Cilinical examination of the abdomen on normal subject
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material to compose a thorough, well-structured answer. Let me deliver it:
Clinical Examination of the Abdomen (Normal Subject)
The abdominal examination follows a strict sequence: General Examination → Inspection → Palpation → Percussion → Auscultation. On a normal subject, all findings are used as the baseline against which pathology is detected.
Preparation & Positioning
-
The patient lies flat on their back, legs extended (a pillow under the head is acceptable).
-
For palpation, hips and knees are flexed to relax abdominal muscles.
-
The abdomen is fully exposed from the nipple line above to the saphenous openings (inguinal/femoral rings) below.
-
Examination is performed in good light, preferably daylight.
-
The examiner inspects first from the side, then tangentially, then from either end of the bed.
-
S Das A Manual on Clinical Surgery 13th Edition, p. 460
Surface Anatomy Reference
The abdomen is divided into nine regions by two horizontal and two vertical lines:
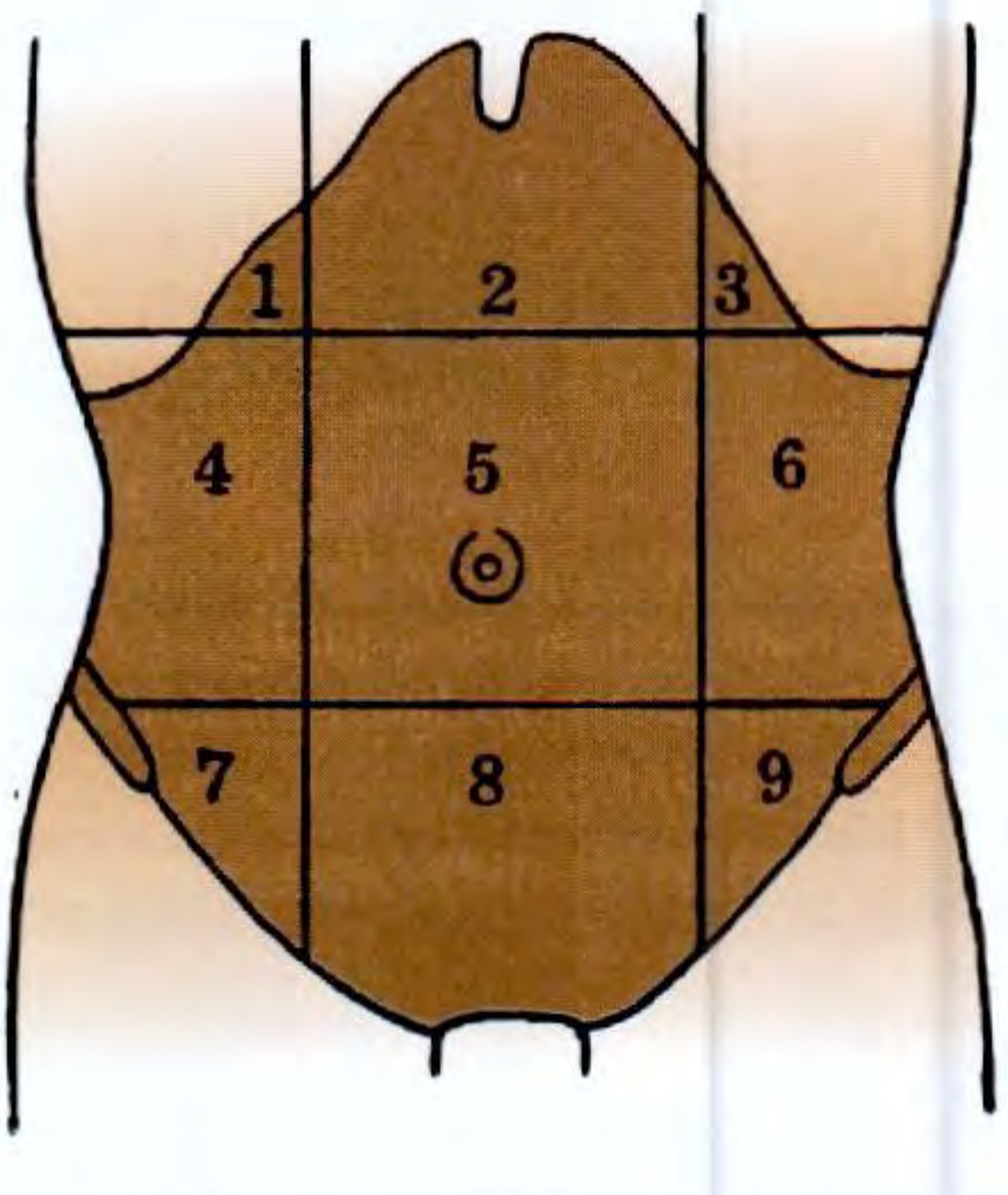
| No. | Region |
|---|---|
| 1 | Right hypochondrium |
| 2 | Epigastrium |
| 3 | Left hypochondrium |
| 4 | Right lumbar (flank) |
| 5 | Umbilical |
| 6 | Left lumbar (flank) |
| 7 | Right iliac fossa |
| 8 | Hypogastrium (suprapubic) |
| 9 | Left iliac fossa |
Alternatively, a simpler 4-quadrant scheme (RUQ, LUQ, RLQ, LLQ) is used for quick clinical description.
