Headache medicine
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough overview of headache types and diagnosis, drawn from multiple medical textbooks.
Overview of Headache: Types & Diagnosis
Classification: Primary vs. Secondary
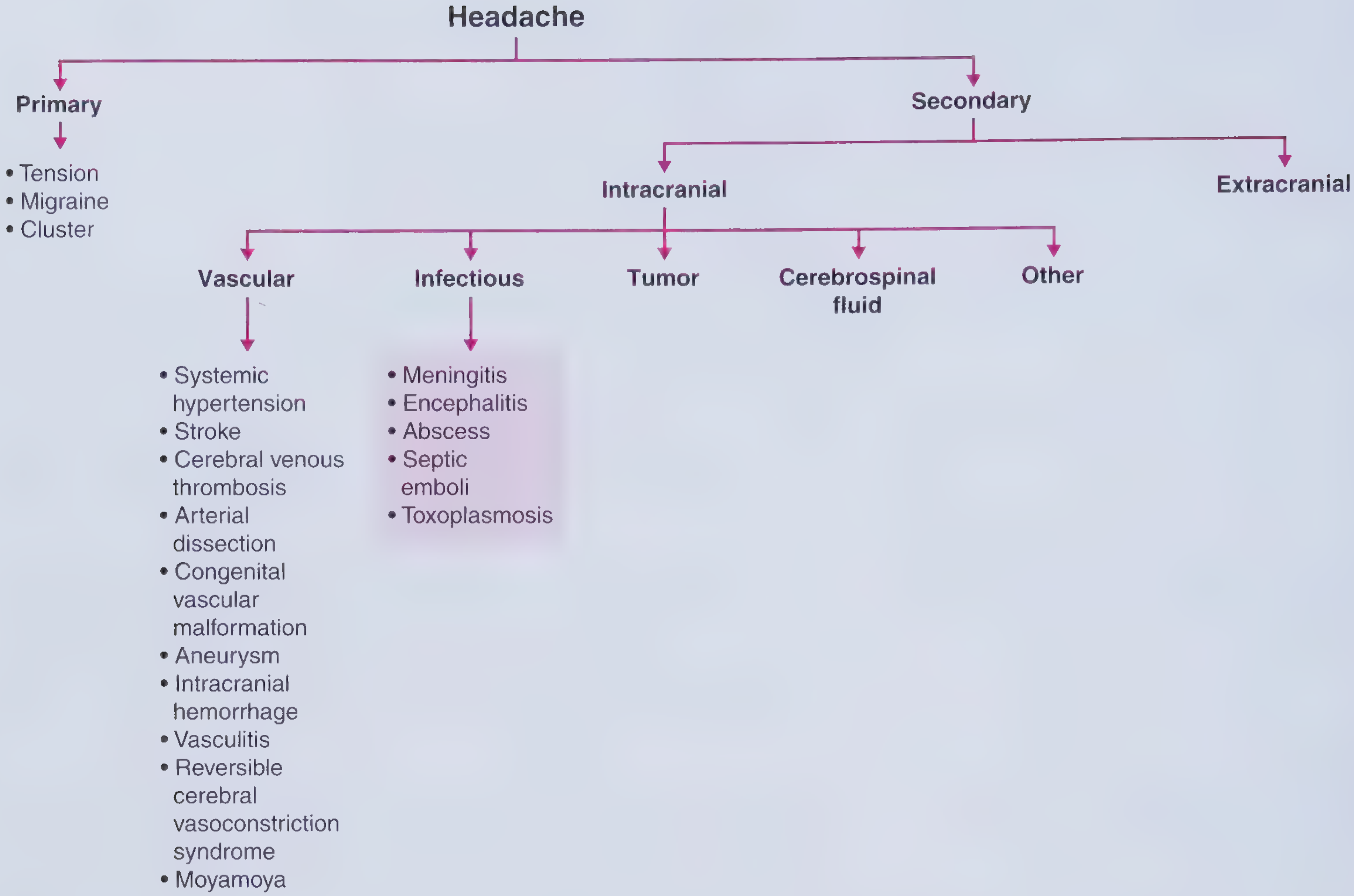
All headaches divide into two broad categories:
- Primary - the headache IS the disorder; no structural cause. Includes migraine, tension-type, and cluster headache.
- Secondary - the headache is a symptom of something else (vascular, infectious, tumor, CSF pressure disorders, extracranial causes).
