Explain Larynx I'm new to this topic explain everything released to anatomy and all
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have all the information and images needed for a comprehensive, beginner-friendly explanation. Let me compile the full answer.
The Larynx - Complete Anatomy for Beginners
The larynx (commonly called the "voice box") is a hollow musculoligamentous structure with a cartilaginous framework that caps the lower respiratory tract. It sits in the front of the neck, roughly at the level of vertebrae C3-C6 in adults.
Key point: The PRIMARY function of the larynx is not voice production - it is the protection of the airway during swallowing. Voice production is a secondary, evolutionary bonus.
1. Position and Relations
The larynx is positioned in the midline of the neck:
- Above: connects to the pharynx (throat) and hangs from the hyoid bone
- Below: continuous with the trachea (windpipe)
- Posteriorly: the esophagus lies behind it
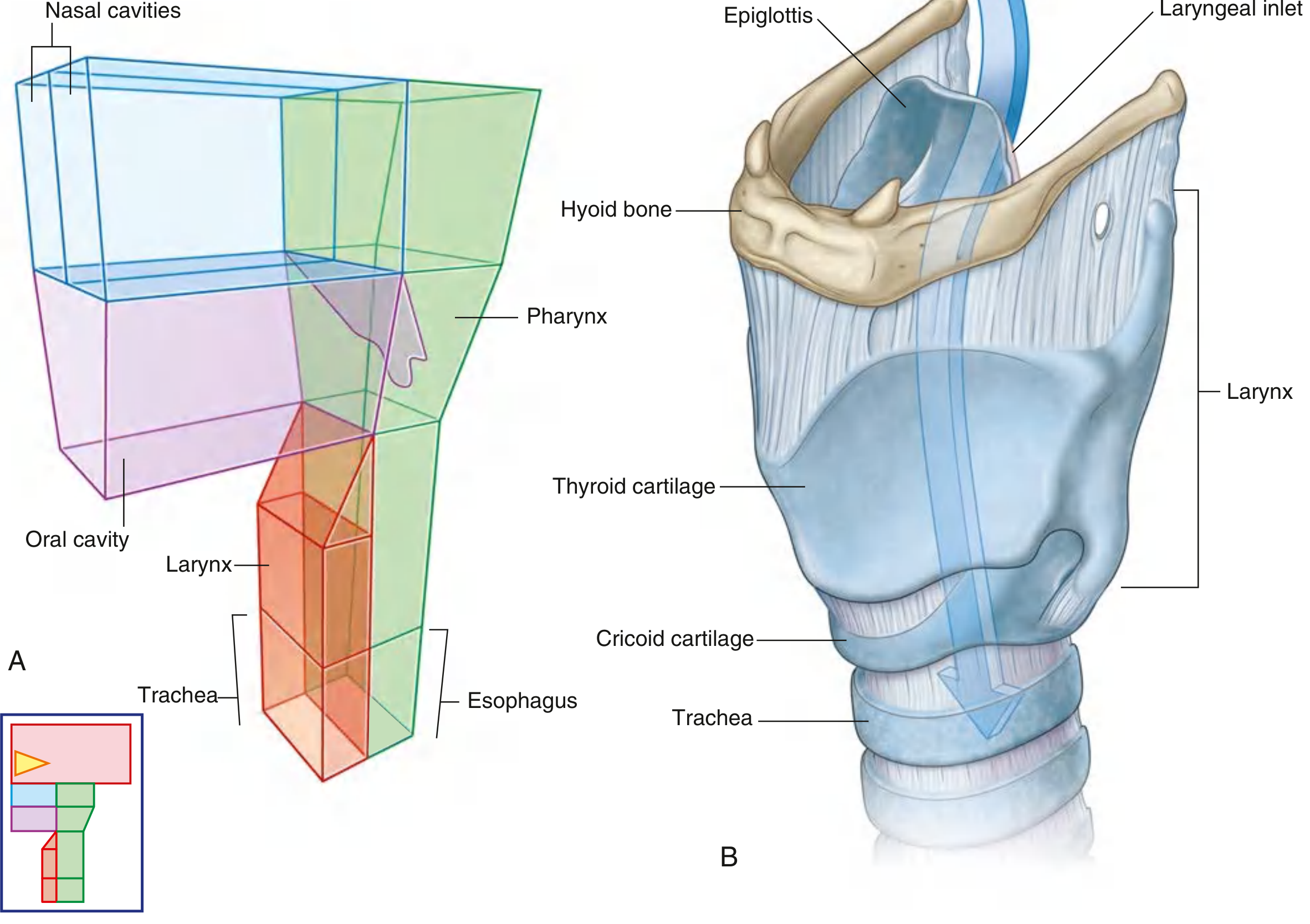
Fig. 8.212 - Position of the larynx relative to other structures (A) and lateral view (B) - Gray's Anatomy for Students
During swallowing, the larynx moves dramatically upward and forward, which closes the laryngeal inlet and opens the esophagus so food goes the right way.
