Make notes on Hydatid Cyst for Surgical residency final exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple surgical textbooks. Let me compile the complete exam notes.
Hydatid Cyst (Echinococcosis) - Surgical Residency Final Exam Notes
Sources: Sabiston Textbook of Surgery (21st ed.), Bailey & Love's Short Practice of Surgery (28th ed.), Maingot's Abdominal Operations (12th ed.)
1. Etiology & Life Cycle
Causative organism: Echinococcus granulosus (most common) - a cestode (tapeworm). Less common: E. multilocularis (alveolar/more aggressive), E. ligartus.
Life cycle:
- Definitive host: Dog (or other carnivore) - adult tapeworm lives in the proximal small bowel attached by hooklets, releases thousands of ova daily in feces
- Intermediate host: Sheep (natural), Humans (accidental)
- Human infection: Ingestion of ova via contact with dogs, contaminated water, or vegetables grown at ground level
- In the human duodenum, the embryo (oncosphere) releases hooklets, penetrates the mucosa, enters the portal bloodstream, and lodges in the liver (first filter) or lungs
- No human-to-human transmission
Endemic regions: Mediterranean, Middle East, Far East, South America, Australia, New Zealand, East Africa
2. Pathology & Cyst Structure
Growth rate: Cysts grow to 1 cm in the first 6 months, then 2-3 cm annually.
Cyst wall - 3 layers:
| Layer | Name | Characteristics |
|---|---|---|
| Outermost (host-derived) | Pericyst (Exocyst/Adventitia) | Fibrous capsule from host reaction; blood vessels and bile ducts become incorporated as it grows; calcifies over time |
| Middle | Ectocyst (Laminated membrane) | Bluish-white, gelatinous, ~0.5 cm thick; chitinous structure without nuclei; acts as bacterial barrier and protein ultrafilter |
| Inner (parasite-derived) | Endocyst (Germinal/Germinal layer) | 10-25 μm thick; produces hydatid fluid, ectocyst, brood capsules, scoleces, and daughter cysts |
Key contents:
- Brood capsules: Small intracystic masses from the germinal layer; contain developing protoscoleces
- Protoscolex: Has 4 suckers and double row of hooks; in definitive host → adult tapeworm; in intermediate host → new hydatid cyst
- Hydatid sand: Free-floating brood capsules + protoscoleces + calcareous bodies in hydatid fluid (~400,000 scoleces/mL); appears hyperechogenic on USG
- Daughter cysts: True replicas of mother cyst; formed as a defense reaction to injury (endogenic vesiculation)
