Body fluids compartment
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Here is a complete, textbook-sourced overview of body fluid compartments.
Body Fluid Compartments
Overview
Total body water (TBW) is the starting point. In a standard 70-kg adult male, TBW is approximately 42 liters (60% of body weight). This varies with age, sex, and body composition:
- Newborns/premature infants: 70-75% of body weight
- Adult males: ~60%
- Adult females: ~50% (higher fat content, which contains little water)
- Elderly: progressively lower due to increased fat and decreased muscle mass
(Guyton and Hall Textbook of Medical Physiology)
The Two Major Compartments
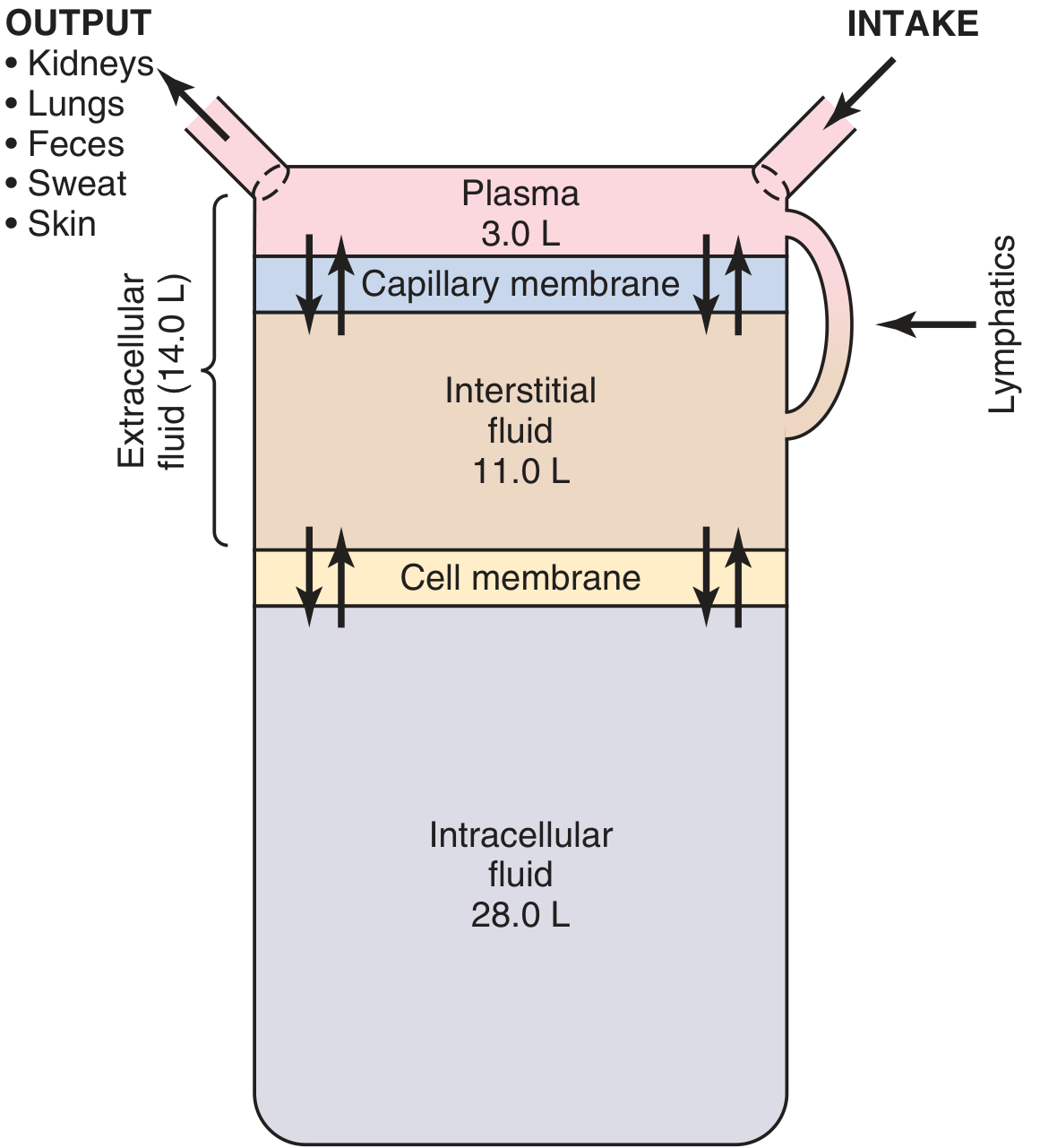
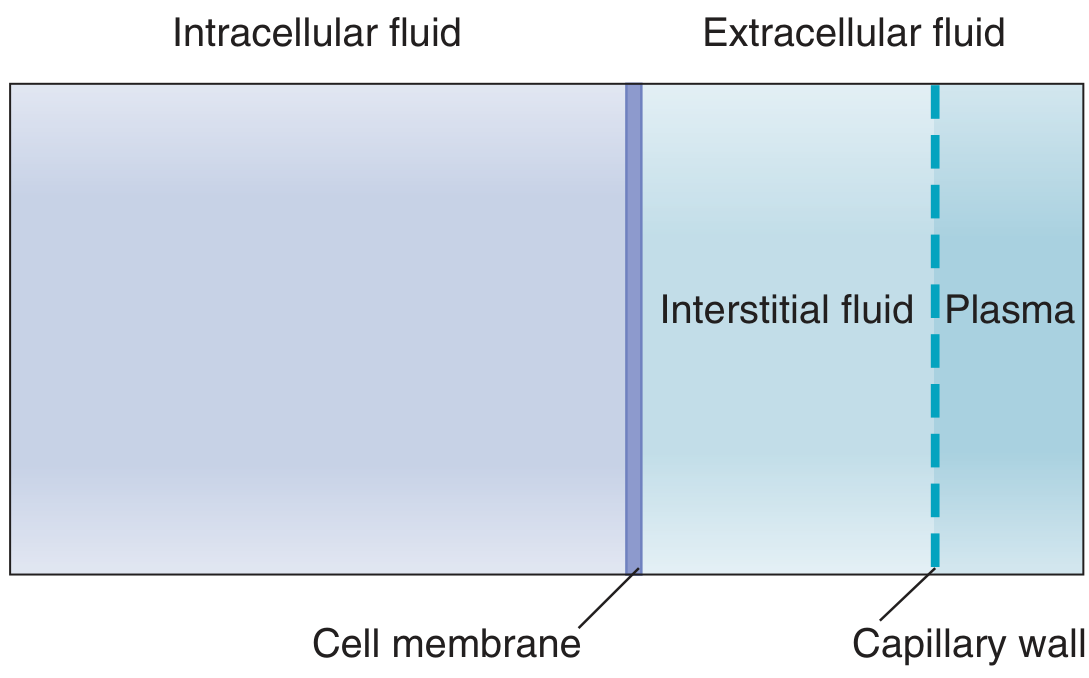
TBW is divided into two main compartments by the cell membrane:
| Compartment | Volume | % Body Weight | % TBW |
|---|---|---|---|
| Intracellular fluid (ICF) | 28 L | 40% | 2/3 |
| Extracellular fluid (ECF) | 14 L | 20% | 1/3 |
1. Intracellular Fluid (ICF)
All fluid inside the cells. Although each cell has its own individual composition, the concentrations of solutes are remarkably similar across different cell types - and even across different species. For this reason, ICF is treated as a single large compartment. - Guyton and Hall, p. 310
Key ICF solutes:
- Major cation: K⁺ (140 mEq/L) and Mg²⁺
- Major anions: Phosphate (PO₄³⁻), organic anions, and proteins
- Very low Na⁺ (14 mEq/L) and Cl⁻ (4 mEq/L)
- pH ~7.1 (more acidic than ECF)
2. Extracellular Fluid (ECF)
All fluids outside the cells. ECF is subdivided further:
| ECF Sub-compartment | Volume | Notes |
|---|---|---|
| Interstitial fluid | 11 L (>3/4 of ECF) | Bathes the cells directly; ultrafiltrate of plasma; very low protein |
| Plasma | 3 L (~1/4 of ECF) | Non-cellular blood component; separated from ISF by capillary wall |
