MI
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"myocardial infarction"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Here is a full overview of Myocardial Infarction (MI) drawn from Robbins & Kumar Pathologic Basis of Disease, Guyton & Hall Textbook of Medical Physiology, and Ganong's Review of Medical Physiology, with 2025 guideline updates.
Myocardial Infarction (MI) - Full Overview
Definition & Epidemiology
MI is the death of cardiac muscle due to prolonged ischemia. It affects roughly 800,000 people in the United States each year (nearly one MI every 40 seconds), causing approximately 400,000 deaths annually. The major underlying cause is atherosclerosis. About 10% of MIs occur in people under 40 years of age, and 45% in people under 65. Male sex is a risk factor through middle age; premenopausal females are largely protected, but postmenopausal women lose this protection due to declining estrogen, rising cholesterol, and increasing inflammatory markers.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 511
Pathogenesis
Typical sequence (atherothrombotic - ~90% of cases)
- An atheromatous plaque is eroded or suddenly disrupted by endothelial injury, intraplaque hemorrhage, or mechanical forces - exposing subendothelial collagen and necrotic plaque contents to blood.
- Platelets adhere, aggregate, and release thromboxane A2, ADP, and serotonin, causing further aggregation and vasospasm.
- Activation of coagulation by tissue factor adds to the growing thrombus.
- Within minutes, the thrombus can completely occlude the coronary artery lumen.
Angiography performed within 4 hours of onset demonstrates coronary thrombosis in ~90% of cases. Note: the culprit lesion is usually at a site that did NOT previously have a critical (>70%) fixed stenosis.
Atypical causes (~10% of cases)
- Coronary vasospasm (with or without atherosclerosis) - cocaine or ephedrine use
- Embolism (from mural thrombus in AF, infective endocarditis vegetations, prosthetic material, or right-to-left shunt through patent foramen ovale)
- Vasculitis, sickle cell disease, amyloid deposition in vessel walls
Myocardial Response to Ischemia
| Feature | Time |
|---|---|
| Onset of ATP depletion | Seconds |
| Loss of contractility | < 2 minutes |
| ATP reduced to 50% of normal | 10 minutes |
| ATP reduced to 10% of normal | 40 minutes |
| Irreversible cell injury (necrosis) | 20-40 minutes |
| Microvascular injury | > 1 hour |
| Complete necrosis | 6-12 hours |
The subendocardium is most vulnerable - it is the last area perfused and is exposed to high intramural pressures. Necrosis begins subendocardially and spreads outward toward the epicardium in a "wavefront" phenomenon.