- Hydatid fluid: Sterile, colorless, antigenic; contains salts, enzymes, proteins, and toxic substances
E. multilocularis difference: Ectogenic vesiculation (germinal layer extrudes outward through membrane defects) → multilocular appearance, invasive, center becomes necrotic and gelatinous, often lethal.
3. Distribution
| Site | Frequency |
|---|---|
| Liver | 50-75% (most common) |
| Lungs | 20-25% |
| Kidney, spleen, brain, bone | 5-10% |
- 75% are in the right lobe of liver
- 75% are solitary
- Though solitary, 50% contain daughter cysts (multilocular)
- Echinococcal infection is the most common cause of liver cysts worldwide
4. Clinical Features
Usually asymptomatic until complications occur (average age at diagnosis ~45 years; equal sex distribution)
Symptoms:
- Abdominal pain (most common)
- Dyspepsia, vomiting
- Palpable hepatomegaly (most frequent sign)
- Jaundice and fever (~8% each)
Emergency presentations:
- Anaphylactic shock from cyst rupture (potentially fatal)
- Coughing up white material (scoleces) from hepatic cyst rupturing through diaphragm into bronchial tree
- Severe abdominal pain after minor trauma
Complications:
- Bacterial superinfection → mimics pyogenic abscess
- Rupture into biliary tree → biliary colic, jaundice, cholangitis
- Rupture into bronchial tree → cough, hemoptysis
- Free rupture into peritoneum/pleura/pericardium → disseminated echinococcosis, anaphylaxis
- Calcification of cyst wall (does NOT always mean cyst is dead)
5. Investigations
Blood Tests
- Eosinophilia (raised eosinophil count)
- Serology: ELISA, immunoelectrophoresis, Casoni skin test (historical) - plagued by low sensitivity and specificity
Imaging
Ultrasound - first choice worldwide (availability, affordability, ~90% specificity):
- Hydatid sand (free-floating hyperechogenic foci)
- "Water lily sign" / floating membrane (split wall = detached laminated membrane)
- Rosette/honeycomb/cartwheel appearance (daughter cysts)
- Eggshell calcification
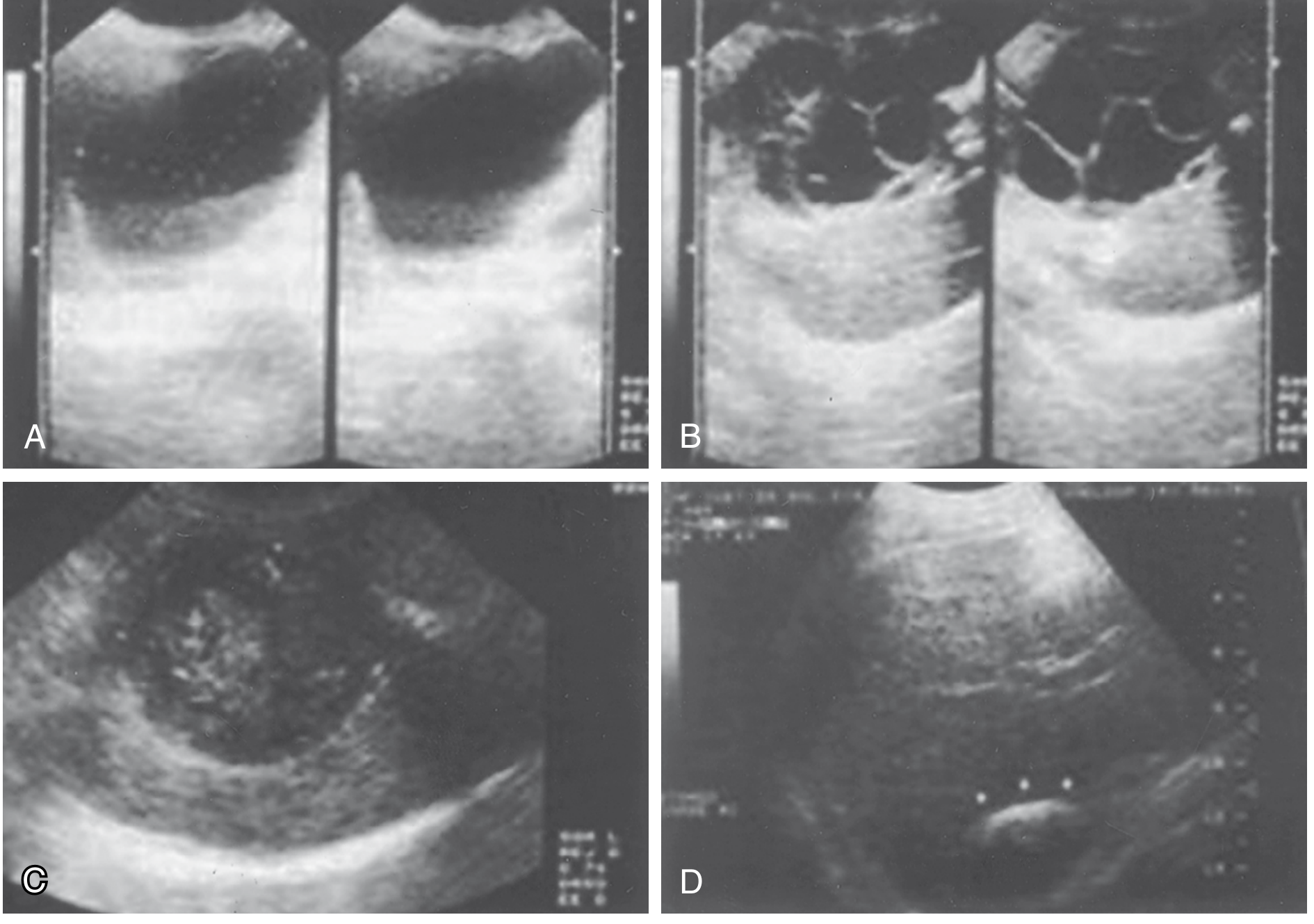
WHO/Gharbi USG Classification (CE Staging):
| Stage | Description |
|---|---|
| CL | Unilocular anechoic cyst, no internal echoes or septations |
| CE1 | Anechoic cyst with fine internal echoes (hydatid sand) |
| CE2 | Internal septations; multivesicular/honeycomb/cartwheel/rosette formation |