| Transcellular fluid | 1-2 L | Synovial, peritoneal, pericardial, intraocular, CSF - a specialized ECF |
Plasma and interstitial fluid have nearly identical composition, except proteins - plasma contains significantly more protein, which cannot cross the capillary wall. - Guyton and Hall, p. 310
Key ECF solutes:
- Major cation: Na⁺ (142 mEq/L in plasma)
- Major anions: Cl⁻ (106 mEq/L) and HCO₃⁻ (24 mEq/L)
- pH 7.4
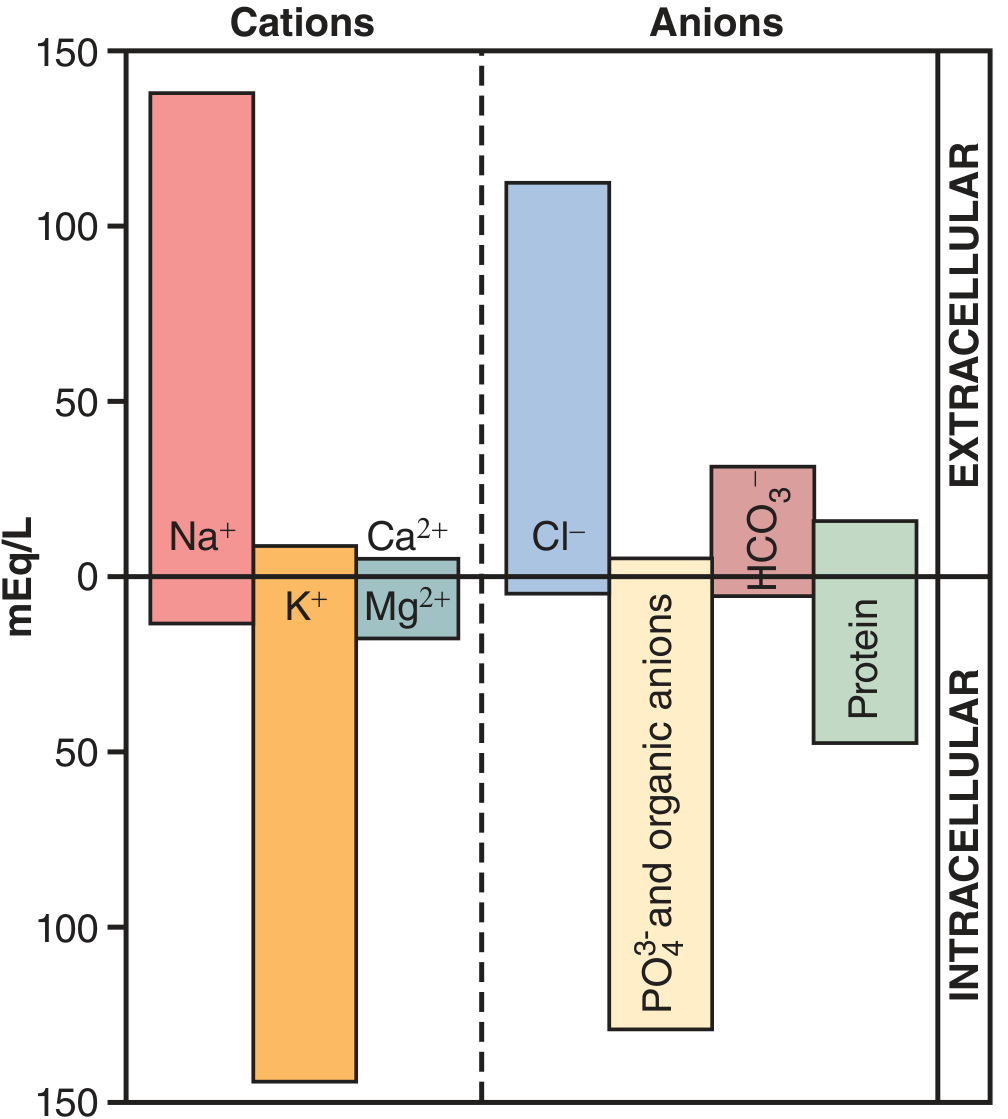
Composition Comparison: ECF vs ICF
| Substance | Plasma (mOsm/L) | Interstitial (mOsm/L) | Intracellular (mOsm/L) |
|---|---|---|---|
| Na⁺ | 142 | 139 | 14 |
| K⁺ | 4.2 | 4.0 | 140 |
| Ca²⁺ | 1.3 | 1.2 | 0.0001 |
| Mg²⁺ | 0.8 | 0.7 | 20 |
| Cl⁻ | 106 | 108 | 4 |
| HCO₃⁻ | 24 | 28.3 | 10 |
| Phosphate | 2 | 2 | 11 |
| Proteins | 16 | 0.2 | 4 |
| Total Osmolarity | ~290 | ~290 | ~290 |
(Guyton and Hall, Table 25.2)
The key principle: despite vastly different individual solute concentrations, total osmolarity is equal across all compartments (~290 mOsm/L). Water moves freely across cell membranes to maintain this equality. - Costanzo Physiology, 7th Ed.
Electroneutrality
Each compartment must obey macroscopic electroneutrality: the total concentration of cations (mEq/L) must equal the total concentration of anions. This holds even when a membrane potential exists, because only a tiny number of charges adjacent to the membrane are separated - not enough to change bulk concentrations. - Costanzo Physiology 7th Ed.
Blood Volume
Blood is a distinct compartment (contains both ECF and ICF elements):
- Total blood volume: ~5 liters (7% of body weight)
- ~60% plasma, ~40% red blood cells
- Normal hematocrit: ~0.42 in men, ~0.38 in women
Measuring Compartment Volumes - Dilution Method
