Gross Anatomy of spleen
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive data from multiple authoritative textbooks. Let me compile a complete, well-structured answer.
Gross Anatomy of the Spleen
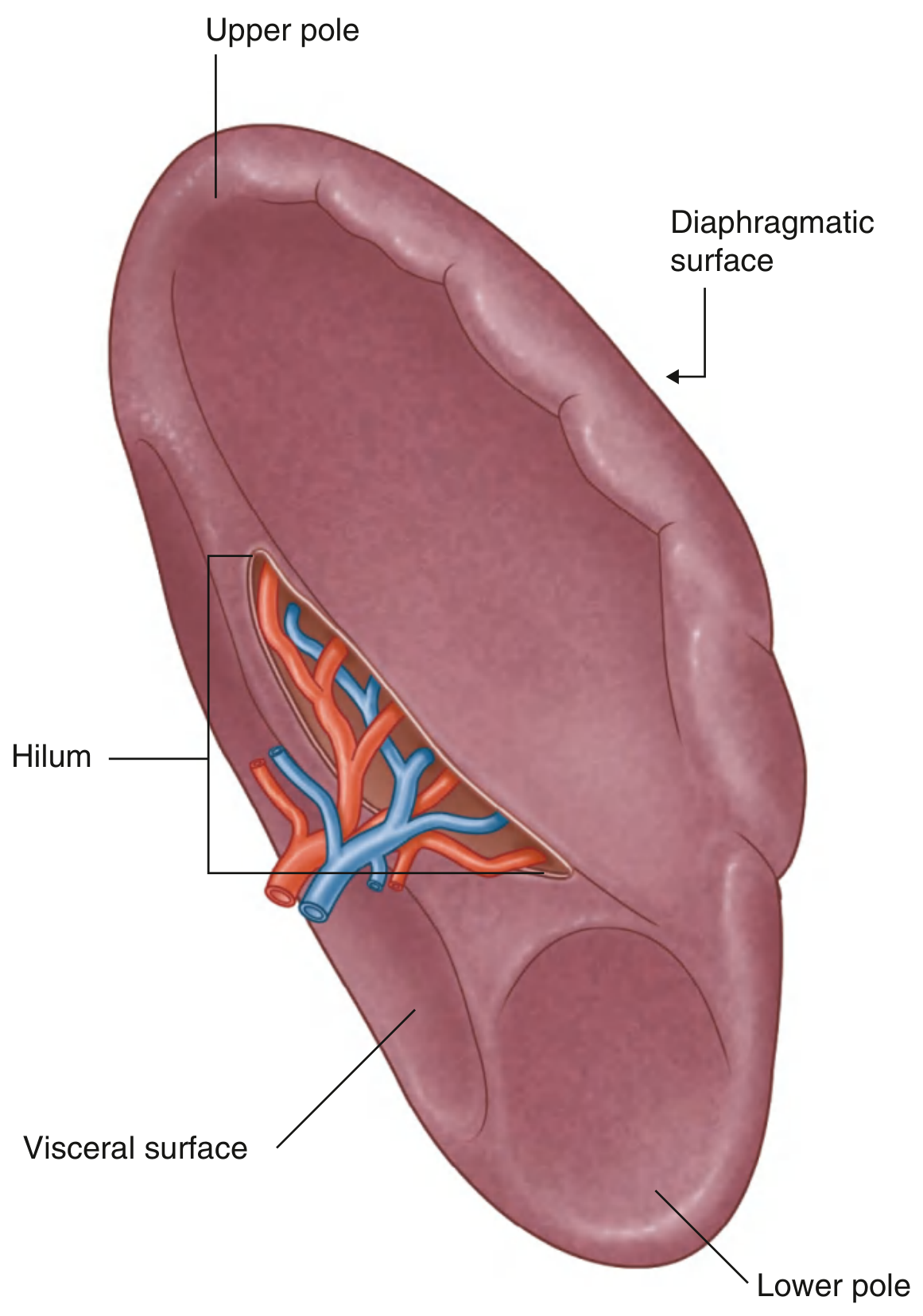
Fig. 4.115 - Surfaces and Hilum of the Spleen (Gray's Anatomy for Students)
Overview
The spleen is the largest lymphoreticular/reticuloendothelial organ in the body. It is also the largest secondary lymphoid organ, situated intraperitoneal in the left hypochondriac region. Unlike lymph nodes, it acts as a filter within the blood circulation rather than the lymphatic system.
- Shape: coffee-bean / kidney-shaped
- Size: 10-13 cm in length, 6-8 cm wide, 3-4 cm thick
- Weight: 150-200 g (range 70-250 g) in a healthy adult; decreases with age
- Colour: soft, bluish-red (fresh state)
Embryological Development
The spleen arises from the primitive mesoderm as an outgrowth of the left side of the dorsal mesogastrium (the mesentery suspending the developing stomach). It becomes recognizable by week 5 of gestation (in an embryo ~8 mm long). Key milestones:
- Day 12 embryonic: formation of the splanchnic mesodermal plate
- Week 2 of gestation: colonized by erythroid and myeloid progenitor cells
- Up to month 5 of fetal life: major hematopoietic organ (erythropoiesis and myelopoiesis)
- After birth: hematopoietic function ceases (may persist in pathological states like myelofibrosis)
- It migrates to the left upper quadrant with its smooth diaphragmatic surface facing posterosuperiorly
Position and Relations
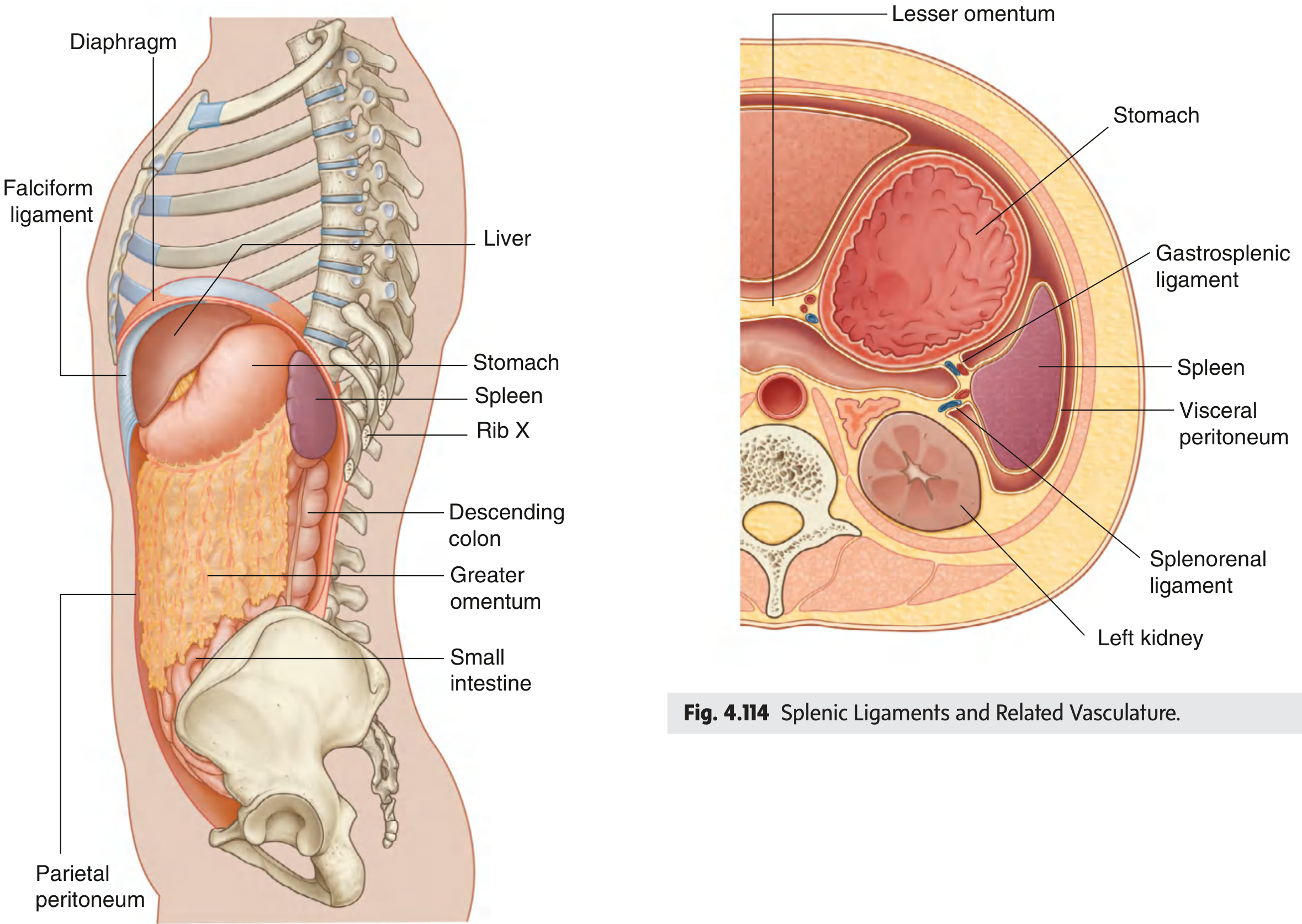
Fig. 4.113/4.114 - Position and ligamentous relations of the spleen (Gray's Anatomy for Students)
The spleen lies:
- Behind ribs 9-11 in the left lateral chest wall, protected by them
- Its long axis is parallel to the 10th rib
- Its posterior pole is ~2 cm from the body of T10 vertebra
- In healthy adults it is not palpable below the costal margin
- Covered by visceral peritoneum except at the hilum
Surfaces
| Surface | Characteristics |
|---|---|
| Diaphragmatic surface | Convex; faces posterosuperiorly; smooth; lies against the left dome of the diaphragm (which separates it from the left lung, pleura, and ribs 9-11) |
| Visceral surface | Concave; faceted; faces anteroinferiorly toward the abdominal cavity; bears 4 impressions |
Visceral Surface Impressions
- Gastric impression - largest; against the fundus and body of the stomach (anterosuperior to hilum)
- Renal impression - posterior to hilum; against the upper pole of the left kidney
- Colic impression - inferior; against the splenic flexure of the colon
- Pancreatic impression - against the tail of the pancreas (near the hilum)
Borders and Poles
| Structure | Description |
|---|---|
| Superior border (anterior margin) | Narrow and notched (1-2 notches); separates diaphragmatic from gastric surface; notches are palpable when the spleen is greatly enlarged (splenomegaly) |
| Inferior border | Broad and blunt; faces posteroinferiorly |
| Upper (posterior) pole | Rounded; reaches ~2 cm from T10 body |
| Lower (anterior) pole | Extends nearly to the midaxillary line; normally not palpable |
Clinical point: The notch on the superior border is palpable in massive splenomegaly and helps distinguish an enlarged spleen from a left kidney (which lacks a notch).
The Splenic Hilum
The hilum is a long, narrow fissure on the visceral surface through which:
- Splenic artery and vein enter/exit
- Lymphatic vessels and nerves pass
- The tail of the pancreas may reach the hilum (present in ~30% of individuals, within 1 cm in ~70%)
The hilum divides the visceral surface into:
- Posterior to hilum - renal impression (left kidney contact)
- Anterior to hilum - gastric impression (stomach and pancreatic tail contact)
Peritoneal Ligaments
The spleen is held in position by several peritoneal ligaments (both the gastrosplenic and splenorenal ligaments are parts of the greater omentum):