| CE3a | Daughter cysts with detached laminated membrane |
| CE3b | Daughter cysts inside solid matrix (transitional) |
| CE4 | No visible daughter cysts; hypo/hyperechoic mixture ("bag of wool") - inactive |
| CE5 | Partial or complete calcification of wall - inactive/degenerative |
CT scan - best single modality:
- Space-occupying lesion with smooth outline and septa
- Daughter cysts clearly seen
- Calcified thick walls
- Evaluates extrahepatic extension
- Required for operative planning (especially laparoscopic)
MRI - adds structural detail, shows biliary communication, superior soft-tissue contrast but expensive
ERCP/MRCP - demonstrates communication between cysts and biliary tree; MRCP may show multiple cysts communicating with biliary system; ERCP can drain biliary tree before surgery
Chest X-ray - elevated diaphragm, concentric wall calcifications (limited value)
Important: FNAC/percutaneous aspiration was historically contraindicated (risk of anaphylaxis + spillage), but PAIR technique has superseded this dogma.
6. Differential Diagnosis of Liver Cysts
| Feature | Pyogenic | Amebic | Hydatid | Congenital | Cystadenoma |
|---|---|---|---|---|---|
| Number | Single/multiple | One or few | Usually single | Single/multiple | Single with loculations |
| Wall | Thick | Thick | Thick | Thin | Variable |
| Contents | Pus with blood | Red-brown "anchovy paste" | Clear/bilious, gelatinous | Clear, water density | Green-brown mucinous |
| Wall character | Uniform/multiloculated | Usually uniform | Uniform, daughter cysts; 50% calcified | Uniform | Septations common |
7. Treatment
Principles
- Eradication of the parasite within the cyst
- Protection of the host against spillage of scoleces
- Management of complications (biliary communication etc.)
Decision-making
- Small cysts (<4 cm), deep, uncomplicated → conservative management
- Asymptomatic, inactive cysts (CE4/CE5) → monitor with USG
- Active cysts → treat with albendazole first, then definitive intervention
- Elderly patients with small, asymptomatic, densely calcified cysts → conservative management
Medical Therapy
Drug of choice: Albendazole (benzimidazole group)
- Readily absorbed from intestine, metabolized by liver to active form
- Alone: only ~30% successful
- Given for at least 3 months preoperatively
- Post-operatively for at least 1 month if spillage, partial removal, or biliary rupture occurred