The principle: a known amount of a marker is injected and allowed to equilibrate, then its concentration is measured. Volume = Amount injected / Equilibrated concentration.
| Compartment | % BW | Fraction of TBW | Marker Used |
|---|---|---|---|
| TBW | 60% | 1.0 | D₂O, tritiated water (THO), antipyrine |
| ECF | 20% | 1/3 | Mannitol, inulin, sulfate |
| ICF | 40% | 2/3 | Calculated: TBW - ECF |
| Plasma | 4% | 1/12 | Radioiodinated serum albumin (RISA), Evans blue |
| Interstitial fluid | 16% | 1/4 | Calculated: ECF - plasma |
Note: ICF and interstitial fluid volumes cannot be measured directly because no unique marker is confined to them. They are derived by subtraction. - Costanzo Physiology 7th Ed., p. 255
Key Principles of Fluid Shifts Between Compartments
- ECF volume is determined by its Na⁺ content - Na⁺ (with Cl⁻ and HCO₃⁻) is the dominant ECF solute; gain or loss of NaCl directly expands or contracts ECF.
- Osmolarity governs water distribution - estimated by:
Plasma Osm = 2 × [Na⁺] + Glucose/18 + BUN/2.8 - ICF and ECF osmolarity are always equal at steady state - any change in ECF osmolarity causes water to shift across cell membranes until equilibrium is restored.
- NaCl, NaHCO₃, and mannitol stay confined to ECF - they do not cross cell membranes, so they raise ECF osmolarity and draw water out of cells.
- Urea distributes across all compartments - it is an "ineffective osmole" because it crosses cell membranes freely and does not cause water shifts.
Sources: Guyton and Hall Textbook of Medical Physiology (25th chapter on body fluids); Costanzo Physiology 7th Edition (Chapters 1 and 6)
Action potential and phases
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive textbook content from Guyton & Hall and Braunwald's Heart Disease. Let me compile a complete, well-illustrated response.