Primary Headache Types
1. Migraine
| Feature | Details |
|---|---|
| Epidemiology | More common in women; strong genetic component |
| Pain quality | Unilateral or bilateral; throbbing; moderate to severe |
| Duration | Hours to days |
| Worsens with | Physical activity |
| Associated symptoms | Photophobia, phonophobia, nausea/vomiting |
| Aura | ~30% of patients - visual, sensory, motor, or language disturbances preceding the headache |
Migraine with complicated features ("complicated migraine") can produce transient focal deficits from cortical spreading depression - including hemiplegia, aphasia, visual loss. These should be diagnoses of exclusion after ruling out stroke or epilepsy.
2. Tension-Type Headache
| Feature | Details |
|---|---|
| Epidemiology | Equal in men and women |
| Pain quality | Dull, band-like pressure; bilateral; mild to moderate |
| Duration | Hours to days |
| Worsens/improves | Improves with activity (opposite of migraine) |
| Associated symptoms | No nausea/vomiting; at most mild light OR sound sensitivity, not both |
The name was changed from "tension headache" to reflect that muscle tension is NOT the primary mechanism.
3. Cluster Headache (Trigeminal Autonomic Cephalgia)
| Feature | Details |
|---|---|
| Epidemiology | 4x more common in men |
| Pain quality | Extremely severe, unilateral, "boring" pain behind one eye |
| Duration | 30-90 minutes per attack; recurs in clusters over weeks |
| Associated symptoms | Ipsilateral: tearing, eye redness, ptosis, miosis (partial Horner's), nasal congestion, flushing |
| Neurobiology | Posterior hypothalamic activation during attacks |
Other trigeminal autonomic cephalgias (TACs) include paroxysmal hemicrania (shorter, responds specifically to indomethacin) and SUNCT/SUNA (very brief attacks, male-predominant, more frequent).
4. Medication Overuse Headache (MOH)
A common secondary/complication pattern - headache occurring >15 days/month in the setting of frequent analgesic or triptan use. Often coexists with chronic migraine.
Secondary Headache - When to Suspect It
The following are red flags ("SNOOP" features) that should prompt workup for secondary causes (Goldman-Cecil Medicine):
- New headache beginning at older age, without prior history or family history
- Unexplained worsening of previously existing migraine
- "Worst headache of my life" - sudden onset (thunderclap)
- Headaches awakening patient from sleep (except cluster)
- Worse when recumbent, upright, or with Valsalva maneuver
- Focal neurologic deficits that persist after headache resolves
- New headache in setting of HIV, malignancy, or pregnancy
- Abnormal neurologic or new psychiatric findings on exam
Thunderclap Headache
Defined as sudden-onset severe headache reaching maximum intensity immediately or within 1 minute. Key causes include:
- Subarachnoid hemorrhage (most feared)
- Intracerebral hemorrhage
- Cerebral venous thrombosis
- Arterial dissection
- Reversible cerebral vasoconstriction syndrome (RCVS)
- Pituitary apoplexy
- Meningitis
Diagnostic Approach
History - five key elements:
- Family history - genetic predisposition
- Life history - new vs. longstanding headache pattern
- Attack history - quality, location, timing, triggers
- Medical/psychiatric history - comorbidities that worsen headache
- Medication history - drug-induced or overuse headache
Imaging:
- CT scan - first choice for acute severe headache (rules out hemorrhage quickly)
- MRI - better for persistent headaches; detects mass lesions, hemosiderin, Chiari malformation, ICP changes
- CT angiography or MR angiography - if RCVS or vascular malformation is suspected
Lab work:
- ESR and/or CRP in patients >60 years with new/unusual headache - to rule out giant cell arteritis
- CSF (lumbar puncture) - if intracranial hypertension, meningitis, or subarachnoid hemorrhage suspected (especially if CT is negative but thunderclap headache)
Frequency-Based Classification
| Category | Frequency |
|---|---|
| Episodic headache | <15 days/month |
| Chronic headache | ≥15 days/month |
Risk factors for progression to chronic headache: female sex, migraine type, high baseline frequency, obesity, low education level, and analgesic overuse.
Sources: Neuroanatomy through Clinical Cases, 3rd ed.; Goldman-Cecil Medicine, International Edition; Frameworks for Internal Medicine
Would you like to go deeper into any specific type - such as migraine diagnosis, cluster headache management, or secondary headache workup? I can also cover acute treatment medications or preventive therapies if helpful.
This is a shared conversation. Sign in to Orris to start your own chat.