- S Das A Manual on Clinical Surgery 13th Edition, p. 523
Step 1: General Examination (Before the Abdomen)
Before focusing on the abdomen, a general survey is done:
-
Hands: Pallor of palmar creases (anaemia), clubbing, leukonychia, Dupuytren's contracture (liver disease), flapping tremor (hepatic encephalopathy).
-
Eyes: Jaundice (scleral icterus), anaemia (conjunctival pallor), xanthelasma.
-
Face/Mouth: Parotid enlargement, angular stomatitis, glossitis, telangiectasia (Osler-Weber-Rendu).
-
Neck: Left supraclavicular lymphadenopathy (Virchow's node / Troisier's sign) - suggests intra-abdominal malignancy.
-
Vital signs: Heart rate, BP, respiratory rate, temperature, weight/BMI.
-
Bailey and Love's Short Practice of Surgery 28th Edition, p. 1076
Step 2: Inspection
Inspect systematically:
1. Hernial Orifices (inspect first)
- Look at the inguinal, femoral, and umbilical rings. Ask the patient to cough - a cough impulse indicates a hernia.
- S Das advises inspecting hernial orifices first, as they may be the cause of acute abdominal symptoms.
2. Skin
- Normal: No scars, erythema, pigmentation, or rash.
- Note any scars - linear (healed by first intention) vs. broad/irregular (wound infection).
- Engorged superficial veins:
- Around umbilicus ("caput medusae") - portal hypertension.
- On flanks running upward - IVC obstruction.
- Hard subcutaneous periumbilical nodule (Sister Mary Joseph's nodule) - intra-abdominal carcinoma.
3. Umbilicus
- Normal position: Midway between the xiphoid tip and the pubic symphysis.
- Normal appearance: Inverted (slit-like), central.
- Displacement upward - pelvic mass; downward - ascites (Tanyol's sign).
- Eversion - ascites; deep inversion - obesity.
4. Contour / Shape of the Abdomen
- Normal: Flat or gently scaphoid (concave) in a lean person; slightly protuberant in a well-nourished adult.
- Normal umbilicus: Inverted in obesity vs. everted in intra-abdominal distension - a key distinguishing feature.
- The 5 "Fs" of distension: Fat, Fluid, Flatus, Faeces, Foetus.
5. Respiratory Movements
- Normal: The abdominal wall rises gently with inspiration (predominantly abdominal breathing in males; thoracic in females).
- Reduced or absent movement indicates peritoneal irritation (localized or diffuse).
6. Visible Peristalsis
- Normal: Not visible.
- Visible peristalsis indicates obstruction (gastric outlet - left to right; small bowel - "ladder pattern"; transverse colon - right to left).
7. Pulsations
- Normal: A faint aortic pulsation may occasionally be seen in thin individuals in the epigastrium.
- A prominent expansile pulsation suggests abdominal aortic aneurysm.
Step 3: Palpation
Technique
- The examiner's forearm must be horizontal at the level of the patient's abdomen.
- Use the volar (palmar) surfaces of the fingers - never the fingertips pointing downward.
- Begin palpation in the quadrant furthest from the site of pain (if any) and end at the painful area.
- Watch the patient's face for signs of discomfort during palpation.
Superficial (Light) Palpation
- Detect tenderness, superficial masses, rigidity, guarding.
- Normal: Soft, non-tender abdomen, no involuntary guarding.
- Voluntary guarding: Patient tenses abdomen in anticipation; can be overcome by distraction.
- Involuntary guarding/rigidity: True sign of peritoneal irritation.
Deep Palpation
Used to examine the solid organs and identify deeper masses.
Liver
- Begin in the right iliac fossa, move upward with each expiration.
- The right hand is placed flat, fingers pointing toward the right costal margin.
- Alternatively, use the bimanual method (left hand behind the right loin) or dipping method for tense ascites.
- Normal: Not palpable below the costal margin (or just palpable with a smooth, firm, regular edge on deep inspiration in thin individuals).
- Note: edge, surface, consistency, tenderness, pulsatility.