2. The Cartilaginous Framework
Think of the larynx like a house - the cartilages are its walls and skeleton.
There are 3 unpaired (single) cartilages and 3 paired (double) cartilages.
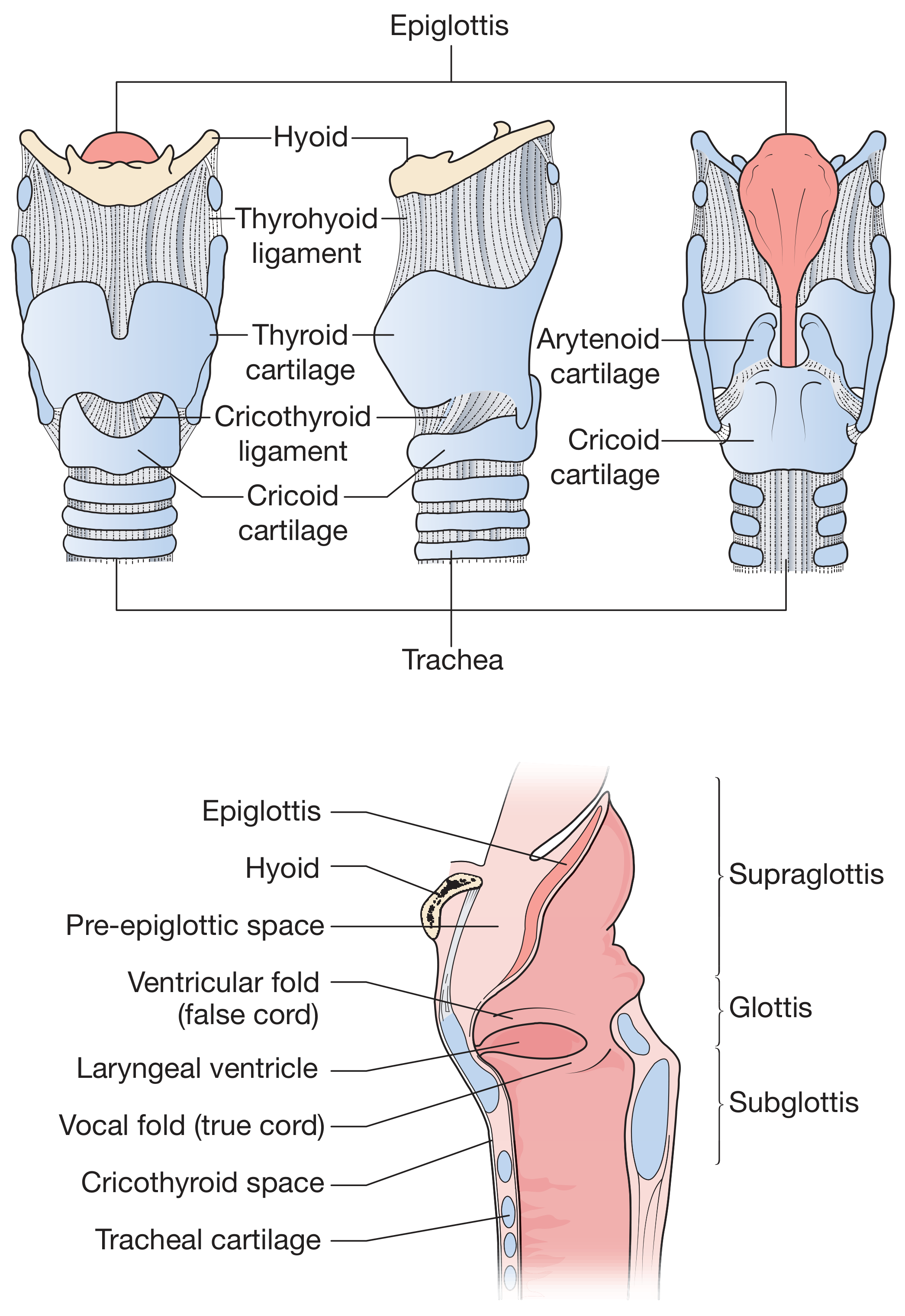
Figure 52.6 - Anatomy of the larynx - Bailey & Love's Short Practice of Surgery
Unpaired Cartilages
A. Thyroid Cartilage (the largest)
- Formed by a right and left lamina that join in the front
- The point where they fuse projects forward as the laryngeal prominence ("Adam's apple")
- In men, the two laminae meet at a sharper angle (90°), making the Adam's apple more visible; in women it is 120°
- At the top, the superior thyroid notch separates the two laminae - palpable in the neck
- The posterior margin of each lamina extends as a superior horn (connects to hyoid) and an inferior horn (articulates with cricoid cartilage)
