Pneumonia
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Pneumonia - Medical Student Exam Overview
Sources: Harrison's Principles of Internal Medicine 22E (2025), Fishman's Pulmonary Diseases, Grainger & Allison's Diagnostic Radiology
Definition
Pneumonia is an infection of the pulmonary parenchyma. It is frequently misdiagnosed, mistreated, and underestimated despite carrying significant morbidity and mortality. - Harrison's Principles of Internal Medicine 22E, p. 1066
Classification by Acquisition Setting
| Type | Definition | Key Features |
|---|---|---|
| CAP (Community-Acquired) | Acquired outside hospital or healthcare settings | Most common; S. pneumoniae is the leading cause |
| HAP (Hospital-Acquired) | Develops ≥48 h after admission | Gram-negatives, S. aureus dominate |
| VAP (Ventilator-Associated) | Develops ≥48-72 h after endotracheal intubation | High mortality; bronchopneumonia pattern typical |
| Aspiration Pneumonia | Macroaspiration of oropharyngeal/gastric contents | Accounts for 5-15% of CAP; gravity-dependent lung zones |
The older category "healthcare-associated pneumonia (HCAP)" has been discontinued - it did not reliably predict resistant organisms and led to overuse of broad-spectrum antibiotics. - Harrison's 22E
Pathophysiology
Route of Entry
Microorganisms reach the lower respiratory tract by:
- Microaspiration of oropharyngeal organisms (most common)
- Inhalation of airborne droplets
- Hematogenous spread from a distant focus
- Direct mucosal dispersion
Positive Feedback Loop Model (Modern Concept)
The lung is not a sterile environment - it has its own microbiota. Pneumonia is not simply "invasion of a sterile space" but an emergent phenomenon:
- Inflammatory event → epithelial/endothelial injury → cytokine/chemokine/catecholamine release
- Some catecholamines selectively promote growth of S. pneumoniae and P. aeruginosa
- This creates a self-accelerating loop: more inflammation → more nutrients for bacteria → more bacterial growth → dominant pathogen emerges