Action Potential and Its Phases
An action potential (AP) is a rapid, transient reversal of membrane potential that propagates along excitable cell membranes (neurons, muscle). It obeys the all-or-nothing principle - once threshold is reached, the full AP fires regardless of stimulus strength. - Guyton and Hall, p. 84
Part I: Nerve Action Potential
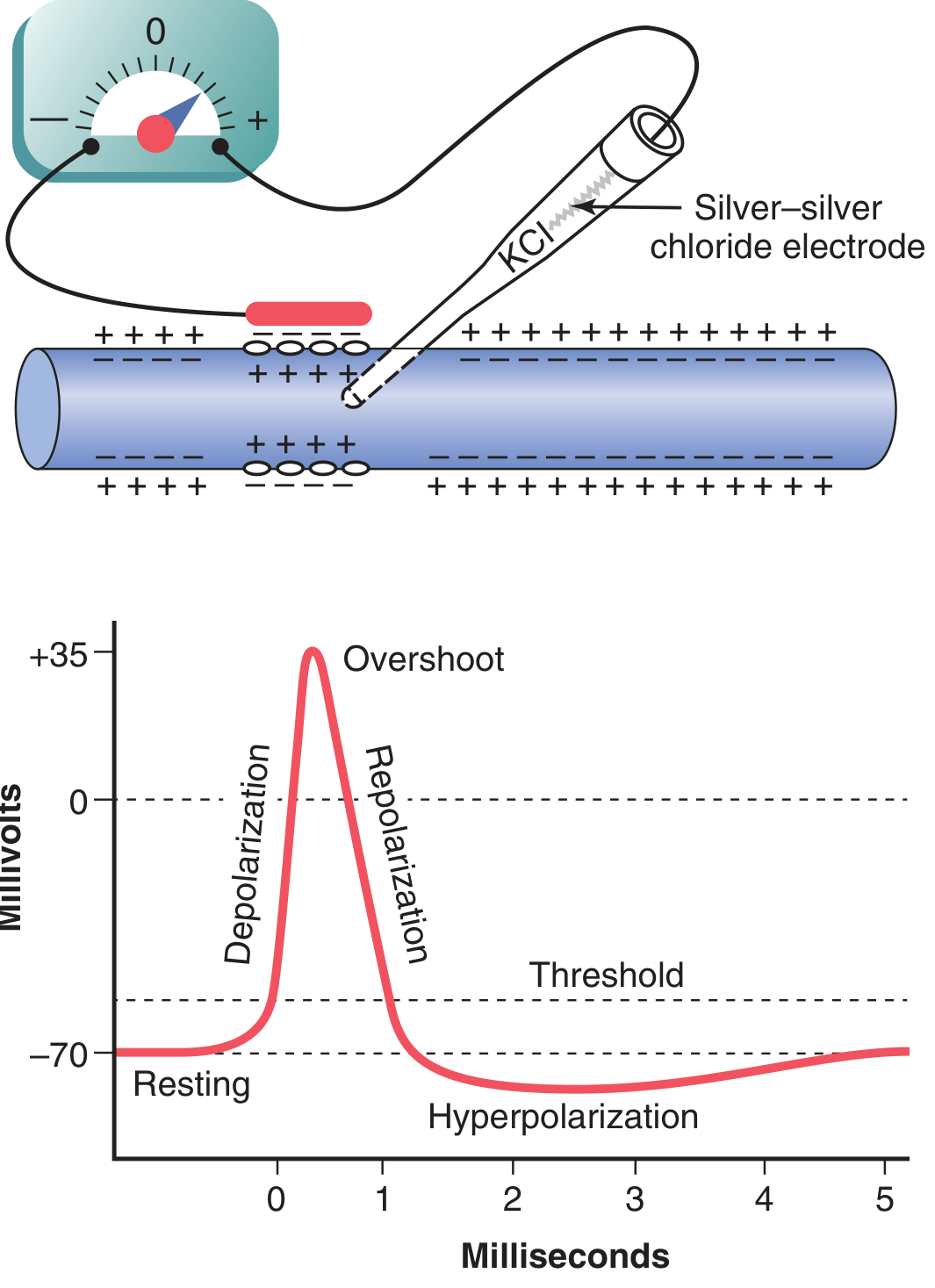
Phases of the Nerve AP
| Phase | Membrane Potential | Ion Movement | Mechanism |
|---|---|---|---|
| Resting | -70 mV | K⁺ leaks out | Na⁺-K⁺ pump maintains gradient; membrane is "polarized" |
| Depolarization | -70 → 0 mV | Na⁺ rushes IN | Threshold (~-55 mV) triggers voltage-gated Na⁺ channels to open |
| Overshoot | 0 → +35 mV | Na⁺ rushes IN | Massive inward Na⁺ current drives potential positive |
| Repolarization | +35 → -70 mV | K⁺ rushes OUT | Na⁺ channels inactivate; voltage-gated K⁺ channels open |
| After-hyperpolarization (undershoot) | Below -70 mV | K⁺ still exiting | K⁺ channels remain open slightly too long |
Voltage-Gated Na⁺ Channel - Three States
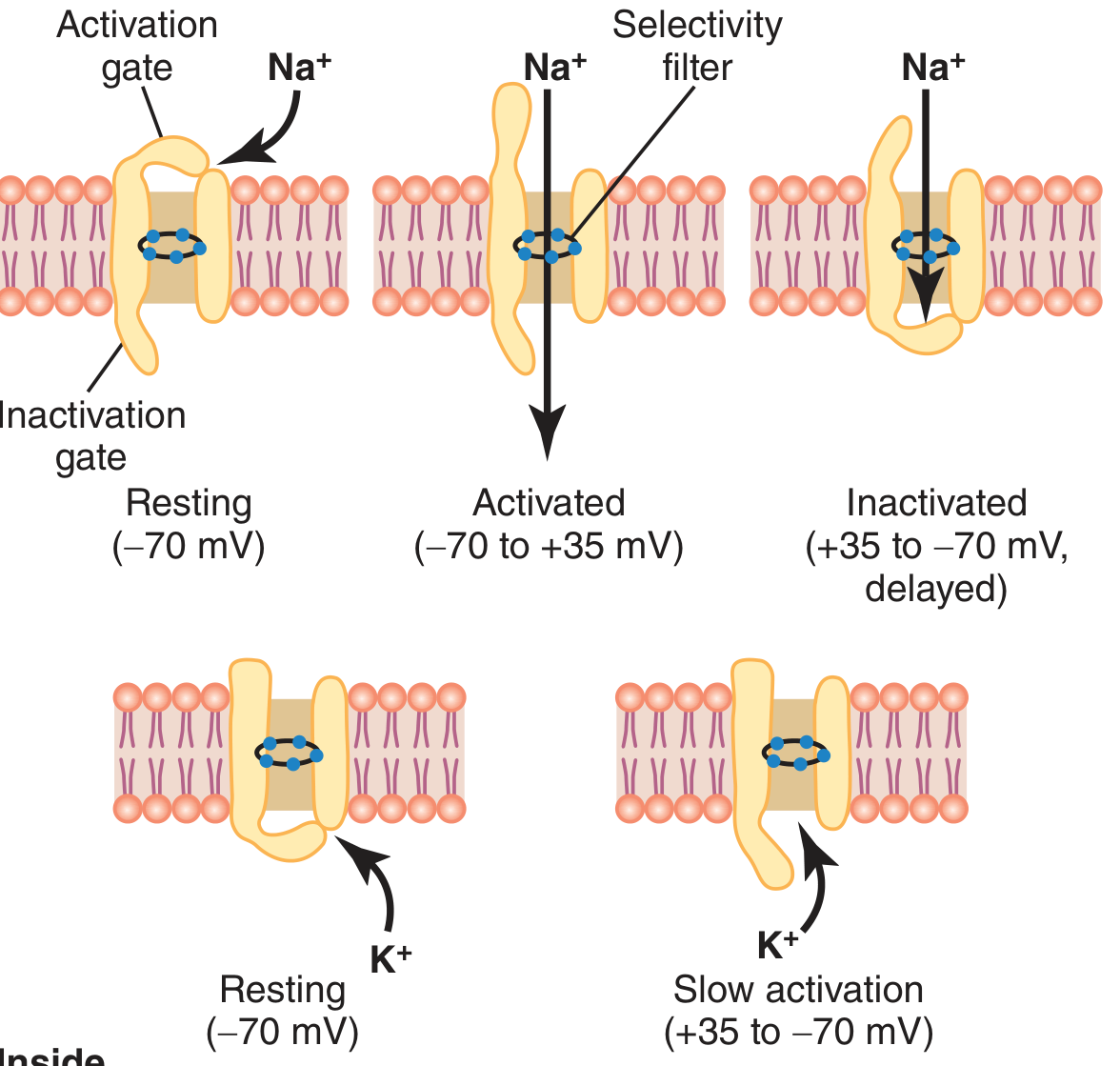
The Na⁺ channel has two gates - an outer activation gate and an inner inactivation gate:
- Resting state (-70 mV): Activation gate closed, inactivation gate open → channel closed
- Activated state (threshold to +35 mV): Activation gate snaps open within microseconds → massive Na⁺ influx (up to 5,000-fold increase in Na⁺ conductance)
- Inactivated state: The inactivation gate slowly closes (a few ten-thousandths of a second after activation) → Na⁺ entry stops; channel is refractory
The inactivation gate cannot reopen until the membrane repolarizes back near -70 mV. This is the basis of the refractory period. - Guyton and Hall, p. 81