- Muscles attach along the oblique line on the outer surface
B. Cricoid Cartilage (the most important structurally)
- Sits below the thyroid cartilage and connects to the trachea below
- It is the only complete ring of cartilage in the entire airway - this makes it unique
- Shaped like a signet ring: broad plate (lamina) posteriorly, narrow arch anteriorly
- The posterior lamina has two oval depressions for the posterior crico-arytenoid muscles, separated by a ridge for the esophagus
- Has articular facets for both the arytenoid cartilages above and the inferior horns of the thyroid cartilage laterally
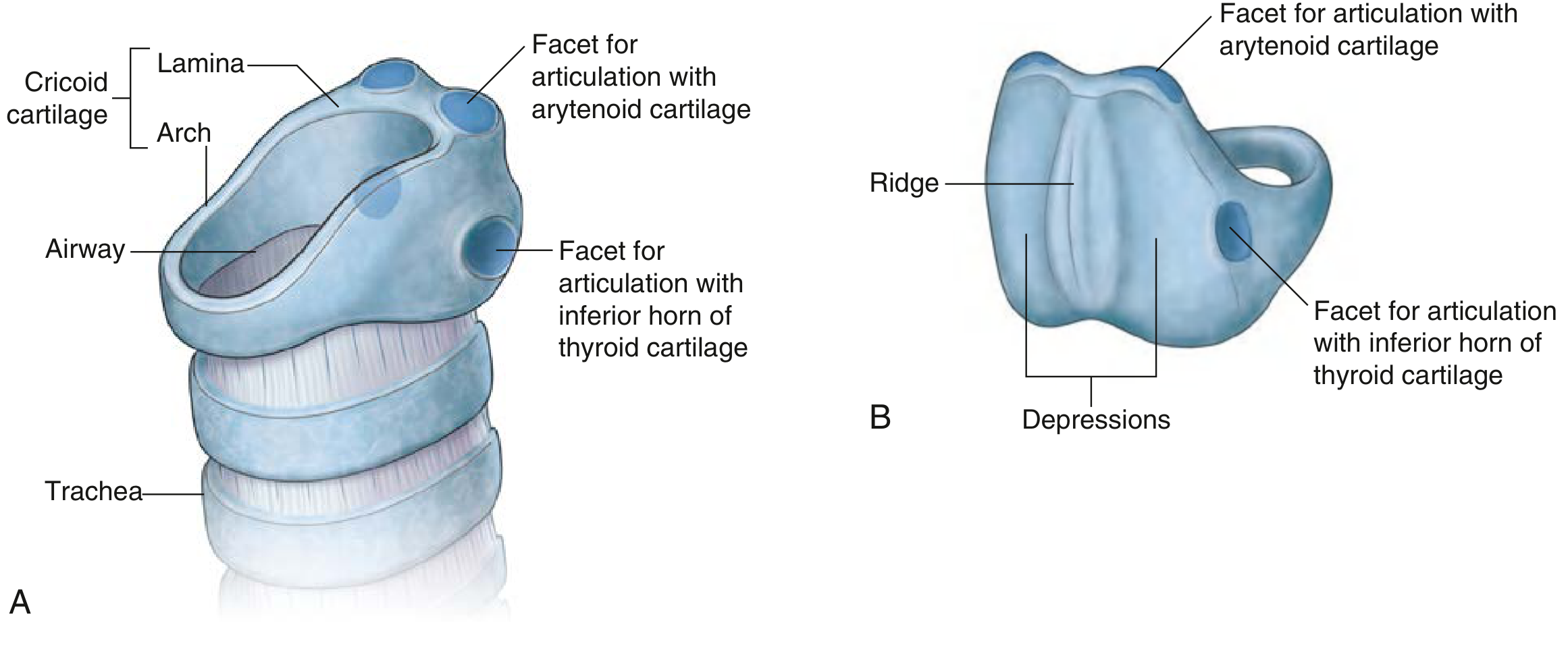
Fig. 8.213 - Cricoid cartilage - Gray's Anatomy for Students
Clinical note: In children, the cricoid cartilage marks the narrowest part of the airway - this is why a breathing tube placed too tightly can damage this spot.