- In CAP/HAP, the trigger is often a viral infection + microaspiration
Host Defense Mechanisms (that can be overcome)
- Nasal hairs, turbinates, branching airways
- Mucociliary clearance
- Gag and cough reflexes
- Alveolar macrophages, neutrophils, secretory IgA
Mediators of Damage
- IL-6, TNF → fever
- IL-8, G-CSF → neutrophil recruitment
- Neutrophil/macrophage mediators → alveolar capillary leak → impaired oxygenation, hypoxemia, infiltrates
- Some bacteria interfere with hypoxic vasoconstriction → severe hypoxemia
Pathology - Classic Stages (Lobar Pneumococcal Pneumonia)
These four stages are a high-yield exam topic:
| Stage | Histology | Key Feature |
|---|---|---|
| 1. Edema | Proteinaceous exudate + bacteria in alveoli | Vascular engorgement; serous fluid |
| 2. Red Hepatization | RBCs fill alveoli; neutrophils appear | Lung = liver-like consistency; red-red color |
| 3. Gray Hepatization | RBCs lysed; neutrophils + fibrin dominate; bacteria disappear | Infection being contained; gas exchange improves |
| 4. Resolution | Macrophages clear debris (neutrophils, bacteria, fibrin) | Return to normal |
This staging best applies to lobar pneumococcal pneumonia; VAP typically shows a bronchopneumonia pattern instead. - Harrison's 22E, p. 1067
Types by Radiographic Pattern
This is a high-yield classification for matching pathogen to X-ray appearance:
| Radiographic Pattern | Characteristic | Common Organisms |
|---|---|---|
| Lobar consolidation | Entire lobe opacified; air bronchograms; no volume loss | S. pneumoniae, Klebsiella pneumoniae |
| Bronchopneumonia | Patchy, multifocal infiltrates; peribronchial distribution | S. aureus, Gram-negative bacilli, anaerobes, S. pneumoniae |
| Interstitial pneumonia | Reticular/reticulonodular pattern; peribronchovascular infiltrate | Viruses, Mycoplasma pneumoniae |
| Cavitation | Air-fluid level within opacity | S. aureus (pneumatoceles), M. tuberculosis, Gram-negatives, anaerobes |
