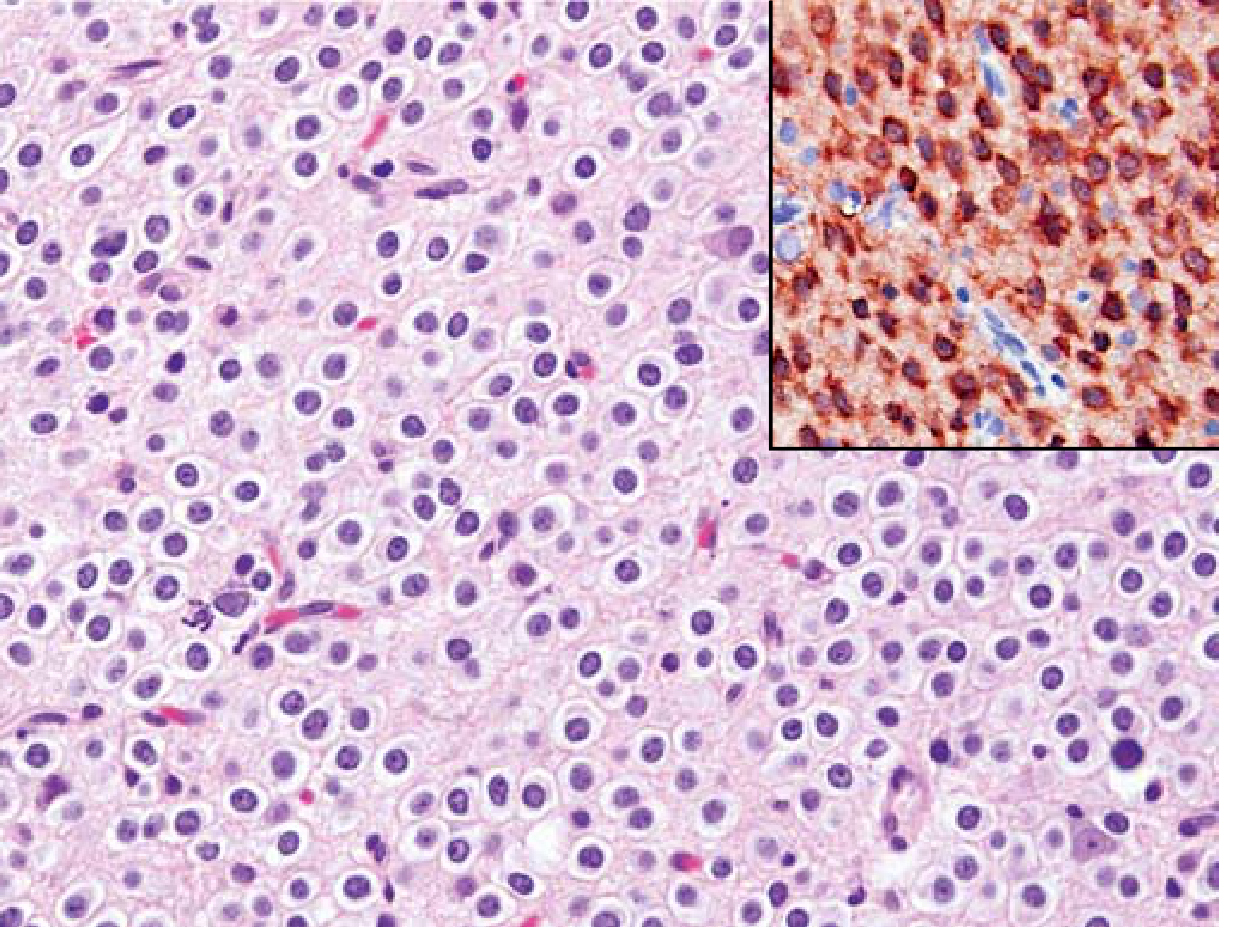
- Micro (the 3 hallmarks):
- "Fried egg" cells - round nuclei with clear cytoplasmic halo (artifact of formalin fixation)
- "Chicken-wire" vascular pattern - delicate anastomosing capillary network
- Calcification in up to 90% of cases (ranges from microscopic to massive)
- Mitotic activity is usually low (grade 2); grade 3 adds nuclear anaplasia, increased mitoses, microvascular proliferation
🧠 Memory Trick
"OLIGO = Old Looking Fried Egg Cells"Remember the 3 C's of oligodendroglioma: Clear halos (fried egg) + Chicken-wire vessels + Calcification1p/19q codeletion = the chromosomes are "deleted like the first and last" parts of 19 = 1p (first arm) and 19q (last chromosome arm listed)
4. MEDULLOBLASTOMA (WHO Grade 4)
Histology
- Gross: Well-circumscribed, gray, friable mass in cerebellar midline; may extend to leptomeninges; "drop metastases" via CSF
- Micro:
- Classic "small blue cell" tumor - densely cellular sheets of monomorphic cells
- Small cells with little cytoplasm, hyperchromatic nuclei, abundant mitoses
- Homer-Wright rosettes - primitive tumor cells arranged in a circle surrounding central neuropil (pink tangled neuronal processes) - NO lumen (differentiates from ependymoma)
- Neuronal markers positive (synaptophysin, NeuN); GFAP usually negative
- Drop metastases to spinal cord via CSF seeding

🧠 Memory Trick
