Abdomen Mass
Reading File
Asking for Preferences
In gynae
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pelvic mass" AND "gynaecology" AND diagnosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive textbook content. Let me compile the full answer.
Gynaecological Abdominal / Pelvic Mass
Based on Berek & Novak's Gynecology (Berek & Novak's Gynecology)
Classification & Differential Diagnosis
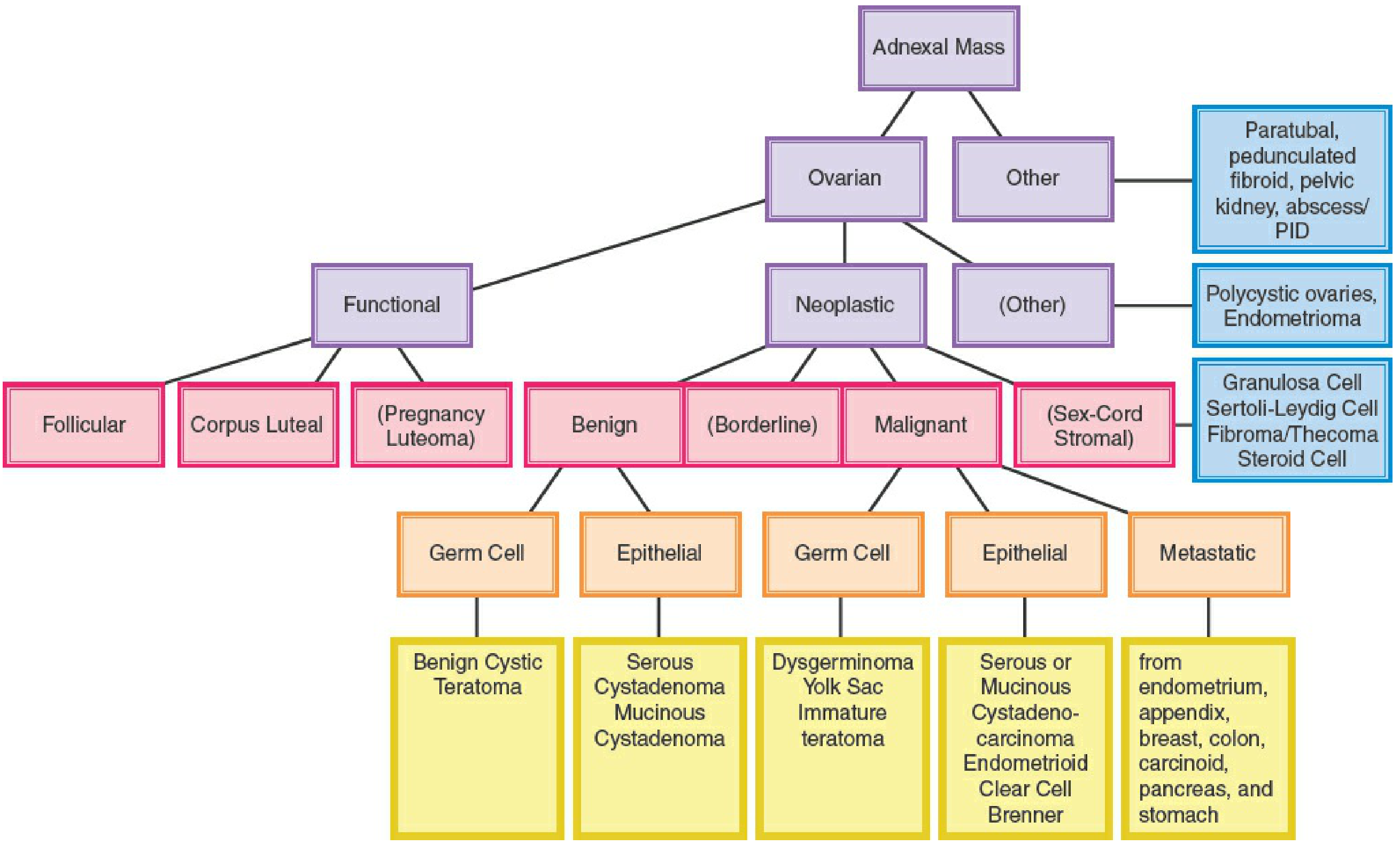
The single most important framework for gynaecological pelvic masses is the adnexal mass algorithm:
Causes of Pelvic Mass by Category (Reproductive-Age Women)
Urinary / Non-Gynae Mimics
- Full urinary bladder
- Urachal cyst
- Stool in sigmoid colon
- Peritoneal cyst
- Matted bowel/omentum
Uterine Masses
| Condition | Notes |
|---|---|
| Sharply anteflexed or retroflexed uterus | Feels like a mass on bimanual |
| Leiomyomas (Fibroids) | Most common benign uterine tumor; often asymptomatic |
| Intraligamentous leiomyomas | Can mimic adnexal mass |
| Intrauterine pregnancy | Always exclude first |
| Tubal (ectopic) pregnancy | Lateral adnexal mass, tender |
| Abdominal pregnancy | Rare |
| Uterine sarcoma | Rare malignant cause |
Uterine leiomyomas are by far the most common benign uterine tumors; they are more prevalent in African American women.