| Ligament | Connects | Contents | Vascularity |
|---|---|---|---|
| Gastrosplenic (gastrolienal) | Hilum to greater curvature of stomach | Short gastric vessels (superior part); left gastroepiploic/gastro-omental vessels (inferior part) | Vascular |
| Splenorenal (lienorenal) | Hilum to left kidney / posterior abdominal wall | Splenic artery and vein; tail of pancreas | Vascular |
| Splenophrenic (phrenosplenic) | Diaphragmatic surface to diaphragm | Relatively avascular (in absence of portal hypertension) | Avascular |
| Splenocolic | Inferior pole to splenic flexure of colon | Relatively avascular | Avascular |
| Phrenicocolic | Left colic flexure to lateral body wall | - | Forms "floor" of a sling supporting the spleen |
Vascular Supply
Arterial Supply
- Splenic artery: largest branch of the celiac trunk; highly tortuous; runs along the posterior superior border of the pancreas
- Gives 16-18 pancreatic branches en route
- Two anatomical types at the hilum:
- Magistral type (30%): single trunk that divides near the hilum
- Distributed type (70%): arborizes proximally, well before the hilum
- Terminally branches into 4-6 polar arteries (lobar/segmental arteries) and 6 short gastric arteries
Venous Drainage
- Splenic vein: formed by union of several intrasplenic veins + left gastroepiploic vein
- Runs posterior to the pancreas
- Joins the superior mesenteric vein (+ inferior mesenteric vein) to form the portal vein
Nerve Supply
- Sympathetic fibers from the celiac plexus travel along the splenic artery
Lymphatic Drainage
- Lymphatics drain to pancreaticosplenic lymph nodes around the splenic vessels, then to celiac nodes
Capsule and Internal Architecture (Brief)
- The spleen is encased in a fibroelastic capsule with smooth muscle fibers
- From the capsule, trabeculae extend inward, compartmentalizing the parenchyma
- The parenchyma consists of:
- White pulp - lymphatic sheaths (PALS) and lymphoid follicles around arterioles; site of immune responses
- Red pulp - vascular sinuses, venous sinusoids, and splenic cords; site of blood filtration
Accessory Spleens (Splenunculi)
- Present in up to 20% of the general population; up to 30% in patients with hematologic disease
- Usually pea-sized to egg-sized
- >80% located at the splenic hilum and vascular pedicle
- Other sites (in decreasing frequency): gastrocolic ligament, pancreatic tail, greater omentum, greater curvature of stomach, splenocolic ligament, bowel mesentery, left broad ligament (females), left spermatic cord (males)
- Clinically important: accessory spleens must be removed in splenectomy for hematologic conditions (e.g., ITP) to prevent relapse
Clinical Correlates
| Feature | Clinical Significance |
|---|---|
| Rib cage protection (ribs 9-11) | Rib fractures are the most common cause of splenic laceration |
| Intraperitoneal location | Splenic rupture causes hemoperitoneum |
| Phrenicocolic ligament | Supports spleen; if disrupted, "wandering spleen" can occur |
| Notch on superior border | Palpable in splenomegaly; distinguishes spleen from kidney |
| Tail of pancreas at hilum | Risk of pancreatic injury during splenectomy |
| Short gastric vessels (in gastrosplenic ligament) | Must be ligated in splenectomy; can cause gastric ischemia if accidentally divided |
Sources:
- Color Atlas of Human Anatomy, Vol. 2 (Internal Organs), Gross Anatomy section
- Gray's Anatomy for Students, Ch. 4 (Abdomen)
- Sabiston Textbook of Surgery, 21e - Splenic Anatomy
- Schwartz's Principles of Surgery, 11e - Embryology and Anatomy of the Spleen
Classification and Clinical Significance of Plasma Proteins Biochemistry
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
I now have comprehensive data from Harper's Biochemistry, Tietz, Guyton & Hall, and Medical Physiology. Let me compile the complete answer.
Classification and Clinical Significance of Plasma Proteins