"MedulloBLASToma = BLAST of small blue cells in the BACK (cerebellum)"Homer-Wright rosette = Homer (from Homer Simpson) sits around a donut with PINK filling (neuropil, no lumen)Contrast: Ependymoma rosettes have a LUMEN (true rosette) + perivascular pseudorosettesRadiosensitive = think "medulloBLAST was BLASTED by radiation" (exquisitely sensitive)CSF spread = "DROP" metastases - drops of tumor fall down the spine
5. MENINGIOMA (WHO Grade 1, 2, 3)
Histology
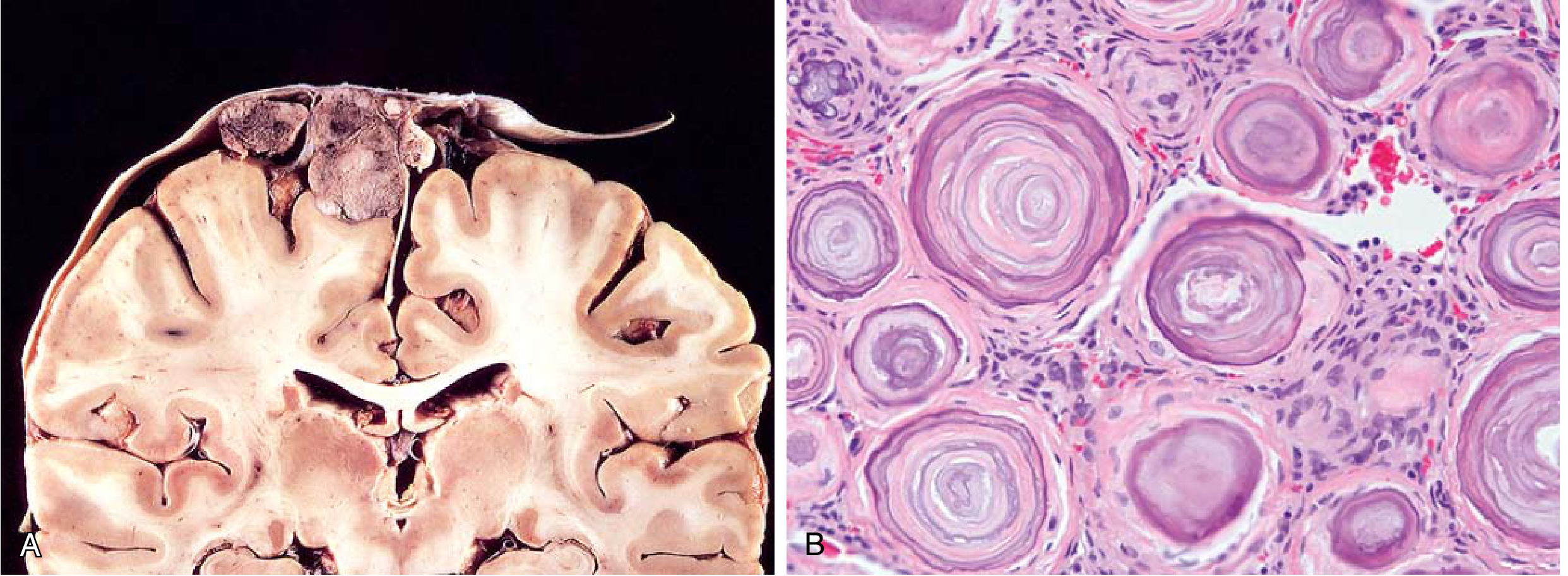
- Gross: Well-defined, lobulated, dura-based mass that compresses but does NOT invade the brain; may show hyperostosis of overlying bone
- Micro (key subtypes):
Subtype Key Feature Meningothelial Syncytium-like lobules, cells with no visible membranes Fibroblastic Elongated cells + abundant collagen Transitional Mix of meningothelial + fibroblastic Psammomatous Multiple psammoma bodies (concentric calcified rings) Secretory PAS-positive eosinophilic glandular material - Whorled pattern of cell growth is characteristic
- Psammoma bodies = concentrically laminated calcifications ("onion-skin rings")
🧠 Memory Trick
"MeninGIOMA = sits on the DURA like a G.I. (general) on a throne, squishing the brain below"Psammoma bodies = think "Psammo = Sand" (from Greek psammos = sand) - calcified whorls that look like sand dollarsWHIRL = the key word: whorled cells + psammoma bodies (whorled calcifications)Grade 2 = Brain invasion or chordoid/clear cell subtype | Grade 3 = looks like sarcoma/carcinoma
Quick-Reference Comparison Table
| Tumor | Hallmark Feature | Memory Hook |
|---|---|---|