| Miliary | Diffuse tiny nodules | M. tuberculosis, endemic fungi, viruses |
Important caveat: No radiographic pattern is specific for any one organism. Overlap is common and differentiation based solely on CXR is unreliable. - Grainger & Allison's Diagnostic Radiology
Lobar Pneumonia mechanism: Organisms induce alveolar inflammatory edema. When consolidation fills an entire lobe, an air bronchogram appears (airway outlined by surrounding fluid-filled alveoli). Volume loss is absent or minimal in early consolidation. - Fishman's Pulmonary Diseases
Typical vs. Atypical Pneumonia
| Feature | Typical | Atypical |
|---|---|---|
| Onset | Acute (hours) | Subacute (days) |
| Presentation | Productive cough, rigors, pleuritic chest pain, high fever | Dry cough, headache, myalgias, low-grade fever |
| Pathogens | S. pneumoniae, H. influenzae, Klebsiella | Mycoplasma, Chlamydophila pneumoniae, Legionella, viruses |
| CXR | Lobar consolidation | Interstitial/patchy bilateral infiltrates |
| Sputum | Purulent, productive | Scant or absent |
| Response to beta-lactams | Yes | No (need macrolide/fluoroquinolone) |
Common Causative Pathogens
CAP Pathogens (most to least common):
- Streptococcus pneumoniae (most common overall)
- Mycoplasma pneumoniae (most common atypical; young adults)
- Haemophilus influenzae (COPD patients)
- Legionella pneumophila (atypical; hyponatremia, GI symptoms, Pontiac fever)
- Chlamydophila pneumoniae
- Respiratory viruses (influenza, RSV, SARS-CoV-2, metapneumovirus)
- Staphylococcus aureus (post-influenza; cavitation/pneumatoceles)
- Klebsiella pneumoniae (alcoholics; "currant jelly sputum"; upper lobe)
Clinical Features
Symptoms:
- Fever, chills, sweats, tachycardia
- Cough (non-productive or productive - mucoid, purulent, blood-tinged)
- Gross hemoptysis → suggests necrotizing pneumonia (think CA-MRSA)
- Dyspnea, pleuritic chest pain
- GI symptoms (nausea, vomiting, diarrhea) in up to 20% of patients
- Fatigue, headache, myalgias, arthralgias