- Reduces recurrence rate
- Mebendazole - poorly absorbed, inactivated by liver; second choice
Praziquantel - also used (available on "named patient" basis in some countries)
PAIR (Minimally Invasive)
PAIR = Puncture, Aspiration, Injection, Re-aspiration
- Done under USG or CT guidance
- Steps: Puncture cyst wall → Aspirate cyst contents → Inject contrast (to opacify and check for biliary communication) → Infuse scolicidal agent → Re-aspirate
- Scolicidal agents used: 15-20% hypertonic saline, 95% ethanol, 30% saline + 95% ethanol combination, povidone-iodine
- Preceded by adequate course of albendazole
- Success rate comparable to surgery in selected patients
- Contraindicated if biliary communication present (sclerosing cholangitis risk)
Surgical Treatment
Preoperative preparation:
- Albendazole course
- Preoperative steroids (recommended by some)
- Epinephrine and steroids on standby for anaphylaxis
- Pack off abdomen to prevent spillage
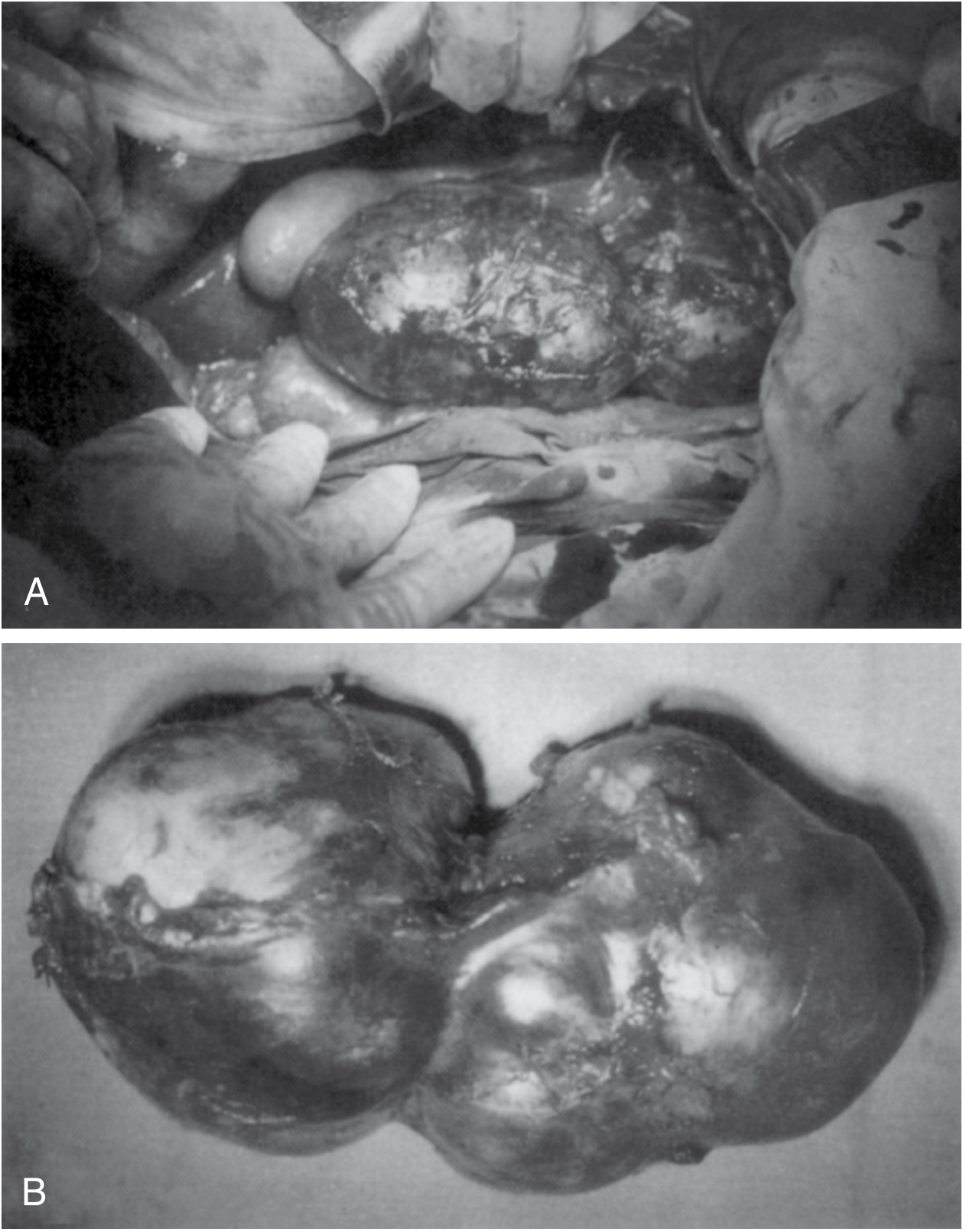
Operative steps (general):
- Complete abdominal exploration
- Mobilize liver and expose cyst
- Pack off surrounding abdomen (anaphylaxis risk + seeding)
- Aspirate through closed suction system
- Inject scolicidal agent (hypertonic saline 15-20%, or 75-95% ethanol, or 5% povidone-iodine)
- Unroof the cyst
Conservative (drainage) procedures:
- Marsupialization - deroofing + drainage
- Laparoscopic marsupialization - removal of endocyst + daughter cysts (most common minimal access approach)
- Omentoplasty (fills residual cavity)
- External drainage
Radical (resection) procedures:
- Pericystectomy (partial or total) - removal of entire cyst including pericyst
- Hepatic segmentectomy/partial hepatectomy - for peripheral cysts
- Both approaches (radical vs. conservative) appear equally effective at controlling disease
Biliary communication management:
- Meticulous search for biliary communication pre/intra-operatively
- Simple suture repair often sufficient
- Major biliary repairs, common bile duct approaches, or postoperative ERCP as needed
- ERCP can drain biliary tree before surgery
Recurrence rate: 1-20%, generally <5% in experienced centers
Laparoscopic approach: Increasingly used; requires CT for operative planning; laparoscopic marsupialization/deroofing with endocyst removal is standard minimal access technique.