1. Introduction
Plasma contains a complex mixture of proteins with a total concentration of 7.0-7.5 g/dL, generating a colloid osmotic (oncotic) pressure of ~25 mmHg. The original classification by early scientists divided plasma proteins into fibrinogen, albumin, and globulins based on solubility. Modern cellulose acetate zone electrophoresis separates the serum protein fraction into 5 major bands:
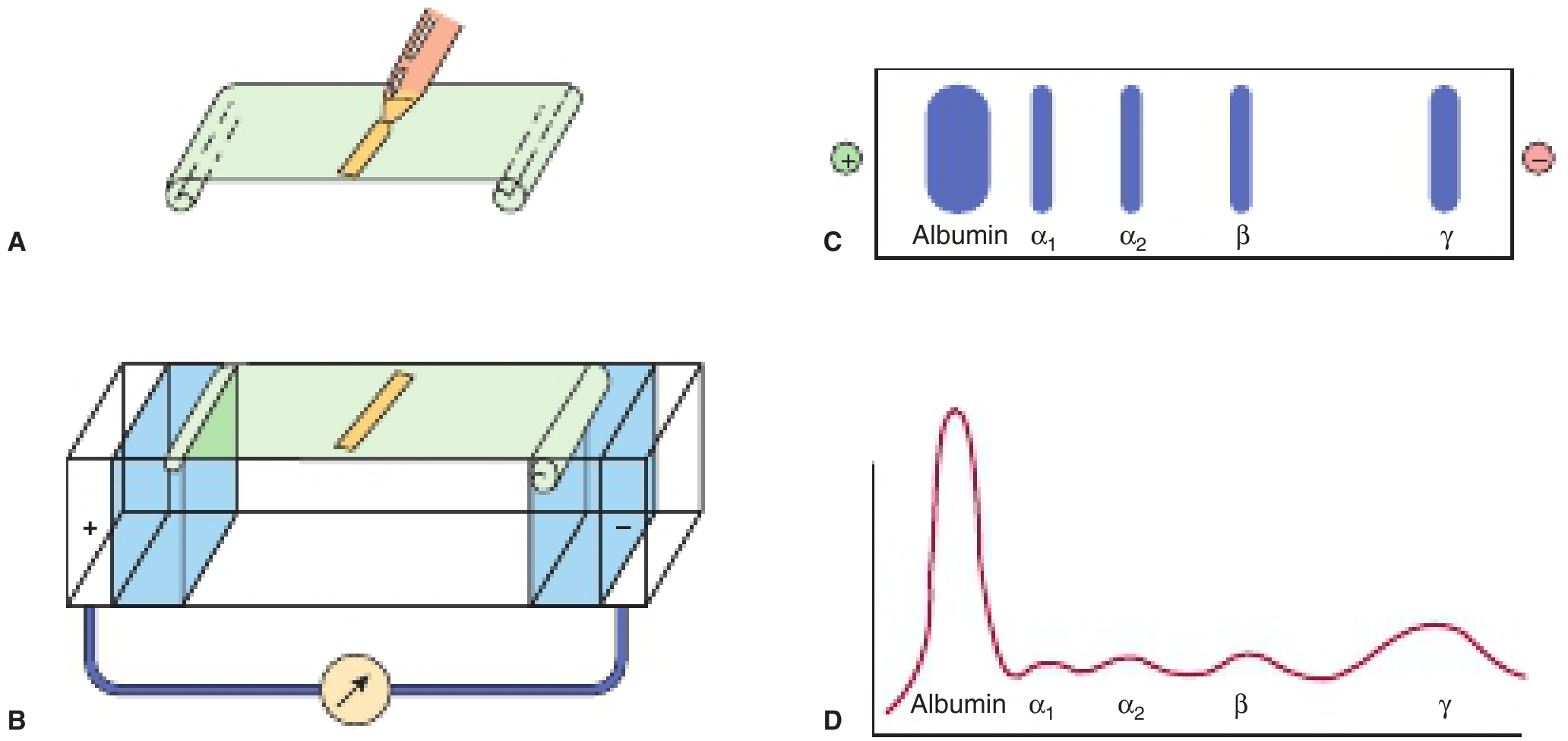
FIGURE 52-1: Cellulose acetate zone electrophoresis showing the 5 major plasma protein fractions: Albumin, α1-, α2-, β-, and γ-globulins (Harper's Illustrated Biochemistry, 32e)
2. Classification of Plasma Proteins
A. By Electrophoretic Mobility (Clinical Standard)
| Fraction | % of Total | Key Proteins |
|---|---|---|
| Albumin | ~60% | Albumin |
| α1-globulins | ~4% | α1-antitrypsin, α1-acid glycoprotein (orosomucoid), α1-fetoprotein |
| α2-globulins | ~8% | Haptoglobin, α2-macroglobulin, ceruloplasmin |
| β-globulins | ~12% | Transferrin, LDL (β-lipoprotein), complement components (C3, C4), fibrinogen |
| γ-globulins | ~16% | Immunoglobulins (IgG, IgA, IgM, IgD, IgE) |
B. By Function
| Functional Class | Key Members |
|---|---|
| Maintenance of oncotic pressure | Albumin |
| Transport/carrier proteins | Albumin, transferrin, ceruloplasmin, haptoglobin, hemopexin, transthyretin, retinol-binding protein, sex hormone-binding globulin (SHBG), thyroxine-binding globulin (TBG), corticosteroid-binding globulin (CBG), vitamin D-binding protein |
| Coagulation factors | Fibrinogen, prothrombin, factors V, VII, VIII, IX, X, XI, XII, XIII |
| Anticoagulants/inhibitors | Antithrombin III, protein C, protein S, α1-antitrypsin, α2-macroglobulin |
| Immunoproteins (antibodies) | IgG, IgA, IgM, IgD, IgE |
| Complement proteins | C1 through C9, factors B, D, H, I |
| Acute phase reactants | C-reactive protein (CRP), fibrinogen, haptoglobin, α1-acid glycoprotein, α1-antitrypsin, ceruloplasmin, serum amyloid A |
| Enzymes in plasma | Lipase, amylase, cholinesterase, alkaline phosphatase |
C. By Site of Synthesis
| Source | Proteins Made |
|---|---|
| Liver (~70-80% of all plasma proteins) | Albumin, fibrinogen, transferrin, prothrombin, coagulation factors (except factor VIII), complement components, α1-antitrypsin, haptoglobin, ceruloplasmin, α2-macroglobulin, CRP, transthyretin |
| Lymphocytes / Plasma cells | All immunoglobulins (γ-globulins) |
| Vascular endothelium | von Willebrand factor |
| Macrophages / monocytes | Complement proteins (C1, C2, C3, C4, properdin, factor B) |
3. Individual Proteins and Their Clinical Significance
ALBUMIN
- MW: 69,000 Da | Half-life: ~20 days | Normal: 3.5-5.0 g/dL
- Functions:
- Maintains plasma oncotic pressure (responsible for ~80% of total oncotic pressure)
- Major transport protein: carries bilirubin, fatty acids, drugs (warfarin, aspirin), hormones, Ca²+, Mg²+, bilirubin
- Acts as a labile protein reserve (amino acid reservoir)
- Negative acute phase reactant - synthesis falls during inflammation (IL-6 suppresses it)
- Clinical significance:
- Hypoalbuminemia → edema, ascites (Starling forces shift fluid to extravascular compartment)
- Seen in: liver cirrhosis, nephrotic syndrome (urinary loss up to 20 g/day), malnutrition, protein-losing enteropathy, burns (liters of protein-rich fluid can be lost daily), chronic infection/inflammation
- Serum albumin is a strong predictor of mortality across many diseases
- Drug binding affected: low albumin → higher free (active) drug levels → toxicity risk
- Albumin-to-globulin (A:G) ratio: normally >1; reversal in liver disease and multiple myeloma
FIBRINOGEN (β-globulin)
- MW: 340,000 Da | Half-life: ~4-6 days | Normal: 200-400 mg/dL
- Functions: Precursor of fibrin; polymerizes into long fibrin threads during coagulation (thrombin cleaves fibrinopeptides A and B to form fibrin monomer)
- Clinical significance:
