Strep a throat infection treatment
Reading File
Finding Sources
Searching PubMed
"streptococcal pharyngitis"[MeSH Terms] AND "treatment"[MeSH Terms]
Finding Sources
Searching PubMed
"group A streptococcus" AND "pharyngitis" AND "antibiotic"
Finding Sources
Searching the Web
Group A strep throat treatment guidelines 2024 2025 antibiotics
Reading File
Reading File
Here is a comprehensive overview of Group A Streptococcal (GAS) pharyngitis treatment based on authoritative textbooks (Harrison's 2025, Red Book 2021, IDSA guidelines) and current CDC guidance.
Group A Strep (GAS) Pharyngitis — Treatment
Diagnosis First
Treat only confirmed GAS pharyngitis. Most pharyngitis is viral — antibiotics should not be given without a positive Rapid Antigen Detection Test (RADT) or throat culture. In children (3–14 years), a negative RADT should be followed by a throat culture. In adolescents and adults, a negative RADT generally does not require culture confirmation, as acute rheumatic fever is rare in these age groups.
Antibiotic Treatment
First-Line (No Penicillin Allergy)
| Antibiotic | Dose | Duration |
|---|---|---|
| Penicillin V (oral) | Adults: 500 mg twice daily or 250 mg 4×/day | 10 days |
| Children: 250 mg 2–3×/day | 10 days | |
| Amoxicillin (oral) | Adults: 500 mg twice daily or 1,000 mg once daily | 10 days |
| Children: 50 mg/kg/day once daily (max 1,000 mg) | 10 days | |
| Benzathine Penicillin G (IM) | <27 kg: 600,000 units IM; ≥27 kg: 1,200,000 units IM | Single dose |
Penicillin is the drug of choice — no clinical GAS isolate has ever been reported resistant to penicillin or cephalosporins. Amoxicillin is preferred in children due to its palatable liquid form. IM benzathine penicillin G is useful when adherence to a 10-day oral course is a concern.
Penicillin-Allergic Patients
| Allergy Type | Antibiotic | Dose | Duration |
|---|---|---|---|
| Non-anaphylactic | Cephalexin | 500 mg twice daily | 10 days |
| Cefadroxil | 1 g once daily | 10 days | |
| Severe/anaphylactic | Clindamycin | 7 mg/kg 3×/day (max 300 mg/dose) | 10 days |
| Azithromycin | 12 mg/kg once daily (max 500 mg) | 5 days | |
| Clarithromycin | 7.5 mg/kg twice daily (max 250 mg/dose) | 10 days | |
| Erythromycin | 250 mg 4×/day | 10 days |
⚠️ Macrolide resistance (azithromycin, clarithromycin) is increasing locally — check regional resistance patterns before prescribing. There is no role for metronidazole.
Why 10 Days?
Unlike many infections where shorter courses are now acceptable, streptococcal pharyngitis requires the full 7–10 day course. Shorter regimens are less effective at eradicating GAS and risk incomplete treatment.
Symptomatic/Supportive Care
- Analgesics: Acetaminophen or NSAIDs for pain and fever
- Saline gargles, humidification, soft foods, honey in tea
- Glucocorticoids (e.g., dexamethasone): NOT recommended — may reduce pain briefly at 24h but do not reduce absenteeism, relapse rates, and even short courses carry risks of sepsis, GI bleeding, VTE, and fracture
Goals of Antibiotic Treatment
- Shorten symptom duration (symptoms typically resolve in 3–5 days even without treatment)
- Prevent acute rheumatic fever (ARF) — the most critical reason to treat
- Prevent suppurative complications (peritonsillar abscess, otitis media, mastoiditis)
- Reduce transmission (person is non-contagious after 12–24h of antibiotics)
When to Seek Further Evaluation
Return if any of the following develop:
- Rigors (shaking chills)
- Neck swelling beyond simple lymphadenopathy
- Difficulty swallowing or drooling (suggests peritonsillar abscess)
- Symptoms that persist beyond 5 days without improvement or improve then worsen
Recurrent/Treatment-Failure GAS
For patients who fail penicillin or have recurrent infections:
- Clindamycin (oral, 10 days) — preferred
- Amoxicillin-clavulanate (oral, 10 days)
- Penicillin + rifampin (last 4 days of the penicillin course)
Sources: Harrison's Principles of Internal Medicine 22e (2025), Red Book 2021, CDC GAS Pharyngitis Guidance, IDSA 2025 Guidelines, IDSA/AAFP dosing tables.
When to use cefpodoxime for throat infection
Finding Sources
Searching the Web
cefpodoxime strep throat pharyngitis when to use guidelines
Cefpodoxime is not a first-line drug for GAS throat infections — it has specific, limited indications. Here's exactly when to reach for it:
When to Use Cefpodoxime for GAS Pharyngitis
1. Penicillin Allergy with History of Anaphylaxis (Type 1 / IgE-mediated)
For patients with a severe/immediate hypersensitivity to penicillin (anaphylaxis, urticaria, angioedema), oral cephalosporins with a dissimilar side chain — cefdinir or cefpodoxime — are preferred over cephalexin/cefadroxil.
- Cephalexin carries ~2.5% cross-reactivity risk with first-gen cephalosporins in this group, so it should be avoided.
- Cefpodoxime (3rd-gen) has a structurally different side chain, making it safer in true penicillin anaphylaxis.