8. Scolicidal Agents - Summary
| Agent | Concentration | Notes |
|---|---|---|
| Hypertonic saline | 15-20% | Most commonly used |
| Ethanol | 75-95% | Effective |
| Povidone-iodine | 5% (some use 10%) | Risk of sclerosing cholangitis if biliary communication |
| Saline + Ethanol combination | 30% + 95% | Used for PAIR |
Warning: Scolicidal agents + biliary communication = risk of sclerosing cholangitis
9. Complications of Surgery
- Anaphylactic shock (from spillage)
- Disseminated echinococcosis (secondary seeding from spillage)
- Biliary fistula / bile leak
- Sclerosing cholangitis (if scolicidal agent contacts bile ducts)
- Residual cavity infection
- Recurrence (1-20%)
10. High-Yield Exam Points
| Point | Key Fact |
|---|---|
| Most common cause of liver cysts worldwide | Echinococcal infection |
| Definitive host | Dog |
| Accidental intermediate host | Humans |
| Most common organ affected | Liver (50-75%), right lobe (75%) |
| Second most common organ | Lungs (20-25%) |
| Most common presenting symptom | Abdominal pain |
| Most frequent clinical sign | Hepatomegaly |
| Emergency presentation | Anaphylactic shock from rupture |
| Best imaging modality | CT scan (for planning); USG (worldwide, first choice) |
| Pathognomonic USG sign | Daughter cysts / "rosette" / floating membrane ("water lily sign") |
| Calcification | Does NOT always mean dead cyst |
| Drug of choice | Albendazole |
| Scolicidal agent of choice | Hypertonic saline 15-20% |
| PAIR contraindication | Biliary communication |
| Risk of scolicidal agent in biliary communication | Sclerosing cholangitis |
| Surgery preparation | Albendazole pre-op + pack off abdomen |
| Recurrence rate | 1-20% (<5% in expert centers) |
| E. multilocularis vs. granulosus | Alveolar, invasive, no pericyst, often lethal; ectogenic vesiculation |
| Hydatid sand | 400,000 scoleces/mL of fluid |
| "Bag of wool" appearance on USG | CE4 - inactive/degenerative stage |
11. Prevention
- Wash hands after contact with canines
- Avoid consuming vegetables grown at ground level (in endemic areas)
- Do NOT feed entrails of slaughtered animals to dogs (interrupts life cycle)
- Public education programs have reduced incidence in endemic areas
Sources: Sabiston Textbook of Surgery, p.1891-1892 | Bailey & Love's Short Practice of Surgery 28th Ed., p.95-100 | Maingot's Abdominal Operations 12th Ed., p.933-937
Create a printable PDF quick-reference card for exam day
Reading File
Running Command
Running Command
Writing File
Running Command
Running Command
Running Command
Writing File
Editing File
Running Command
Running Command
Running Command
1 page, 9 KB. Your quick reference card is ready.
Hydatid Cyst Quick Reference
PDF Document · PDF
Here's what's packed into the single A4 page in a two-column layout:
Left column:
- Overview & Aetiology (organism, hosts, transmission, endemic regions)
- Life Cycle (5-step numbered sequence)
- Cyst Wall - 3 Layers table (Pericyst / Ectocyst / Endocyst with descriptions)
- Distribution table (Liver 50-75%, Lungs 20-25%, Other 5-10%)
- Clinical Features (elective, emergency, and complications)
Right column:
- Investigations (blood tests + USG signs)
- WHO/Gharbi CE Staging table (CL, CE1-CE5 with USG description and activity status)
- CT / MRCP / ERCP notes
- Differential Diagnosis of Liver Cysts table
- Treatment Algorithm (watchful waiting vs. PAIR vs. surgery)
- PAIR steps + scolicidal agents + warning box for biliary communication
- Surgical options table (conservative vs. radical)
- Medical Therapy (Albendazole, Mebendazole, Praziquantel)
- High-Yield Exam Facts table (14 key mnemonics)
Print at A4, 100% scale. Good luck on the exam!
This is a shared conversation. Sign in to Orris to start your own chat.