- Elevated: Acute phase reactant - rises in infection, inflammation, pregnancy, myocardial infarction; independent cardiovascular risk factor
- Decreased/absent: Disseminated intravascular coagulation (DIC), liver failure, afibrinogenemia
- Prothrombin time (PT) / INR measures fibrinogen-dependent coagulation; worsening PT in acute hepatitis = poor prognosis
IMMUNOGLOBULINS (γ-globulins)
- Synthesized exclusively by plasma cells (B lymphocytes)
- IgG: Most abundant; secondary immune response; only Ig that crosses placenta
- IgA: Predominant in secretions (saliva, colostrum, tears)
- IgM: First antibody in primary immune response; pentameric; activates complement most effectively
- IgD: B-cell surface receptor
- IgE: Mediates Type I hypersensitivity; elevated in parasitic infections and allergies
- Clinical significance:
- Polyclonal hypergammaglobulinemia: broad γ-peak; seen in chronic infection, liver cirrhosis, autoimmune disease
- Monoclonal gammopathy (M-spike): narrow sharp peak; seen in multiple myeloma, Waldenström macroglobulinemia, MGUS
- Hypogammaglobulinemia: increased susceptibility to bacterial infections; seen in agammaglobulinemia, common variable immunodeficiency (CVID)
α1-ANTITRYPSIN (α1-globulin)
- MW: ~55 kDa | Major serine protease inhibitor (serpin) in plasma
- Inhibits trypsin, elastase, collagenase, chymotrypsin; protects lung tissue from neutrophil elastase
- Clinical significance:
- Deficiency (homozygous PiZZ genotype): emphysema (unopposed elastase destroys alveoli), liver cirrhosis (abnormal protein accumulates in hepatocytes)
- Elevated as positive acute phase reactant in infection, inflammation
HAPTOGLOBIN (α2-globulin)
- MW: ~100 kDa | Synthesized in liver
- Binds free hemoglobin (from hemolyzed RBCs) → Hb-Hp complex taken up by macrophages → prevents iron and Hb loss in urine
- Half-life of free haptoglobin: ~5 days; Hb-Hp complex: ~90 min (rapidly cleared)
- Clinical significance:
- Decreased or absent: Marker of intravascular hemolysis (haptoglobin consumed faster than it is synthesized) - seen in hemolytic anemia, transfusion reactions, malaria
- Elevated: Positive acute phase reactant; elevated in infections, inflammation
- Elevated in some cancers (haptoglobin-related protein)
TRANSFERRIN (β-globulin)
- MW: ~76 kDa (glycoprotein) | Synthesized in liver
- Transports Fe3+ in the plasma; contains 2 high-affinity binding sites for Fe3+
- Normal plasma [Tf]: ~300 mg/dL → total iron-binding capacity (TIBC) ~300 μg/dL
- Normally ~30% saturated with iron
- Clinical significance:
- Elevated (low % saturation): Iron deficiency anemia (liver makes more transferrin to compensate; TIBC ↑, saturation ↓ <16%)
- Decreased (high % saturation): Iron overload (hemochromatosis; TIBC ↓, saturation >45%)
- Carbohydrate-deficient transferrin (CDT): biomarker of chronic alcoholism
CERULOPLASMIN (α2-globulin)
- MW: ~132 kDa | Copper-containing glycoprotein (ferroxidase activity)
- Carries >90% of plasma copper; also functions as ferroxidase (oxidizes Fe2+ to Fe3+)
- Clinical significance:
- Decreased: Wilson disease (autosomal recessive copper accumulation), Menkes disease, chronic hepatitis, nephrotic syndrome
- Elevated: Pregnancy, estrogen therapy, cholestasis, hemochromatosis, and as a positive acute phase reactant
- Low ceruloplasmin + Kayser-Fleischer rings + neuropsychiatric symptoms = Wilson disease
C-REACTIVE PROTEIN (CRP) (β/γ region)
- MW: ~115 kDa; pentameric protein
- Named because it reacts with the C-polysaccharide of Streptococcus pneumoniae
- Synthesized in liver; one of the most sensitive acute phase reactants
- Activates the classical complement pathway
- Normal: <10 mg/L; rises 100-1000-fold within hours of infection/tissue injury
- Clinical significance:
- Elevated: Bacterial infection, MI, autoimmune disease, malignancy, post-surgery
- Useful in: monitoring antibiotic response, distinguishing bacterial vs. viral infection (CRP much higher in bacterial)