The voltage-gated K⁺ channel opens more slowly (delayed) and has only one gate. It opens during repolarization and closes after membrane potential returns to rest.
Key Quantitative Points
- Resting potential: -70 mV
- Threshold potential: ~-55 mV (about 15 mV above resting)
- Peak overshoot: ~+35 mV
- Total AP duration: ~1-2 milliseconds in large nerve fibers
- At peak depolarization: Na⁺ conductance increases 500- to 5,000-fold; K⁺ conductance increases ~30-fold
Initiation - Positive Feedback Cycle
Depolarization → Na⁺ channels open → more Na⁺ in → more depolarization → more Na⁺ channels open. This self-sustaining positive feedback drives the explosive upstroke. The cycle terminates as Na⁺ channels inactivate and K⁺ channels open. - Guyton and Hall, p. 82
Refractory Periods
| Period | Mechanism | Clinical Significance |
|---|---|---|
| Absolute Refractory Period (ARP) | Na⁺ channels inactivated - cannot open again regardless of stimulus strength | No new AP is possible |
| Relative Refractory Period (RRP) | Some Na⁺ channels recovering; K⁺ channels still partially open; membrane hyperpolarized | A stronger-than-normal stimulus can fire a new AP |
Propagation
Local currents generated by the depolarized segment flow to adjacent resting membrane, raising it to threshold and triggering the AP there. The AP thus self-propagates in all directions. In myelinated fibers, conduction jumps between nodes of Ranvier (saltatory conduction), greatly increasing speed and metabolic efficiency. - Guyton and Hall, p. 84
Part II: Cardiac Action Potential
The cardiac AP differs fundamentally from the nerve AP - it is much longer (200-500 ms vs 1-2 ms) and has five numbered phases (0-4). Different cardiac cell types have distinct AP morphologies.