Signs on examination:
- Tachypnea; accessory muscle use
- Dullness to percussion (consolidation/effusion)
- Increased tactile fremitus (consolidation)
- Crackles (crepitations), bronchial breath sounds, pleural friction rub
- Elderly: may present with new-onset confusion or worsening of chronic illness with few respiratory symptoms
Diagnosis
Clinical Diagnosis
Requires: compatible history (cough, fever, dyspnea, sputum) + new infiltrate on chest radiography
The sensitivity/specificity of physical examination alone is only 58% and 67% respectively.
Imaging
| Modality | Role |
|---|---|
| CXR (PA + lateral) | First-line; determines extent, detects complications (cavitation, effusion, pneumothorax) |
| CT chest (HRCT) | More sensitive; detects infiltrates up to 5 days earlier than CXR; used if CXR normal but clinical suspicion high, or to rule out alternative diagnoses |
False-negative CXR occurs in: early disease, neutropenia, hypovolemia, PCP (Pneumocystis jirovecii)
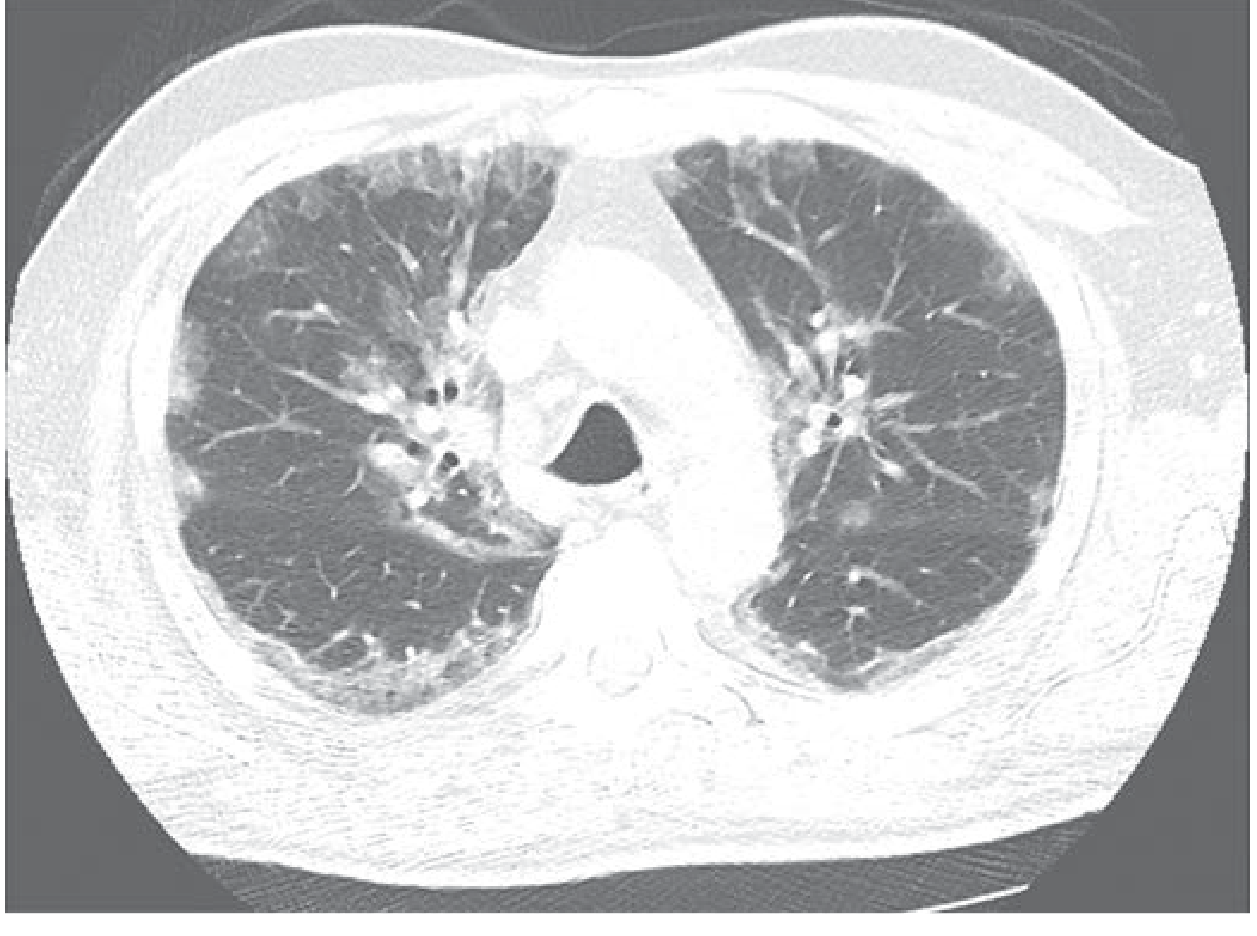
CT Images of Viral Pneumonia
CT - Influenza pneumonia (peripheral ground-glass opacities):
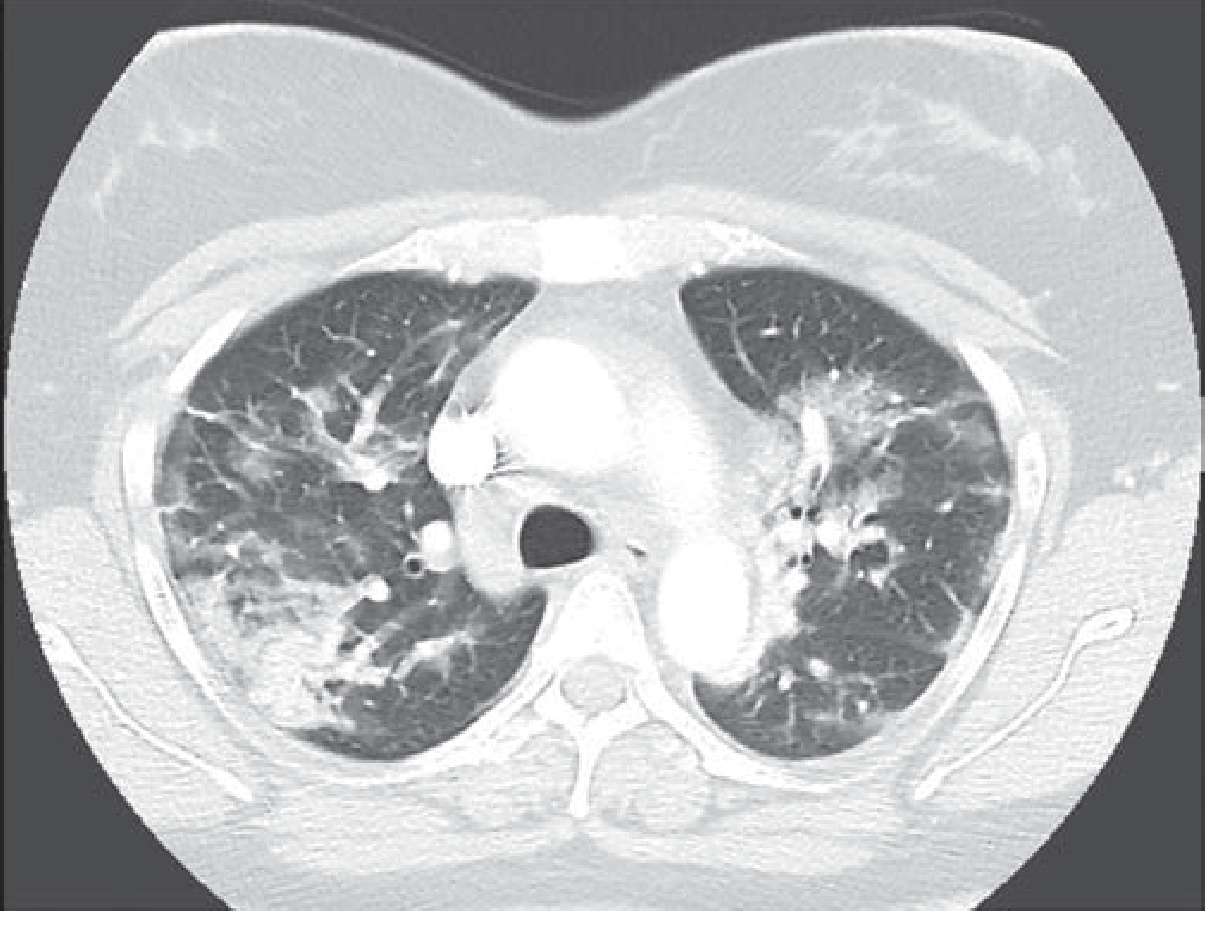
CT - COVID-19 pneumonia (bilateral ground-glass opacities + consolidation):
Laboratory (for hospitalized patients)
- Blood cultures (before antibiotics) - low yield (~14%) but important
- Sputum Gram stain + culture (if quality sputum obtainable)
- Urine antigen tests: S. pneumoniae antigen (high sensitivity/specificity), Legionella antigen
- Nasopharyngeal swab/PCR: influenza, SARS-CoV-2, RSV
- Inflammatory markers: CRP and procalcitonin (PCT) - PCT is insufficiently accurate alone and should NOT be used to withhold antibiotics
Microbiological gram stain (microscopy):
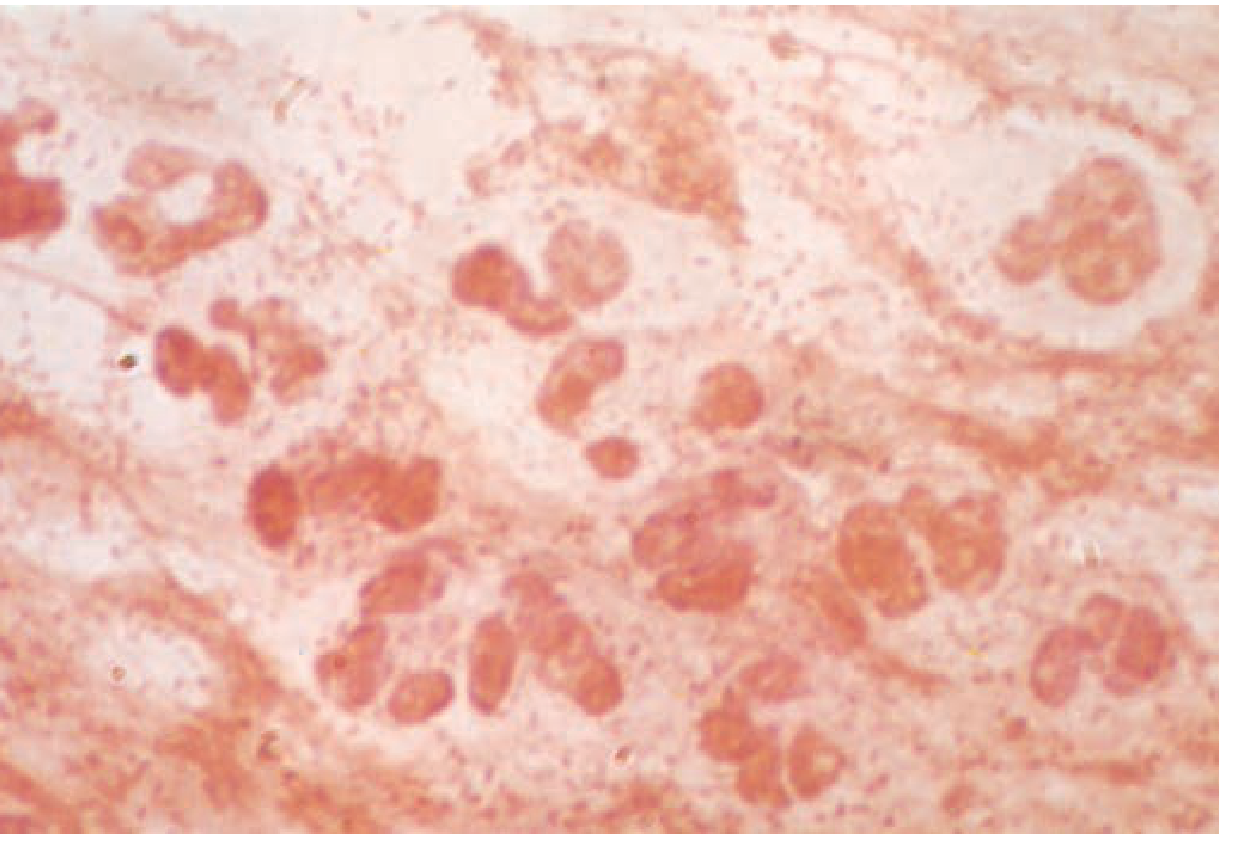
Sputum from pneumococcal lobar pneumonia - Gram-positive lancet-shaped diplococci with polymorphonuclear leukocytes.
Severity Scoring (Site-of-Care Decision)
CURB-65 (simpler, bedside)
| Letter | Criterion |