- High-sensitivity CRP (hsCRP): cardiovascular risk stratification
- Notable: CRP stays normal/low in systemic lupus erythematosus (SLE) unless infection is present
α-FETOPROTEIN (AFP)
- Normal fetal plasma protein; falls to adult levels by 1 year of age
- Clinical significance:
- Mild increase → hepatocellular regeneration in acute/chronic hepatitis
- Markedly elevated → Hepatocellular carcinoma (HCC) (tumor marker)
- Also elevated in: yolk sac tumors (germ cell), neural tube defects (in maternal serum), Down syndrome (low AFP)
TRANSTHYRETIN (Prealbumin)
- MW: ~55 kDa | Half-life: 24-48 hours (shortest of all liver-made proteins)
- Transports thyroxine (T4) and retinol (via retinol-binding protein complex)
- Clinical significance:
- Short half-life makes it the most sensitive indicator of current hepatic synthetic function and nutritional status
- Decreased: malnutrition, liver disease (cirrhosis), acute inflammation
- Serial monitoring used in nutritional assessment (better than albumin due to short half-life)
α2-MACROGLOBULIN
- MW: ~720 kDa (largest plasma protein)
- Broad-spectrum protease inhibitor; "traps" proteases (trypsin, chymotrypsin, plasmin, thrombin)
- Clinical significance:
- Elevated in nephrotic syndrome (too large to be lost in urine, so relative increase while smaller proteins are lost)
- Elevated in liver disease and diabetes
4. Acute Phase Response
During tissue injury or infection, the acute phase response causes changes in plasma protein concentrations driven primarily by IL-1, IL-6, and TNF-α from macrophages acting on the liver:
| Positive Acute Phase Proteins (Increase) | Negative Acute Phase Proteins (Decrease) |
|---|---|
| CRP (up to 1000x increase) | Albumin |
| Fibrinogen | Transthyretin (prealbumin) |
| Haptoglobin | Transferrin |
| α1-antitrypsin | Retinol-binding protein |
| α1-acid glycoprotein (orosomucoid) | |
| Ceruloplasmin | |
| Serum amyloid A (SAA) | |
| Complement components | |
| Ferritin |
Clinical pearl: Albumin and transthyretin fall in acute phase states, which is why a low albumin may reflect acute inflammation rather than malnutrition alone.
5. Serum Protein Electrophoresis (SPEP) Patterns - Clinical Correlates
| Disease | Characteristic SPEP Pattern |
|---|---|
| Normal | Albumin peak large; γ-band small/moderate |
| Liver cirrhosis | Albumin ↓; β-γ bridging (IgA elevation); polyclonal γ ↑ |
| Nephrotic syndrome | Albumin ↓; α2-macroglobulin ↑; γ ↓ |
| Multiple myeloma | Narrow "M-spike" (monoclonal band) in β or γ region |
| Acute infection | α1, α2, fibrinogen ↑; albumin ↓ |
| Chronic inflammation | Polyclonal γ ↑ |
| Agammaglobulinemia | γ fraction absent |
| Iron deficiency | Transferrin ↑ (β-band ↑) |
6. Half-Lives of Key Plasma Proteins
| Protein | Half-life | Clinical Use |
|---|---|---|
| CRP | ~19 hours | Monitoring acute infection response |
| Transthyretin | 24-48 hours | Sensitive nutritional/hepatic function marker |
| Fibrinogen | 4-6 days | Coagulation; acute phase marker |
| Haptoglobin-Hb complex | ~90 minutes | Rapidly consumed in hemolysis |
| Albumin | ~20 days | Long-term nutritional and hepatic status |
| IgG | ~21 days | Most long-lived immunoglobulin |
| IgM | ~5 days | - |
Sources:
- Harper's Illustrated Biochemistry, 32e, Chapter 52 (Plasma Proteins)
- Tietz Textbook of Laboratory Medicine, 7e, Chapters 22 & 51
- Guyton & Hall Textbook of Medical Physiology, Functional Roles of Plasma Proteins
- Medical Physiology (Boron & Boulpaep), Plasma Proteins section
DLC in physiology
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive data. Let me compile the full DLC answer.
Differential Leukocyte Count (DLC) - Physiology
Overview
The Differential Leukocyte Count (DLC) is the percentage of each type of white blood cell (WBC) among the total WBC count. The total WBC count in a normal adult is 4,500-11,000 cells/µL of blood (approximately 7,000/µL on average), compared to ~5 million RBCs/µL.