Five Phases of the Cardiac AP (Fast-Response: Ventricular Myocyte / His-Purkinje)
| Phase | Name | mV Range | Key Current(s) | Ion Movement |
|---|---|---|---|---|
| Phase 4 | Resting potential / Diastolic depolarization | -80 to -90 mV | I_(K1) (inward rectifier K⁺) | K⁺ out; maintains resting potential |
| Phase 0 | Upstroke / Rapid depolarization | -90 → +40 mV | I_Na (fast inward Na⁺) | Rapid Na⁺ in |
| Phase 1 | Early rapid repolarization | +40 → ~0 mV | I_to (transient outward K⁺) | K⁺ out (transiently) |
| Phase 2 | Plateau | ~0 mV sustained | I_CaL (L-type Ca²⁺ IN) vs I_K (K⁺ out) | Balance of Ca²⁺ in / K⁺ out |
| Phase 3 | Final rapid repolarization | 0 → -90 mV | I_Kr, I_Ks (delayed rectifier K⁺) | K⁺ out dominates; Ca²⁺ channels close |
(Braunwald's Heart Disease)
Phase Details
Phase 0 - Upstroke:
- Triggered when membrane depolarizes to threshold (~-65 to -70 mV in fast-response tissue)
- Fast Na⁺ channels (Nav1.5, encoded by SCN5A) open → explosive Na⁺ entry
- dV/dt_max (Vmax) in ventricular myocytes: 100-200 V/sec; in His-Purkinje: 500-700 V/sec
- Reaches ~+40 mV (near Na⁺ equilibrium potential of +60 mV)
- Conduction velocity correlates with Vmax: Purkinje fibers conduct fastest (2-3 m/sec)
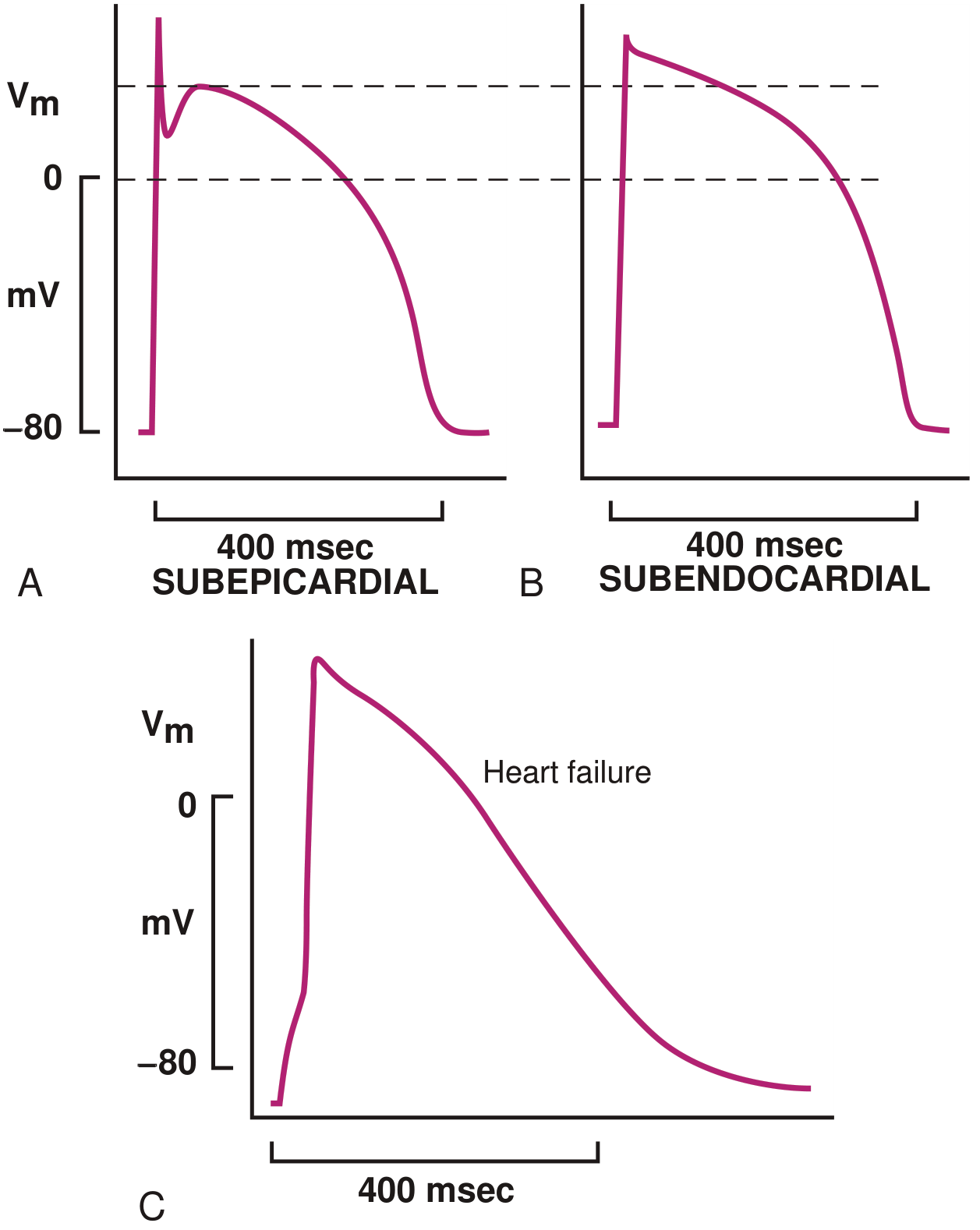
Phase 1 - Early notch:
- I_to (4-aminopyridine-sensitive transient outward K⁺ current) activates rapidly
- Creates a visible notch in epicardial cells (I_to density higher epicardially)
- Transmural gradient in I_to creates dispersion of repolarization - relevant in Brugada syndrome
Phase 2 - Plateau (unique to cardiac cells):
- The distinguishing feature of cardiac APs - absent in nerve APs
- L-type Ca²⁺ channels (slow channels) open and allow sustained Ca²⁺ entry
- This Ca²⁺ entry triggers Ca²⁺-induced Ca²⁺ release from the SR (excitation-contraction coupling)
- Prolonged plateau keeps the cardiac cell refractory (prevents tetany - crucial for pumping function)
- Duration: 200-300 ms in ventricular myocytes; 300-500 ms in His-Purkinje
Phase 3 - Final repolarization:
- Delayed rectifier K⁺ channels (I_Kr, I_Ks) provide increasing outward K⁺ current
- L-type Ca²⁺ current decays (inactivates)
- K⁺ efflux drives rapid return to resting potential
Phase 4 - Resting potential / Pacemaker potential:
- In non-pacemaker cells: stable at -80 to -90 mV; maintained by I_(K1)
- In SA/AV node pacemaker cells: spontaneous diastolic depolarization occurs - membrane gradually drifts toward threshold due to I_f ("funny current," HCN channels) + I_CaT, and NCX current
- This automatic depolarization generates the heart's intrinsic rhythm
Fast-Response vs Slow-Response Cardiac APs
| Feature | Fast-Response (Ventricle, His-Purkinje) | Slow-Response (SA node, AV node) |
|---|---|---|
| Resting potential | -80 to -95 mV | -50 to -70 mV |
| Phase 0 upstroke | Steep, rapid (I_Na) | Slow, gradual (I_CaL) |
| Vmax | 100-700 V/sec | 1-15 V/sec |