- Dose: 100–200 mg twice daily × 5–10 days
2. Recurrent or Treatment-Failure GAS Pharyngitis
When a patient has repeated strep throat episodes (particularly penicillin treatment failures), cefpodoxime proxetil is one of the recognized rescue options:
- Recurrent strep: Penicillin + rifampin or cefpodoxime proxetil
- This is because beta-lactamase-producing oral flora (e.g., H. influenzae, M. catarrhalis, anaerobes) can co-colonize the tonsillar tissue and inactivate penicillin locally — cefpodoxime is beta-lactamase stable and penetrates tonsillar tissue well.
When NOT to Use Cefpodoxime
| Situation | Preferred Drug |
|---|---|
| Standard first episode GAS pharyngitis, no allergy | Penicillin V or Amoxicillin |
| Non-anaphylactic (rash-type) penicillin allergy | Cephalexin or Cefadroxil |
| Severe penicillin allergy, macrolide available | Clindamycin or Azithromycin |
Cefpodoxime is a broader-spectrum, more expensive antibiotic — routine use contributes to antibiotic resistance and is not endorsed by the IDSA or CDC for uncomplicated first-episode strep throat.
Summary
Use cefpodoxime for GAS pharyngitis in two specific scenarios:
- True penicillin anaphylaxis — when you need a beta-lactam but cephalexin is too risky
- Recurrent/relapsing strep throat failing standard penicillin therapy
For everything else, stick to penicillin or amoxicillin.
Small white spots pharyngitis
Finding Sources
Searching the Web
white spots on tonsils pharyngitis differential diagnosis strep EBV
Finding Sources
Searching Images
white spots exudate tonsils pharyngitis strep throat
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
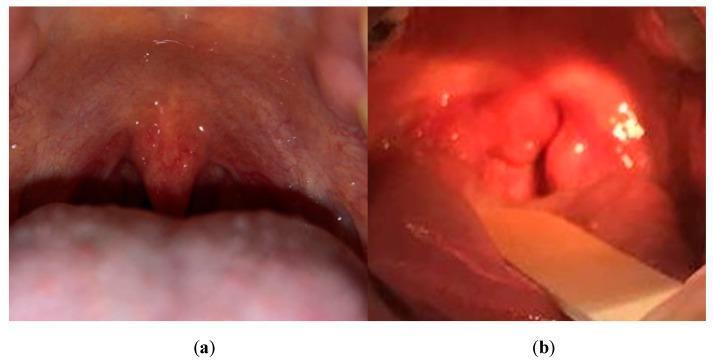
White Spots on the Tonsils/Throat — What Do They Mean?
White spots (exudate) on the tonsils or pharynx are a non-specific sign — they narrow the differential but don't diagnose by themselves. Here is the full clinical picture:
Differential Diagnosis by Appearance & Context
| Cause | Type of White Spots | Key Distinguishing Features |
|---|---|---|
| Group A Strep (GAS) | White/yellow patchy exudate on tonsils | Sudden onset, high fever, NO cough, tender anterior cervical nodes, palatal petechiae |
| Infectious Mononucleosis (EBV) | Thick grey-white patches, may cover entire tonsil | Extreme fatigue, posterior cervical adenopathy, splenomegaly, age 15–25 yrs |
| Viral tonsillitis (adenovirus, etc.) | Mild exudate or none | Usually with cough, runny nose, conjunctivitis ("pharyngoconjunctival fever") |
| Diphtheria | Tough, grey-white pseudomembrane that bleeds when removed | Rare (unvaccinated), "bull neck," stridor, systemic toxicity |
| Vincent's angina (Fusobacterium) | Unilateral grey ulcerative membrane | Foul breath, unilateral tonsillar ulceration |
| Oral candidiasis (thrush) | White curd-like plaques, easily wiped off | Immunocompromised, post-antibiotic, painful; angular cheilitis |
| Peritonsillar abscess | Unilateral bulge with exudate | Uvular deviation, muffled "hot potato" voice, trismus |
| Tonsil stones (tonsilloliths) | Small white/yellow firm nodules in tonsillar crypts | No fever, bad breath, recurrent, painless or minimal discomfort |
Key Clinical Clues
Points TOWARD Strep GAS:
- Sudden severe sore throat, high fever (>38.5°C)
- Tonsillar exudate + palatal petechiae (pathognomonic combination)
- Tender anterior cervical lymphadenopathy
- Scarlatiniform (sandpaper) rash
- No cough, no rhinorrhea
Points TOWARD Mono (EBV):
- Gradual onset, profound fatigue persisting weeks
- Posterior cervical adenopathy, splenomegaly
- Age 15–30 years
- Rash after amoxicillin/ampicillin (classic clue)
Points TOWARD Fungal (Candida):
- Immunocompromised (HIV, diabetes, steroid use, post-antibiotics)
- Plaques wipe off, leaving bleeding surface
- Angular cheilitis
Diagnostic Approach
- RADT (Rapid Antigen Detection Test) — first-line for suspected GAS
- Throat culture — if RADT negative in children (gold standard)
- Monospot test / EBV heterophile antibodies — if mono suspected (note: 25% false-negative in first 10 days)
- Do NOT give amoxicillin empirically if mono is possible — causes a florid rash in ~70–100% of EBV patients
Important Warning Signs (Seek Immediate Care)
- Stridor, drooling, difficulty breathing → possible epiglottitis
- Trismus + uvular deviation → peritonsillar abscess (needs drainage)
- Tough grey membrane that bleeds → possible diphtheria
- Symptoms >5 days with no improvement
The presence of exudate alone does not reliably distinguish bacterial from viral pharyngitis — scoring systems (Centor, McIsaac) combined with RADT remain the standard approach. — Textbook of Family Medicine 9e; Sherris Medical Microbiology 8e
This is a shared conversation. Sign in to Orris to start your own chat.