- Robbins, p. 512; Guyton & Hall, p. 271
Infarct Distribution by Coronary Artery

| Artery | Frequency | Territory |
|---|---|---|
| Left anterior descending (LAD) | 40-50% | Anterior LV wall near apex, anterior ventricular septum, apex |
| Right coronary artery (RCA) | 30-40% | Inferior/posterior LV wall, posterior septum, posterior RV free wall |
| Left circumflex (LCx) | 15-20% | Lateral LV wall (except apex) |
Morphologic Changes Over Time
| Time | Gross Appearance | Microscopy |
|---|---|---|
| 0-4 hours | None visible | None (may see wavy fibers) |
| 4-12 hours | Pale, dark mottling | Coagulative necrosis begins, edema |
| 12-24 hours | Dark mottling | Pyknosis, contraction bands, neutrophil infiltration |
| 1-3 days | Mottled with yellow-tan center | Dense neutrophil infiltration, nuclear karyolysis |
| 3-7 days | Yellow-tan, hyperemic border | Macrophage infiltration, beginning removal of necrotic debris |
| 1-2 weeks | Yellow-tan, depressed | Granulation tissue - vascularized, with collagen deposition |
| 2-8 weeks | Gray-white scar | Progressive fibrosis |
| > 2 months | Firm scar | Dense collagen scar |
Clinical Presentation
Symptoms:
- Severe, crushing substernal chest pain/pressure radiating to the left arm, jaw, or neck
- Diaphoresis, nausea, vomiting, dyspnea
- ~20-30% are "silent" (especially in diabetics and elderly)
Types:
- STEMI (ST-Elevation MI) - full-thickness (transmural) infarct, complete coronary occlusion; higher mortality (~9% in-hospital)
- NSTEMI (Non-ST-Elevation MI) - partial or transient occlusion, subendocardial infarct; slightly lower mortality (~6% in-hospital)
ECG Changes
The three mechanisms driving ECG changes in acute MI:
| Defect in Infarcted Cells | Current Flow | ECG Change (leads over infarct) |
|---|---|---|
| Rapid repolarization | Out of infarct | ST segment elevation |
| Decreased resting membrane potential | Into infarct | TQ segment depression (recorded as ST elevation) |
| Delayed depolarization | Out of infarct | ST segment elevation |
Key ECG evolution:
-
Acute (hyperacute): Peaked T-waves, then ST elevation in the leads overlying the infarct; reciprocal ST depression in opposite leads
-
Days to weeks: ST segment normalizes; Q waves develop (deep/wide Q waves in transmural MI)
-
Old MI: Persistent Q waves; "failure of R wave progression" in anterior infarcts
-
Ganong's Review of Medical Physiology, p. 534
Cardiac Biomarkers
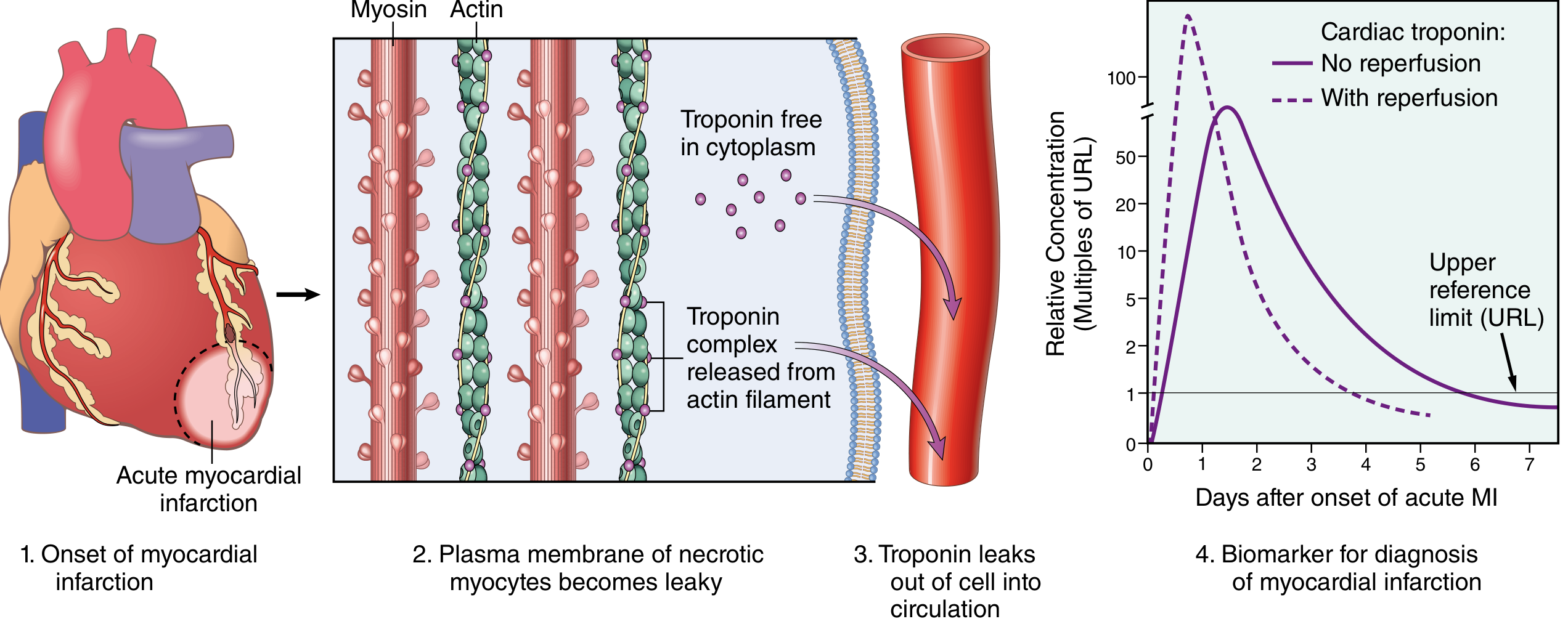
- Troponin I / Troponin T (gold standard): Rise in 2-4 hours, peak at 24-48 hours, remain elevated 7-10 days. With reperfusion, levels are higher but peak earlier (rapid washout from necrotic tissue).