| Overshoot | +30 mV | 0-15 mV |
| Conduction velocity | 0.3-3 m/sec | <0.05-0.1 m/sec |
| Automaticity | No (non-pacemaker) | Yes |
| AP duration | 200-500 ms | 100-300 ms |
(Braunwald's Heart Disease, Table 62.2)
Properties of Cardiac Na⁺-K⁺ ATPase
The Na⁺-K⁺ pump is electrogenic (pumps 3 Na⁺ out for 2 K⁺ in), contributing a small net negative charge to the resting potential. As heart rate increases, pump rate increases to restore ionic gradients depleted by each depolarization. Inhibition by digitalis toxicity can depolarize cardiac cells and cause arrhythmias. - Braunwald's Heart Disease, p. 393
Sources: Guyton and Hall Textbook of Medical Physiology (Chapter 5); Braunwald's Heart Disease, 2-Vol Set (Chapter 62 - Cardiac Electrophysiology)
Blood transfusion and complications
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
I now have comprehensive coverage from Harrison's Principles of Internal Medicine 22E (2025) and Bailey & Love's Surgery. Here is the full response:
Blood Transfusion and Complications
Blood Products Overview
| Product | Content | Storage | Indication |
|---|---|---|---|
| Red Blood Cell Concentrate (RBCC) | Packed RBCs, ~200-250 mg Fe | 2-4°C, 21-35 days | Anemia, hemorrhage (Hb trigger typically <7-8 g/dL) |
| Platelet Concentrate (PC) | Platelets | Room temp, ≤5 days | Thrombocytopenia, platelet dysfunction |
| Fresh Frozen Plasma (FFP) | All coagulation factors | -18°C, 12 months | Coagulopathy, factor deficiency |
| Cryoprecipitate | Fibrinogen, Factor VIII, vWF | -18°C, 12 months | Hypofibrinogenemia, hemophilia A, vWD |
| Granulocyte concentrate | Granulocytes | Room temp, ≤24 h | Severe neutropenia with infection |
| Whole blood | All components | 2-4°C, 21-35 days | Massive hemorrhage (damage control) |
(Harrison's Principles of Internal Medicine, 22E)
Pre-Transfusion Testing
Before any transfusion:
- ABO and D (Rh) phenotyping - also includes CcEe, Kell (K), Duffy, Kidd, MNS antigens depending on clinical context
- Antibody screen - patient serum mixed with type-O RBCs to detect alloantibodies
- Crossmatch - recipient plasma vs selected donor RBCs (essential in alloimmunized patients, sickle cell disease, frequent transfusion recipients)
- Patient identity verification - double ABO determination where possible
Note: Anti-CD38 monoclonal antibody therapy (e.g., daratumumab for myeloma) can interfere with antibody screening by binding to erythrocytes. Dithiothreitol (DTT) pretreatment can offset this. - Harrison's 22E
Complications
Complications are classified as immunologic and non-immunologic, and further as related to single transfusion or massive transfusion.
A. Immunologic Complications
1. Acute Hemolytic Transfusion Reaction (AHTR)
Mechanism: Preformed recipient antibodies (most often anti-A or anti-B IgM) lyse transfused donor RBCs. Anti-A/B IgM fixes complement up to C5/C9, forming membrane attack complex (MAC) → intravascular hemolysis.