C. Epiglottis
- A leaf-shaped cartilage made of elastic (flexible) cartilage (not the rigid hyaline type)
- Attached below to the thyroid cartilage angle; its upper portion projects freely toward the base of the tongue
- During swallowing, it folds backward like a trap door to cover the laryngeal opening and prevent food/liquid from entering the airway
- Contains tiny perforations through which glands and nerves pass
Paired Cartilages
D. Arytenoid Cartilages (most functionally important pair)
- Pyramid-shaped cartilages sitting on the upper rim of the cricoid lamina posteriorly
- Each has:
- A vocal process projecting anteriorly - the vocal ligament attaches here
- A muscular process projecting laterally - most laryngeal muscles attach here
- An apex pointing upward - the corniculate cartilage sits on top
- Movement of the arytenoids opens and closes the vocal folds - they can slide, rotate, and glide on the cricoid
E. Corniculate Cartilages
- Small horn-shaped cartilages sitting on top of each arytenoid apex
- They extend the arytenoids slightly and contribute to the aryepiglottic folds (lateral walls of the laryngeal opening)
F. Cuneiform Cartilages
- Small rod-shaped pieces inside the aryepiglottic folds, anterior to the corniculate cartilages
- Create small visible bumps (cuneiform tubercles) on the inlet
3. Ligaments and Membranes
The cartilages are joined and supported by membranes and ligaments:
| Structure | What it connects | Role |
|---|---|---|
| Thyrohyoid membrane | Thyroid cartilage → hyoid bone above | Suspends larynx from hyoid; has a hole for the internal superior laryngeal nerve and vessels |
| Cricothyroid ligament (conus elasticus) | Cricoid → thyroid cartilage; upper free edge = vocal ligaments | Forms the floor of the larynx; its thickened midline part is the median cricothyroid ligament |
| Quadrangular membrane | Epiglottis lateral margin → arytenoid cartilage | Upper wall of the larynx; its free lower margin = vestibular ligament (false cord) |
| Cricotracheal ligament | Cricoid → first tracheal ring | Joins larynx to trachea |
Clinical note: The median cricothyroid ligament is the site of emergency cricothyrotomy - a life-saving cut to open the airway when normal intubation fails. It's accessible because it sits just below the Adam's apple, with no major vessels overlying it.