Gallbladder
- Palpable just below the liver edge at the tip of the 9th costal cartilage, right of midline.
- Normal: Not palpable.
- Murphy's sign: Deep inspiration while pressure is applied at the gallbladder point produces inspiratory arrest in acute cholecystitis.
Spleen
- Begin palpation from the right iliac fossa, move toward the left costal margin.
- Bimanual: left hand behind the left lower ribs, right hand palpating.
- The patient may be asked to roll to the right lateral decubitus (right lateral position) to bring the spleen forward.
- Normal: Not palpable (must be 2-3 times its normal size to be felt).
Kidneys
- Bimanual (ballottement): Left hand in the loin (posteriorly), right hand in the flank (anteriorly).
- The kidney can be ballotted (bounced between the two hands).
- Normal: Left kidney generally not palpable; right kidney occasionally palpable in thin individuals on deep inspiration.
Aorta
- Palpate in the midline epigastrium.
- Normal: A pulsatile, non-expansile aorta felt as a single midline structure in thin patients.
- Widened or expansile pulsation - aneurysm.
Rebound Tenderness (Blumberg's Sign)
- Press slowly and deeply, then release rapidly.
- Pain on release = peritoneal irritation.
- Normal: No rebound tenderness.
Fluid Thrill and Shifting Dullness
- Tested during percussion (see below), but sometimes elicited during palpation by the fluid thrill test.
Step 4: Percussion
- Used to delineate organ boundaries and detect free fluid or gas.
Liver Dullness
- Percuss downward from the right 4th intercostal space in the mid-clavicular line.
- Upper border: Where resonance changes to dullness (normally 5th ICS, MCL).
- Lower border: Where dullness ends (normally at the costal margin in MCL).
- Loss of liver dullness (gas over liver) is a critical sign of hollow viscus perforation (e.g., peptic ulcer perforation).
Splenic Dullness
- Traube's space (lower left chest, bounded by stomach, diaphragm, splenic flexure): normally resonant.
- Dullness in Traube's space suggests splenomegaly.
Percussion for Ascites
- Shifting dullness: Percuss from umbilicus to flank - note level where dullness begins. Patient rolls to the opposite side; the dullness shifts (fluid follows gravity). Normal: No shifting dullness.
- Fluid thrill: Place a hand flat on one flank; flick the other flank with a finger. An assistant's hand on the midline prevents conduction through fat. A transmitted impulse = free fluid. Normal: No fluid thrill.
Percussion of the Bladder
- A distended bladder produces suprapubic dullness extending upward from the symphysis pubis.
- Normal: Suprapubic area is resonant (empty bladder).
Step 5: Auscultation
- Use the diaphragm of the stethoscope, held lightly on the abdomen.
- Listen for at least 2 minutes before declaring bowel sounds absent.
Bowel Sounds
- Normal: Soft gurgling sounds every 5-10 seconds, reflecting peristalsis.
- Increased (tinkling, high-pitched): Mechanical obstruction, early peritonitis.
- Absent: Paralytic ileus, advanced peritonitis, immediately post-operative.
Vascular Bruits
- Auscultate over the aorta (epigastrium), renal arteries (just lateral to umbilicus bilaterally), and iliac arteries.
- Normal: No bruits.
- A bruit suggests arterial stenosis or aneurysm.
Succussion Splash
- The patient is asked to move rapidly from side to side while the examiner listens over the epigastrium.
- An audible splash indicates fluid + air in a hollow viscus (e.g., gastric outlet obstruction).
- Normal: No succussion splash (or a mild splash if the patient has just eaten/drunk).
Step 6: Special Tests & Completion
- Per rectal (digital rectal) examination: Should not be omitted. Assess anal sphincter tone, rectal mucosa, prostate (in males), cervix/uterus via posterior wall (in females). Note stool color/consistency.
- Hernial orifices re-examined with the patient standing and coughing.
- Examine external genitalia and scrotum (testicular malignancy can produce para-aortic masses).
Summary: Normal Findings on Abdominal Examination
| Step | Normal Finding |
|---|---|
| Inspection | Flat/scaphoid contour; inverted or centrally placed umbilicus; no scars, no dilated veins, no visible peristalsis; active respiratory movements |
| Superficial palpation | Soft, non-tender, no guarding or rigidity |
| Deep palpation | Liver, spleen, kidneys not palpable (except occasionally in thin individuals); no masses |
| Percussion | Liver dull (5th ICS to costal margin); Traube's space resonant; no shifting dullness |
| Auscultation | Normal bowel sounds every 5-10 sec; no bruits; no succussion splash |
Sources:
- S Das, A Manual on Clinical Surgery, 13th ed. - Bailey and Love's Short Practice of Surgery, 28th ed. - Textbook of Family Medicine, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.