| Astrocytoma | Fibrillary background, GFAP+, infiltrative | "Airy/Fibrillar" background |
| GBM | Palisading necrosis + microvascular proliferation | "Palisade + Glomeruloid vessels" |
| Oligodendroglioma | Fried egg + chicken-wire + calcification | "3 C's: Clear halo, Chicken-wire, Calcification" |
| Medulloblastoma | Small blue cells + Homer-Wright rosettes | "Blue BLAST + Homer's Pink donut" |
| Meningioma | Whorled cells + psammoma bodies | "WHIRL + Sand dollars" |
Rosette Cheat Sheet (Easy Confusion!)
| Rosette | Tumor | Center Content |
|---|---|---|
| Homer-Wright | Medulloblastoma, Neuroblastoma | Neuropil (pink fibers) - NO lumen |
| True (Flexner-Wintersteiner) | Retinoblastoma, Ependymoma | Central lumen |
| Perivascular pseudorosette | Ependymoma | Fibrillary processes radiating to a blood vessel |
Trick: "Homer Wright = Pink neuropil, NO hole" / "True rosette = TRUE lumen/hole"
Create a visual poster comparing these 5 tumors side-by-side
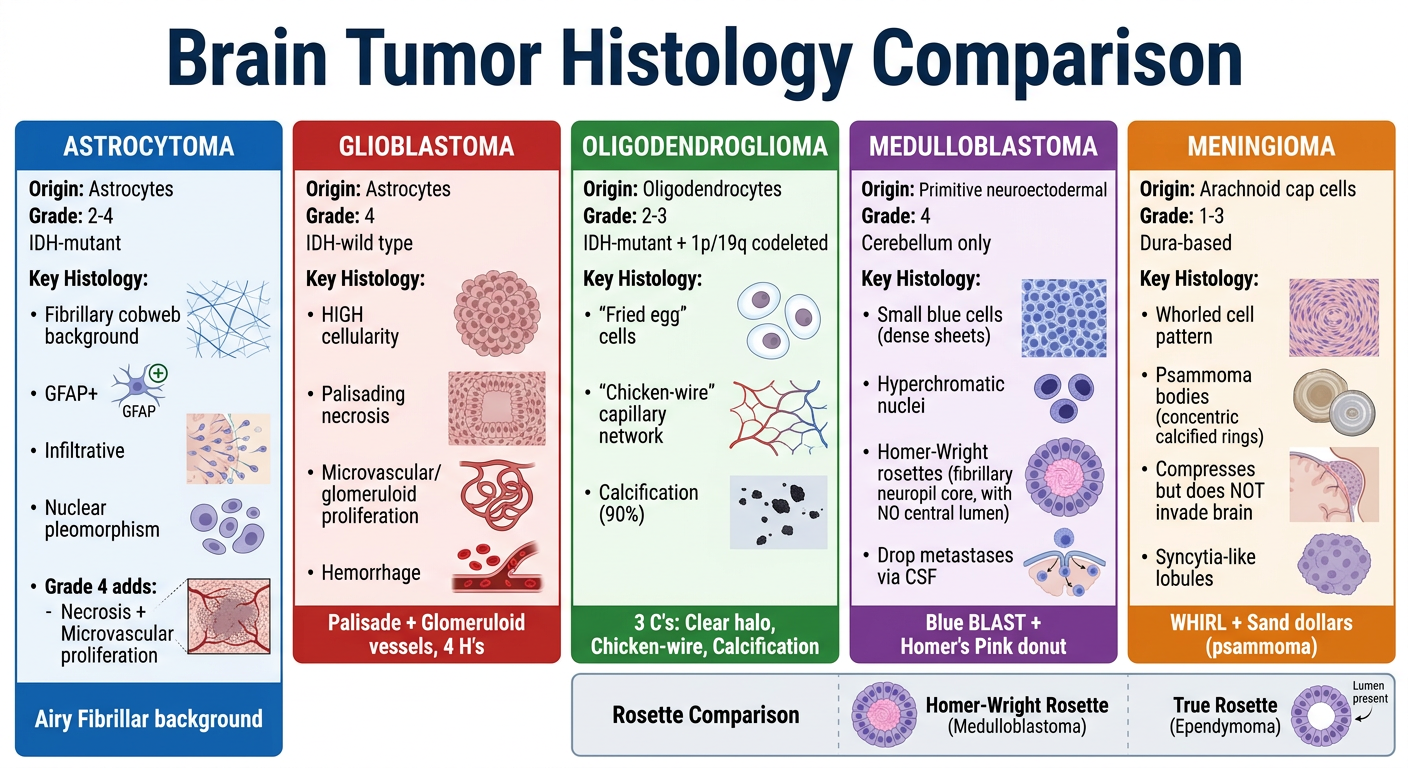
A clean, professional medical education poster titled "Brain Tumor Histology Comparison" comparing 5 tumors side by side in 5 columns. Each column has a distinct color header. The columns are: 1. ASTROCYTOMA (blue header) - Origin: Astrocytes, Grade 2-4, IDH-mutant. Key histology: Fibrillary cobweb background, GFAP+, infiltrative, nuclear pleomorphism. Grade 4 adds necrosis + microvascular proliferation. Mnemonic: "Airy Fibrillar background" 2. GLIOBLASTOMA (red header) - Origin: Astrocytes, Grade 