4. Cavity of the Larynx - The Three Regions
The inside of the larynx is divided into three regions by two pairs of folds:
LARYNGEAL INLET (opening into pharynx)
↓
┌─── VESTIBULE (supraglottis) ───┐
│ (above the vestibular folds) │
└─────────────────────────────────┘
↓
VESTIBULAR FOLDS = FALSE VOCAL CORDS
↓
┌── MIDDLE CHAMBER (ventricle) ──┐
│ (between false & true cords) │
└─────────────────────────────────┘
↓
VOCAL FOLDS = TRUE VOCAL CORDS
↓
┌── INFRAGLOTTIC CAVITY (subglottis) ┐
└────────────────────────────────────┘
↓
TRACHEA
The Three Regions in Detail:
1. Vestibule (Supraglottis)
- From the laryngeal inlet down to the vestibular (false) folds
- Bounded laterally by the aryepiglottic folds
- The pre-epiglottic space is a fat-filled space anterior to the epiglottis
2. Middle Chamber (Glottis)
- The narrowest and most important part
- The rima glottidis is the actual opening between the two true vocal folds - this is what opens and closes for breathing vs. speaking
- On each side, between the false and true cords, is a small pocket called the laryngeal ventricle (sinus of Morgagni)
- A small diverticulum called the laryngeal saccule extends from each ventricle and contains mucous glands that lubricate the vocal folds
3. Infraglottic Cavity (Subglottis)
- Below the true vocal folds down to the lower border of the cricoid cartilage
- Widens to become the trachea
5. The Vocal Folds (True Vocal Cords)
The true vocal folds are the key structures for voice production:
- They appear white (unlike the pink surrounding mucosa)
- Each fold contains a vocal ligament (the upper free edge of the conus elasticus) and the vocalis muscle
- They meet anteriorly at the midline of the thyroid cartilage (called the anterior commissure)
- Posteriorly, each is attached to the vocal process of an arytenoid cartilage
- This arrangement creates a characteristic "V" shape when viewed from above
Rima Glottidis = the gap between the two vocal folds:
- Intermembranous part - between the ligamentous vocal folds anteriorly (about 3/5 of total length)
- Intercartilaginous part - between the arytenoid cartilages posteriorly (about 2/5)
6. Intrinsic Muscles of the Larynx
These muscles move the laryngeal cartilages to open/close the airway and produce voice:
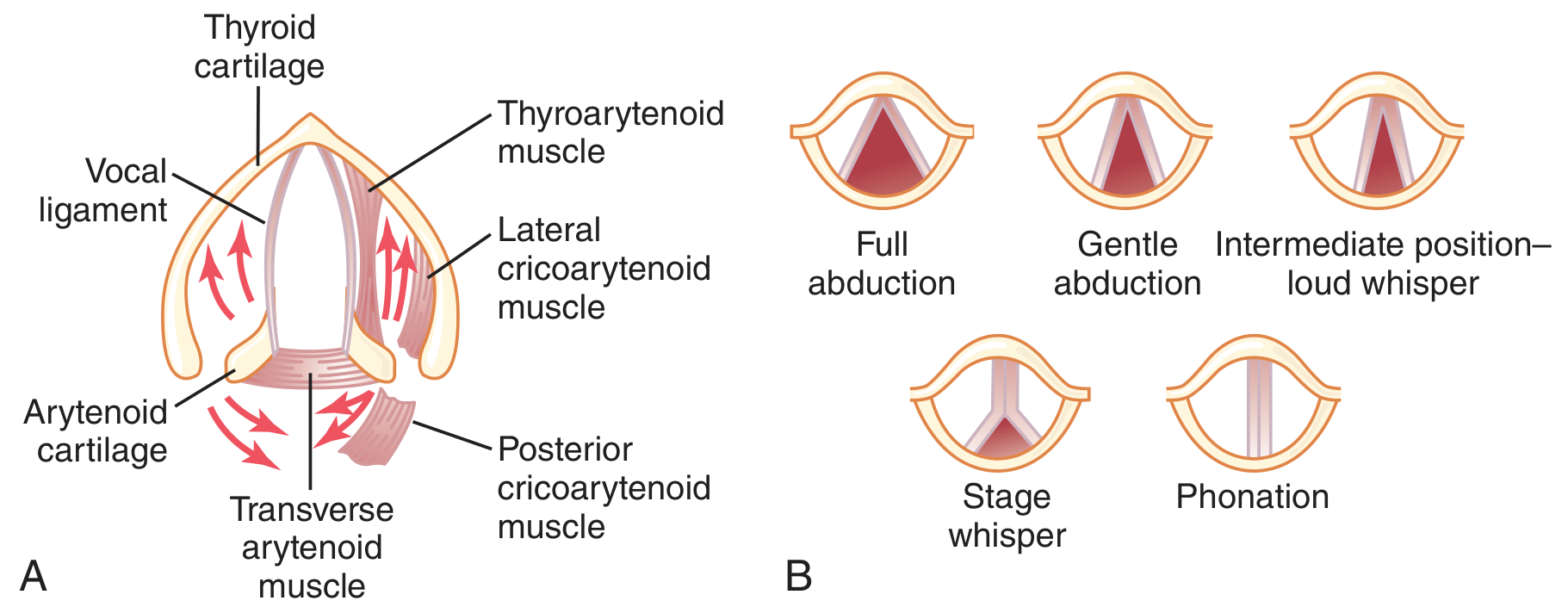
Fig. 38.9 - Laryngeal anatomy and vocal cord positions during phonation - Guyton & Hall Medical Physiology
| Muscle | Action | Nerve |
|---|---|---|
| Posterior crico-arytenoid (PCA) | Abducts vocal folds (opens airway) - the ONLY abductor | Recurrent laryngeal nerve (RLN) |
| Lateral crico-arytenoid (LCA) | Adducts vocal folds (closes airway) | RLN |
| Transverse arytenoid | Adducts - closes posterior glottis | RLN |
| Oblique arytenoid | Closes laryngeal inlet (sphincter function) | RLN |
| Cricothyroid | Tenses/lengthens vocal folds (raises pitch) | External branch of superior laryngeal nerve |
| Thyro-arytenoid | Relaxes/shortens vocal folds (lowers pitch); also adducts | RLN |
| Vocalis | Fine tension adjustment on vocal fold | RLN |
Key memory point: The Posterior Crico-Arytenoid is the ONLY abductor. If both recurrent laryngeal nerves are damaged (e.g., in thyroid surgery), only the adductors work - the vocal folds adduct and close the airway, causing respiratory distress.