WBCs are divided into two major groups based on cytoplasmic granule content:
- Granulocytes (polymorphonuclear cells) - have abundant specific granules and a polymorphic/multilobed nucleus
- Agranulocytes - lack specific granules; have a spherical or indented (not lobed) nucleus
Classification of WBCs
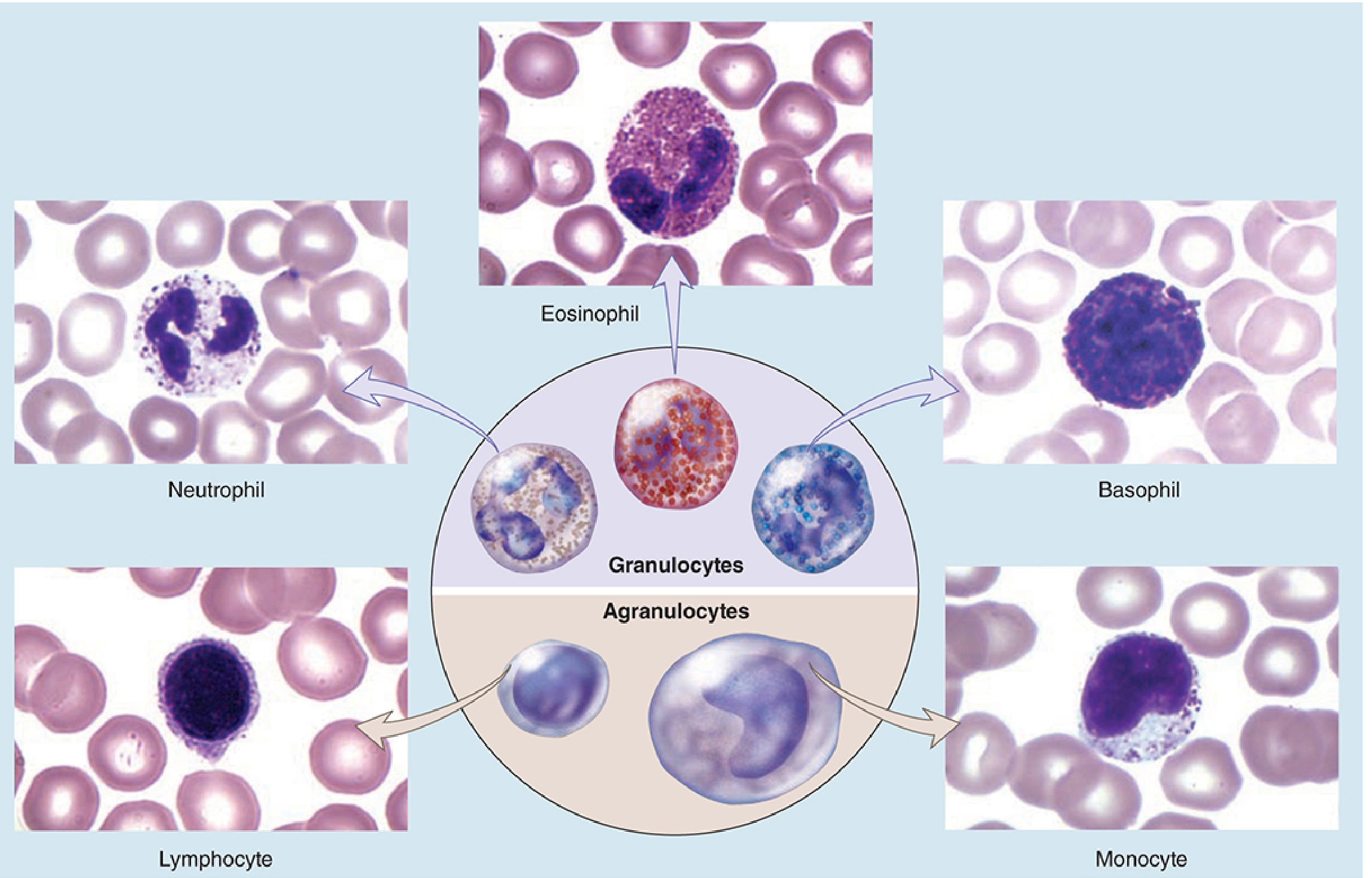
Fig 12-1: Types of leukocytes - granulocytes and agranulocytes (Junqueira's Basic Histology, 17e)
Normal DLC Values
| Cell Type | % (Guyton & Hall) | % (USMLE/NBME Range) | Absolute Count (cells/µL) |
|---|---|---|---|
| Neutrophils | 62% | 50-70% | 3,000-7,000 |
| Eosinophils | 2.3% | 1-4% | 150-400 |
| Basophils | 0.4% | 0.5-1% | 0-100 |
| Monocytes | 5.3% | 2-8% | 200-800 |
| Lymphocytes | 30% | 20-40% | 1,500-4,000 |
Memory mnemonic: "Never Let Monkeys Eat Bananas" - Neutrophils (60%), Lymphocytes (30%), Monocytes (6%), Eosinophils (3%), Basophils (1%)
Genesis of WBCs
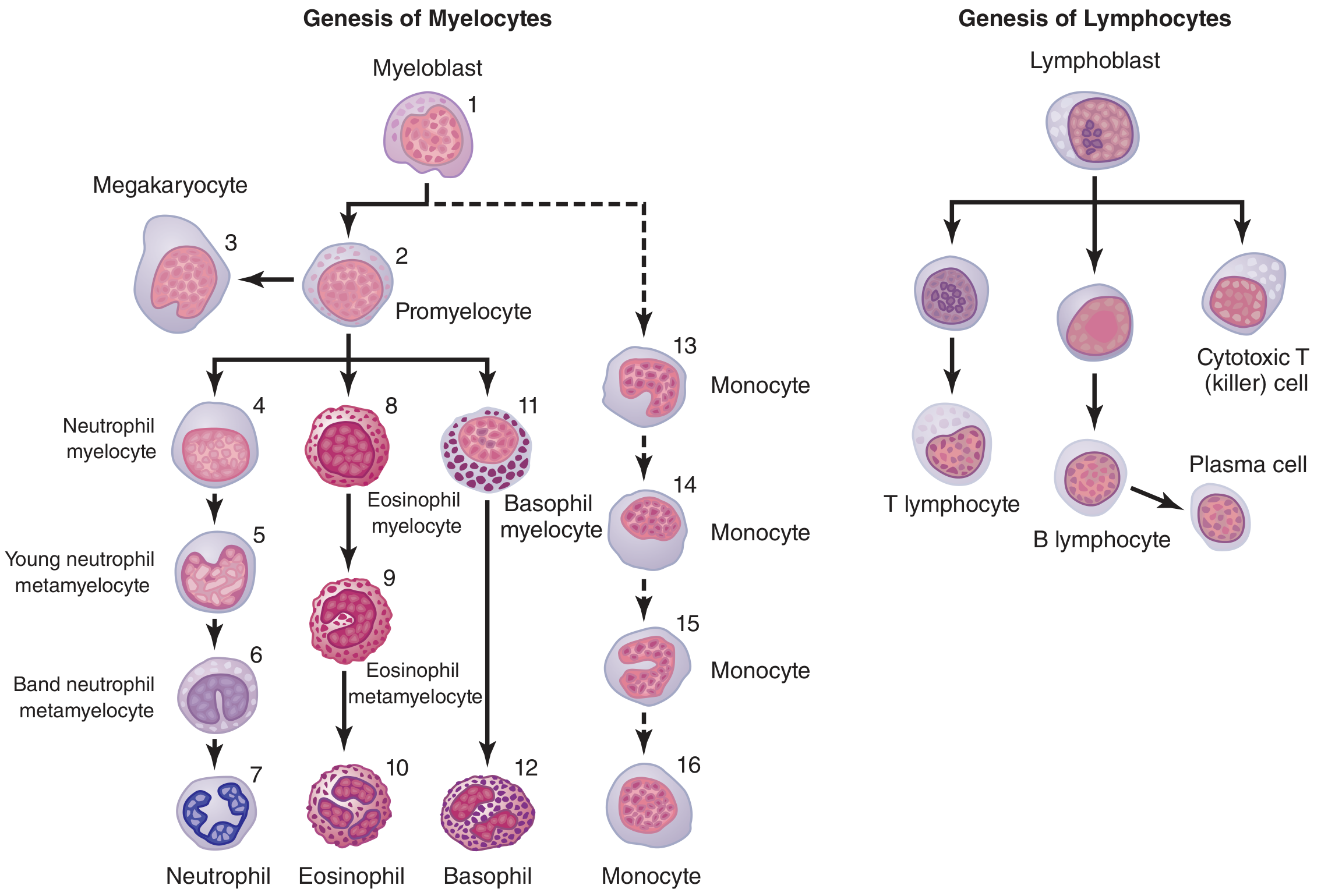
Figure 34.1: Genesis of white blood cells - myelocytic and lymphocytic lineages (Guyton & Hall, 14e)
Two major lineages:
- Myelocytic lineage (bone marrow): Myeloblast → Promyelocyte → Myelocyte → Metamyelocyte → Band cell → Mature granulocyte/Monocyte
- Lymphocytic lineage (bone marrow + lymphoid tissues): Lymphoblast → T and B lymphocytes, plasma cells
Individual WBCs - Morphology, Function, and Clinical Significance
1. NEUTROPHILS (Polymorphonuclear Neutrophils / PMNs)
| Feature | Detail |
|---|---|