|---|---|
| C | Confusion (new onset) |
| U | Urea >7 mmol/L (BUN >19 mg/dL) |
| R | Respiratory rate ≥30/min |
| B | Blood pressure: systolic ≤90 or diastolic ≤60 mmHg |
| 65 | Age ≥65 years |
- Score 0 → outpatient (30-day mortality ~1.5%)
- Score 1-2 → hospitalize (unless solely due to age ≥65)
- Score ≥3 → consider ICU (mortality ~22%)
PSI (Pneumonia Severity Index)
- More validated and accurate than CURB-65 but complex (20 variables)
- Classes I-V; Class V mortality = 29.2%
Direct ICU admission criteria
- Septic shock requiring vasopressors
- Acute respiratory failure requiring mechanical ventilation
- Or ≥3 of 9 minor criteria (tachypnea, hypoxemia, multilobar infiltrates, confusion, uremia, leukopenia, thrombocytopenia, hypothermia, hypotension)
Complications (High-Yield)
| Complication | Notes |
|---|---|
| Parapneumonic effusion / Empyema | Most common with S. pyogenes, S. aureus |
| Lung abscess | Cavitation with air-fluid level; anaerobes, S. aureus, Klebsiella |
| Bacteremia | Occurs in ~25-30% of pneumococcal CAP |
| ARDS | Bilateral infiltrates; PaO2/FiO2 <300 |
| Respiratory failure | May require mechanical ventilation |
| Septic shock | End-organ failure |
High-Yield Exam Mnemonics
CURB-65 = severity scoring for CAP
Classic pathogens by setting:
- Young, healthy, walking pneumonia → Mycoplasma
- Elderly, community → S. pneumoniae
- Post-influenza, cavitation → S. aureus
- Alcoholic, upper lobe, "currant jelly" sputum → Klebsiella
- Nosocomial/ventilated → Pseudomonas, Acinetobacter, MRSA
- Hyponatremia + GI symptoms → Legionella
- Immunocompromised (HIV, CD4 <200) → Pneumocystis jirovecii
Stages of lobar pneumonia: Congestion → Red hepatization → Gray hepatization → Resolution (Come Right Go Rest)
Sources: Harrison's Principles of Internal Medicine 22E (2025) Ch. 131 | Fishman's Pulmonary Diseases and Disorders Ch. 122 | Grainger & Allison's Diagnostic Radiology Ch. 5
This is a shared conversation. Sign in to Orris to start your own chat.