7. Nerve Supply
The larynx is innervated entirely by the vagus nerve (CN X) via two branches:
Superior Laryngeal Nerve (SLN)
- Arises from the vagus at the nodose ganglion
- Divides into:
- Internal branch: purely sensory above the vocal folds (enters via thyrohyoid membrane)
- External branch: motor to the cricothyroid muscle only
Recurrent Laryngeal Nerve (RLN)
- Loops around the subclavian artery (right) or arch of aorta (left)
- Ascends in the tracheo-esophageal groove
- Provides sensory supply below the vocal folds + motor to all intrinsic muscles except cricothyroid
Clinical note: The RLN is at risk during thyroid surgery, carotid endarterectomy, and thoracic procedures. Unilateral damage causes a hoarse voice; bilateral damage can cause airway obstruction.
8. Blood Supply
| Vessel | Region supplied |
|---|---|
| Superior laryngeal artery (from superior thyroid artery → external carotid) | Upper larynx |
| Inferior laryngeal artery (from inferior thyroid artery → thyrocervical trunk) | Lower larynx |
Veins follow the same pattern. Lymphatics from above the vocal folds drain to upper deep cervical nodes; those from below drain to lower deep cervical nodes. The vocal folds themselves have very sparse lymphatic drainage.
9. How the Larynx Produces Sound (Phonation)
- Air from the lungs builds pressure below the closed vocal folds
- Pressure forces the folds apart - air rushes through
- The Bernoulli effect and myoelastic recoil snap the folds back together
- This vibration creates sound waves
- Pitch is controlled by the tension/length of vocal folds:
- Higher pitch = cricothyroid contracts → lengthens/tenses folds
- Lower pitch = thyro-arytenoid contracts → shortens/relaxes folds
- Volume depends on airflow pressure from the lungs
- The sound is then shaped into words by the tongue, lips, teeth, and palate
10. How the Larynx Protects the Airway
During swallowing, three lines of defense prevent aspiration:
- Epiglottis folds back over the laryngeal inlet (pushed by the base of tongue)
- Aryepiglottic folds constrict, narrowing the inlet
- True and false vocal folds adduct tightly shut
The larynx also moves upward and forward (you can feel your Adam's apple rise when you swallow), pulling the inlet away from the food bolus.
Summary Diagram: At a Glance
HYOID BONE (not part of larynx but suspends it)
|
Thyrohyoid membrane
|
THYROID CARTILAGE (largest, "Adam's apple")
├── Epiglottis (attached inside, faces up/back)
├── Arytenoid cartilages (on cricoid, posteriorly)
│ └── Vocal process (→ vocal ligament → vocal fold)
│
Cricothyroid ligament (median part = emergency airway site)
|
CRICOID CARTILAGE (only complete ring; marks C6)
|
Cricotracheal ligament
|
TRACHEA
Sources: Gray's Anatomy for Students, p. 1192-1203 | Bailey & Love's Short Practice of Surgery 28e, p. 798 | Guyton & Hall Textbook of Medical Physiology | Cummings Otolaryngology Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.