| Normal % | 50-70% |
| Size | 12-15 µm |
| Nucleus | 3-5 lobes connected by thin chromatin strands |
| Granules | Faint/light pink; neutral-staining |
| Life span in blood | 4-8 hours; in tissues: 4-5 days (shortened to hours during acute infection) |
| Origin | Bone marrow (myelocytic lineage) |
Granule types:
- Primary (azurophilic) granules - lysosomes containing myeloperoxidase, defensins, lysozyme, elastase
- Secondary (specific) granules - lactoferrin, collagenase, B12-binding proteins, alkaline phosphatase
Functions:
- First responders in acute bacterial infection (arrive within minutes to hours)
- Phagocytosis of bacteria, fungi, cellular debris
- Chemotaxis - migrate toward sites of infection following chemotactic signals (C5a, IL-8/CXCL8, LTB4, fMLP)
- Diapedesis - squeeze through endothelial gaps via P-selectin/integrin interactions
- Oxidative burst (respiratory burst): NADPH oxidase generates superoxide → H2O2 → hypochlorous acid (HOCl) via myeloperoxidase
Clinical significance:
| Condition | Change |
|---|---|
| Bacterial infection | Neutrophilia + left shift (band forms) |
| Viral infection | Neutropenia |
| CML (chronic myeloid leukemia) | Massive neutrophilia |
| Aplastic anemia, chemotherapy | Neutropenia → severe infection risk |
| Hereditary hypersegmentation | B12/folate deficiency (>5 lobes) |
"Left shift": Appearance of band (stab) neutrophils and immature forms in the blood, indicating accelerated marrow release. Normal band neutrophils = 3-5%.