- CK-MB: Rises within 3-6 hours, peaks at 24 hours, normalizes within 48-72 hours.
- Myoglobin: Rises earliest (1-3 hours) but is non-specific.
Troponin "leak" at low levels can occur with myocarditis, PE, renal failure, CHF, and sepsis - serial measurements help distinguish these.
- Robbins, p. 517
Initial Management
| Category | Intervention |
|---|---|
| Oxygen | For hypoxia or respiratory distress (SpO2 < 90%) |
| Antiplatelet | Aspirin + ADP receptor inhibitor (clopidogrel, ticagrelor, or prasugrel); GPIIb/IIIa inhibitors |
| Anticoagulation | UFH, LMWH, direct thrombin inhibitors, or factor Xa inhibitors |
| Nitrates | For vasodilation and reversal of vasospasm |
| Beta-blockers | Reduce myocardial O2 demand and arrhythmia risk (avoid in acute heart failure) |
| Reperfusion | Primary goal - PCI (preferred) or fibrinolysis if PCI unavailable within 120 minutes |
| Supportive | Treat pain, anxiety, hemodynamic abnormalities, arrhythmias |
Key 2025 guideline update: The 2025 ACC/AHA Guideline for Acute Coronary Syndromes (PMID: 40014670) provides updated recommendations on ACS management. Additionally, a 2025 meta-analysis (PMID: 39298680) found that beta-blockers for secondary prevention after MI in patients WITHOUT reduced ejection fraction or heart failure may not provide the same benefit as previously assumed.
- Robbins, p. 517
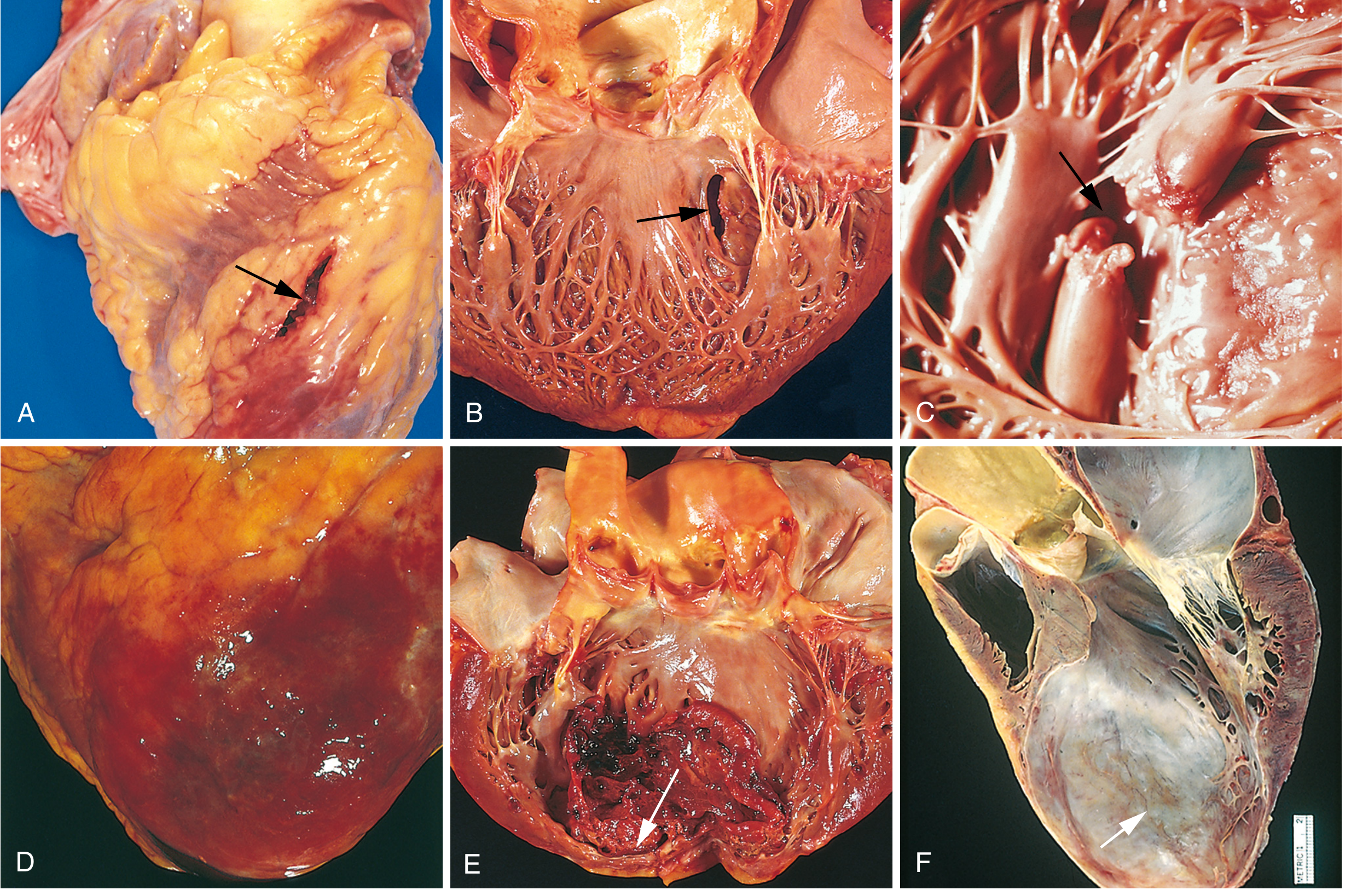
Complications
| Complication | Details |
|---|---|
| Contractile dysfunction / Cardiogenic shock | Occurs in ~10% of transmural MIs; typically when ≥40% of LV is damaged |
| Arrhythmias | ~90% of patients; most common cause of pre-hospital death; VF, heart block, SVTs, PVCs |
| Myocardial rupture | 1-3% of MIs; usually 3-7 days post-MI when granulation tissue is maximal; LV free wall (hemopericardium/tamponade), VSD (left-to-right shunt), papillary muscle rupture (severe MR) |