Ovarian / Adnexal Masses
Functional (non-neoplastic):
- Follicular cyst - most common; usually resolves spontaneously
- Corpus luteal cyst - can bleed causing acute pain
- Pregnancy luteoma
Neoplastic - Benign:
| Type | Examples |
|---|---|
| Germ cell (benign) | Benign cystic teratoma (dermoid) - most common in women <20 yrs; accounts for >50% of ovarian neoplasms in this group |
| Epithelial | Serous cystadenoma, Mucinous cystadenoma |
| Sex-cord stromal | Fibroma, Thecoma, Granulosa cell, Sertoli-Leydig cell |
| Other | Endometrioma ("chocolate cyst"), Paraovarian/paratubal cyst, Polycystic ovaries |
Neoplastic - Borderline (Low Malignancy Potential):
- Serous or mucinous borderline tumours
Neoplastic - Malignant:
| Type | Examples |
|---|---|
| Epithelial (most common) | Serous/mucinous cystadenocarcinoma, Endometrioid, Clear cell, Brenner |
| Germ cell (malignant) | Dysgerminoma, Yolk sac tumour, Immature teratoma |
| Metastatic | From endometrium, appendix, breast, colon, carcinoid, pancreas, stomach (Krukenberg) |
Inflammatory Masses
- Tubo-ovarian abscess (TOA) / complex
- Diverticular abscess
- Appendiceal abscess
Less Common But Must Exclude
- Pelvic kidney
- Carcinoma of colon, rectum, appendix
- Carcinoma of the fallopian tube
- Retroperitoneal tumours (anterior sacral meningocele)
Causes by Age Group (Approximate Frequency)
| Age Group | Most Likely Causes |
|---|---|
| Infancy | Functional cyst, Germ cell tumour |
| Prepubertal | Functional cyst, Germ cell tumour |
| Adolescent | Functional cyst, Pregnancy, Benign cystic teratoma/germ cell, Obstructive uterovaginal anomalies, Epithelial tumour |
| Reproductive | Functional cyst, Pregnancy, Uterine fibroids, Epithelial ovarian tumour, Endometrioma |
| Perimenopausal | Fibroids, Epithelial ovarian tumour, Functional cyst |
| Postmenopausal | Ovarian tumour (malignant or benign), Functional cyst, Bowel malignancy/inflammatory, Metastases |
Key point on malignancy risk: In women undergoing laparotomy for pelvic mass, malignancy was found in only 10% of those under 30, and most had low-malignancy-potential tumours. Mature cystic teratomas (dermoids) account for one-third of masses in women <30; endometriomas account for ~one-quarter in those aged 31-49.
Features Suggesting Benign vs. Malignant
| Feature | Likely Benign | Likely Malignant |
|---|---|---|
| Laterality | Unilateral | Bilateral |
| Consistency | Cystic | Solid or mixed |
| Mobility | Mobile | Fixed |
| Surface | Smooth | Irregular |
| Ascites | Absent | Present |
| Cul-de-sac nodules | Absent | Present |
| Growth rate | Slow | Rapid |
Investigations
- Pregnancy test - mandatory in all women of reproductive age regardless of stated sexual activity
- Transvaginal ultrasound (TVS) - primary diagnostic tool; characterises cystic vs. solid, uni- vs. multilocular, Doppler flow
- Transabdominal USS - useful in adolescents who may not tolerate TVS; also for large masses
- CT / MRI - for complex masses, staging malignancy, retroperitoneal extension
- Tumour markers:
- CA-125 - epithelial ovarian cancer (also raised in endometriosis, fibroids, PID)
- AFP (alpha-fetoprotein) + beta-hCG - germ cell tumours
- CEA - mucinous tumours / bowel primary
- Inhibin - granulosa cell tumours
- CBC - leucocytosis suggests inflammatory mass (TOA)
- Doppler flow studies - helpful in ovarian torsion
Key Clinical Points
- Uni- and multilocular simple cysts often resolve with observation; a solid component mandates surgical assessment due to high risk of germ cell tumour (especially in prepubertal girls)
- Ovarian torsion - acute onset severe pain + nausea/vomiting; Doppler flow may not reliably predict torsion; management is detorsion (not oophorectomy), even with absent flow, as ovarian recovery is likely
- Endometriosis in adolescents may have atypical appearance (non-pigmented, vesicular lesions); up to 70% of adolescents not responding to conventional analgesia have endometriosis at laparoscopy
- Referral to a gynecologic oncologist is recommended when a pelvic mass is suspicious on USS
- In postmenopausal women, any pelvic mass warrants prompt evaluation for malignancy
Berek & Novak's Gynecology, pp. 391-392, 415-419, 448-450
This is a shared conversation. Sign in to Orris to start your own chat.