2. EOSINOPHILS
| Feature | Detail |
|---|---|
| Normal % | 1-4% |
| Size | 12-17 µm |
| Nucleus | Bilobed ("spectacle" shape) |
| Granules | Bright red/dark pink (acidophilic); contain major basic protein (MBP), eosinophil cationic protein (ECP), eosinophil peroxidase |
| Life span | 1-2 weeks in tissues |
| Origin | Bone marrow |
Functions:
- Kill helminthic parasites (worms too large to phagocytose): degranulate and release MBP directly onto parasite surface
- Modulate inflammation in allergic reactions: produce prostaglandins, leukotrienes; take up antigen-antibody complexes
- Phagocytose antigen-antibody complexes
- Respond to IL-5 (from Th2 cells) for proliferation and differentiation
Clinical significance:
| Condition | Change |
|---|---|
| Parasitic infections (helminths) | Eosinophilia |
| Allergic conditions (asthma, urticaria, hay fever) | Eosinophilia |
| Drug hypersensitivity | Eosinophilia |
| Addison's disease (adrenal insufficiency) | Eosinophilia (cortisol suppresses eosinophils normally) |
| Steroid therapy | Eosinopenia |
| Acute bacterial/viral infection | Eosinopenia |
"NAACP" mnemonic for eosinophilia: Neoplasm, Asthma/Allergy, Addison's disease, Collagen vascular disease, Parasites
3. BASOPHILS
| Feature | Detail |
|---|---|
| Normal % | 0.5-1% (least common WBC) |
| Size | 10-14 µm |
| Nucleus | Bilobed or S-shaped (often obscured by granules) |
| Granules | Large, dark blue/purple (strongly basophilic); contain heparin, histamine, serotonin, leukotrienes |
| Life span | 1-3 days in tissues |
| Origin | Bone marrow |
Functions:
- Carry IgE receptors (FcεRI) on their surface - central to Type I hypersensitivity (anaphylaxis, atopy)
- On cross-linking of IgE by antigen → degranulation → histamine release (vasodilation, bronchoconstriction, itching)
- Release heparin (local anticoagulant), serotonin, SRS-A (slow reacting substance of anaphylaxis = LTC4, LTD4, LTE4)
- Functionally related to mast cells in tissues (mast cells are tissue-resident counterparts)
Clinical significance:
| Condition | Change |
|---|---|
| Allergic reactions, anaphylaxis | Basophilia (degranulation) |
| CML | Basophilia (pathognomonic finding) |
| Hypothyroidism | Basophilia |
| Polycythemia vera | Basophilia |
| Hyperthyroidism | Basopenia |
| Steroid therapy, stress | Basopenia |
4. MONOCYTES
| Feature | Detail |
|---|---|
| Normal % | 2-8% |
| Size | 15-20 µm (largest WBC in blood) |
| Nucleus | Kidney-shaped, indented, or horseshoe-shaped (C-shaped); no lobes |
| Granules | None specific (azurophilic granules only) |
| Life span in blood | 10-20 hours |
| Life span in tissues | Months to years (as macrophages) |
| Origin | Bone marrow (monocytic lineage) |
Functions:
- Immature phagocytes in blood - limited phagocytic ability while in circulation
- Exit blood → enter tissues → differentiate into tissue macrophages (swell up to 60-80 µm)
- Macrophages perform: phagocytosis of bacteria/dead cells/debris, antigen presentation (MHC II), cytokine secretion, activation of adaptive immunity
Tissue macrophage names by location:
| Location | Macrophage Name |
|---|---|
| Liver | Kupffer cells |
| Lung | Alveolar macrophages |
| Brain | Microglia |
| Skin | Langerhans cells (histiocytes) |
| Kidney | Mesangial cells |
| Bone | Osteoclasts |
| Connective tissue | Histiocytes |
| Spleen, lymph nodes | Fixed macrophages (RES) |
All macrophages together with monocytes form the Reticuloendothelial System (RES) - also called the Monocyte-Macrophage System
Clinical significance:
| Condition | Change |
|---|---|
| Viral infections (EBV, CMV) | Monocytosis |
| Tuberculosis, brucellosis | Monocytosis |
| SLE, RA | Monocytosis |
| Monocytic leukemia (AML-M5) | Monocytosis |
| Aplastic anemia, acute infections | Monocytopenia |
5. LYMPHOCYTES
| Feature | Detail |
|---|---|
| Normal % | 20-40% (2nd most common) |
| Size | 7-12 µm (small); 12-16 µm (large) |
| Nucleus | Large, spherical, densely stained; occupies most of the cell |
| Cytoplasm | Scant, light blue |
| Granules | None (agranulocyte) |
| Life span | Hours to many years (memory cells) |
| Origin | Bone marrow; mature in thymus (T cells) or bone marrow/GALT (B cells) |
Types and functions:
| Subtype | Marker | Function |
|---|---|---|
| T lymphocytes | CD3+; 65-80% of lymphocytes | Cell-mediated immunity; helper (CD4+), cytotoxic (CD8+), regulatory (Treg) |
| B lymphocytes | CD19+, CD20+; 10-15% | Humoral immunity; differentiate into plasma cells → antibody production |
| NK cells (Natural Killer) | CD16+, CD56+; ~10% | Kill virus-infected cells and tumor cells without prior sensitization |
Clinical significance:
| Condition | Change |
|---|---|
| Viral infections (EBV, CMV, hepatitis) | Lymphocytosis + atypical (reactive) lymphocytes |
| Pertussis (whooping cough) | Absolute lymphocytosis |
| CLL (chronic lymphocytic leukemia) | Massive lymphocytosis |
| ALL (acute lymphoblastic leukemia) | Lymphoblasts in blood |
| HIV/AIDS | CD4+ lymphopenia |
| Severe combined immunodeficiency (SCID) | Lymphopenia |
| Steroid therapy, radiotherapy | Lymphopenia |
Summary Table
| Cell | % | Nucleus | Granules | Key Function | ↑ In | ↓ In |
|---|---|---|---|---|---|---|
| Neutrophil | 50-70 | 3-5 lobes | Faint pink | Bacteria killing, phagocytosis | Bacterial infection | Viral infection, aplastic anemia |
| Eosinophil | 1-4 | Bilobed | Red/dark pink | Antiparasitic, allergy modulation | Parasites, allergy | Steroid therapy, acute infection |
| Basophil | 0.5-1 | Bilobed/S-shape | Dark blue-purple | IgE-mediated hypersensitivity, heparin | CML, allergy | Stress, steroids |
| Monocyte | 2-8 | Kidney/C-shaped | None (agranular) | Precursor of macrophages, phagocytosis | TB, viral, SLE | Aplastic anemia |
| Lymphocyte | 20-40 | Spherical, large | None (agranular) | Adaptive immunity (T & B cells) | Viral, CLL, ALL | AIDS, steroids |
Life Spans
| Cell | Blood | Tissues |
|---|---|---|
| Neutrophil | 4-8 hours | 4-5 days (hours if infected) |
| Eosinophil | Hours | 1-2 weeks |
| Basophil | Hours | 1-3 days |
| Monocyte | 10-20 hours | Months-years (as macrophages) |
| Lymphocyte | Hours (recirculate) | Weeks to years (memory cells) |
Diapedesis and Chemotaxis (How WBCs Reach Infection Sites)
- Margination - WBCs move to periphery of vessel (slow rolling)
- Pavementing - WBCs stick to endothelium via P-selectin (expressed on endothelium) binding glycosylated ligands on WBCs
- Adhesion - Firm attachment via integrins (ICAM-1/LFA-1 interaction)
- Diapedesis - WBCs squeeze through gaps between endothelial cells (postcapillary venules)
- Chemotaxis - Migration toward chemoattractants: C5a, IL-8 (CXCL8), LTB4, fMLP (bacterial peptides)
Sources:
- Guyton & Hall Textbook of Medical Physiology, 14e, Chapter 34 - General Characteristics of Leukocytes
- Junqueira's Basic Histology, 17e, Chapter 12 - Leukocytes
- Henry's Clinical Diagnosis and Management by Laboratory Methods - Differential Leukocyte Count
Create a study guide comparing normal vs. abnormal DLC patter
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.