4, IDH-wild type. Key histology: HIGH cellularity, Palisading necrosis (tumor cells lining up around necrosis), Microvascular/glomeruloid proliferation, Hemorrhage. Mnemonic: "Palisade + Glomeruloid vessels, 4 H's" 3. OLIGODENDROGLIOMA (green header) - Origin: Oligodendrocytes, Grade 2-3, IDH-mutant + 1p/19q codeleted. Key histology: "Fried egg" cells (round nuclei + clear cytoplasmic halo), "Chicken-wire" capillary network, Calcification (90%). Mnemonic: "3 C's: Clear halo, Chicken-wire, Calcification" 4. MEDULLOBLASTOMA (purple header) - Origin: Primitive neuroectodermal, Grade 4, Cerebellum only. Key histology: Small blue cells (dense sheets), Hyperchromatic nuclei, Homer-Wright rosettes (pink neuropil center, NO lumen), Drop metastases via CSF. Mnemonic: "Blue BLAST + Homer's Pink donut" 5. MENINGIOMA (orange header) - Origin: Arachnoid cap cells, Grade 1-3, Dura-based. Key histology: Whorled cell pattern, Psammoma bodies (concentric calcified rings), Compresses but does NOT invade brain, Syncytia-like lobules. Mnemonic: "WHIRL + Sand dollars (psammoma)" At the bottom: a small comparison row for Rosettes: Homer-Wright = neuropil no lumen (Medulloblastoma) vs True rosette = lumen (Ependymoma). Layout: clean white background, each tumor in its own column with colored headers, icons or small diagrams of cell shapes where possible, bold mnemonics in colored boxes at the bottom of each column. Medical textbook style, clear fonts, well-organized, suitable for exam revision.