| Papillary muscle dysfunction/ischemia | Leads to mitral regurgitation |
| RV infarction | With RCA occlusion; right-sided heart failure, systemic hypotension |
| Pericarditis (Dressler syndrome) | Fibrinous pericarditis in the days following MI; autoimmune late pericarditis 2-10 weeks later |
| Mural thrombus | On the endocardial surface over the infarct; risk of systemic embolism |
| Ventricular aneurysm | Late complication; paradoxical systolic expansion of infarcted wall |
| Infarct extension / reinfarction | New area of necrosis adjacent to or distant from original infarct |
Causes of Death After Acute MI
- Decreased cardiac output (cardiogenic shock / systolic stretch of infarcted wall)
- Pulmonary edema (from LV failure damming blood in pulmonary vasculature)
- Ventricular fibrillation (most common cause of out-of-hospital MI death)
- Cardiac rupture (hemopericardium / tamponade)
One-third of patients who suffer STEMI at home die - usually from arrhythmia within the first hour before reaching medical care.
- Guyton & Hall, p. 271; Robbins, p. 518
Summary
MI is initiated by plaque rupture and coronary thrombosis, causes time-dependent irreversible myocyte necrosis (salvageable if reperfused within 20-40 minutes of occlusion), and evolves through predictable morphologic stages over weeks. Diagnosis rests on troponin kinetics and ECG. Management centers on rapid reperfusion (primary PCI), antiplatelets, anticoagulation, and beta-blockade. Complications span arrhythmias (most lethal in the early phase) to structural mechanical complications (rupture, aneurysm, MR) in the days to weeks after.
This is a shared conversation. Sign in to Orris to start your own chat.