- Origin, grade, and molecular marker for each
- Key histological hallmarks (palisading necrosis, fried egg cells, Homer-Wright rosettes, psammoma bodies, fibrillary background)
- Mnemonics highlighted at the bottom of each column
- Rosette comparison row at the bottom to avoid the classic Homer-Wright vs. true rosette confusion
Verocay bodies
Verocay Bodies
What they are
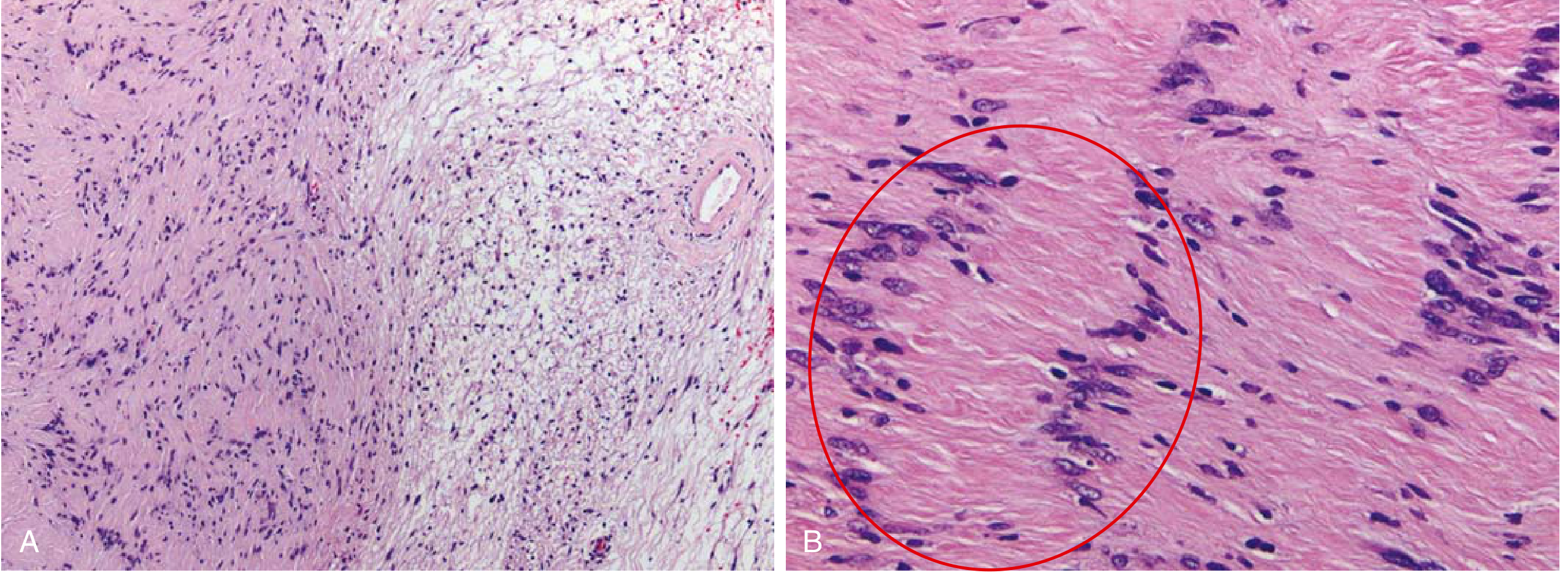
- Two parallel rows of palisaded Schwann cell nuclei arranged in double rows facing each other
- Flanking an acellular eosinophilic center made of tangled cytoplasmic processes (not a true lumen - no secretion, no blood vessel)
The Full Schwannoma Picture
| Zone | Name | Appearance |
|---|---|---|
| Dense, cellular | Antoni A | Spindle cells in fascicles, nuclear palisading, Verocay bodies |
| Loose, hypocellular | Antoni B | Spindle cells in myxoid matrix, edema, hyalinized vessels, no Verocay bodies |
- Well-encapsulated (EMA-positive capsule from perineurium)
- Axons excluded from tumor (unlike neurofibromas, which trap axons within)
- GFAP-negative; S100-positive and SOX10-positive
- Mitoses absent or very rare
- Hyalinized (thick-walled) blood vessels in Antoni B areas
IHC
| Marker | Schwannoma | Neurofibroma |
|---|---|---|
| S100 | Diffuse + | Focal + |
| SOX10 | + | + |
| Axons within tumor | Absent | Present |
| Verocay bodies | Present | Absent |
| Encapsulation | Yes | No (except localized) |
Associations
- Sporadic: Most cases (single tumor)
- NF2 (Neurofibromatosis Type 2): Bilateral vestibular schwannomas are the hallmark - caused by loss-of-function mutation in merlin gene on chromosome 22
- Most common cranial nerve affected: CN VIII (vestibular branch) - causing hearing loss
🧠 Memory Trick
"VERo = VERtical rows" - Verocay bodies = two vertical rows of nuclei facing each other like a mirrorAntoni A = Active/dense = pAliSAding (Verocay) | Antoni B = Bland/loose = B for Background"SCHWANN cells SCHWING back and forth in palisades" - they line up in rows, creating the alternating dark (nuclear) and light (acellular) bandsVerocay ≠ Homer-Wright: Verocay has NO central fibers (just cytoplasmic processes); Homer-Wright has neuropil (pink fibers) in center