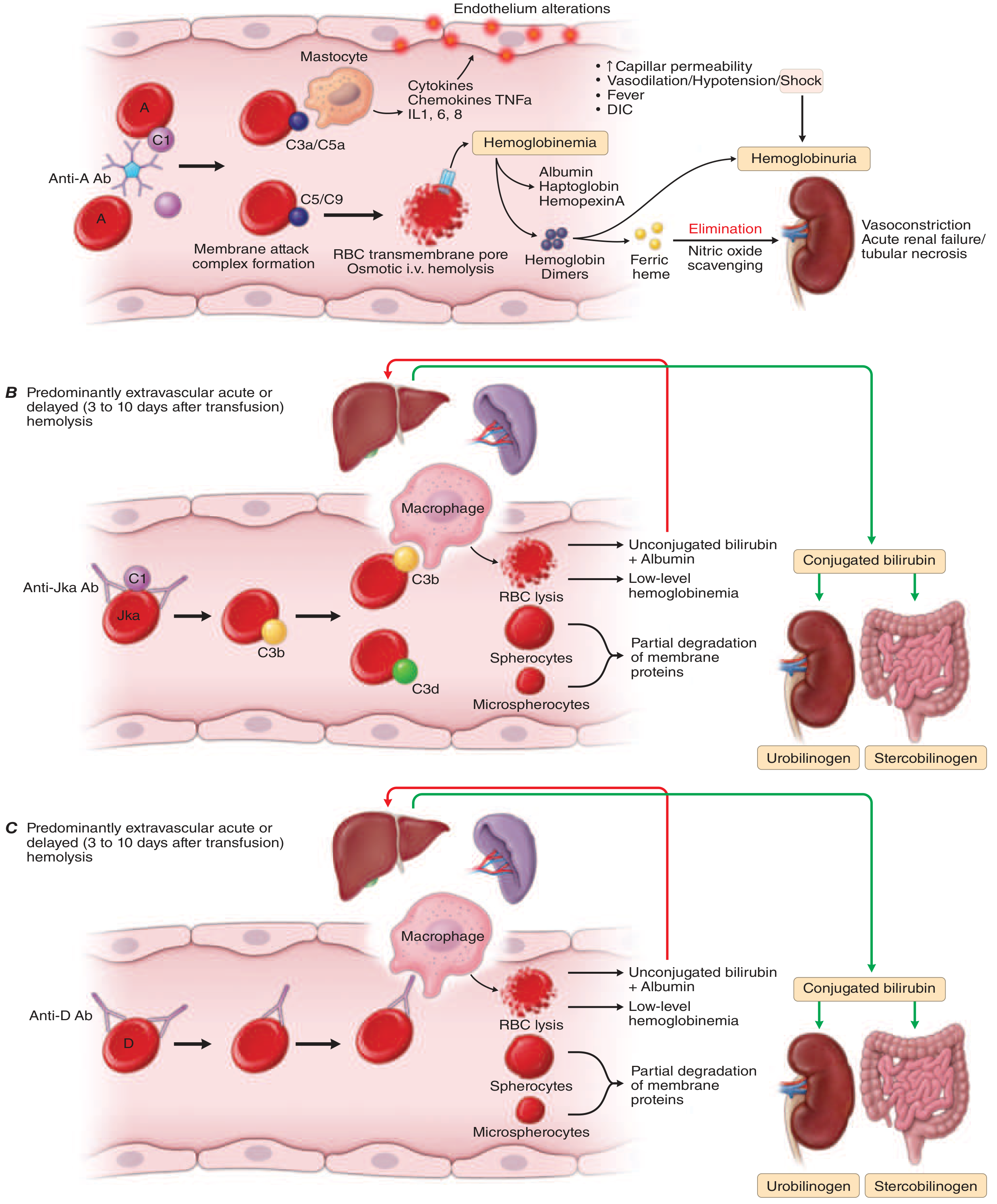
Causes: ABO incompatibility, errors in patient/product identification, unidentified alloimmunization.
Clinical features:
- Fever (≥1-2°C rise), chills, rigors
- Hypotension, tachycardia, tachypnea
- Chest and back pain
- Hemoglobinuria (pink/red urine), hemoglobinemia
- In severe cases: DIC, acute renal failure, shock, death
Frequency: 1-10 per 10⁵ transfused units
Diagnosis: Persisting/worsening anemia, depleted plasma haptoglobin, elevated LDH, unconjugated bilirubin, free plasma hemoglobin; positive direct antiglobulin test (DAT/Coombs)
Management:
- STOP the transfusion immediately
- Maintain IV access and blood pressure
- IV fluids + furosemide to maintain urine output and protect kidneys
- Monitor for DIC; treat accordingly
- Send blood/urine samples for investigation
2. Delayed Hemolytic Transfusion Reaction (DHTR)
Mechanism: Anamnestic (secondary) immune response in previously sensitized patients. AlloAbs (typically IgG against Rh, Kell, Duffy, Kidd) were below detectable levels at pretransfusion testing but rise 1-2 weeks post-transfusion. Complement activation stops at C3 → C3b opsonization → extravascular hemolysis (macrophage clearance in spleen/liver).
Clinical features: Icterus (jaundice), persisting or worsening anemia developing 3-10 days post-transfusion; spherocytes on smear.
Frequency: 5-40 per 10⁵ transfused units
Special concern - Hyperhemolytic syndrome: In sickle cell patients on long-term transfusion, hemolysis extends to the patient's own RBCs. Hb can fall below pre-transfusion values; further transfusion may worsen the reaction.
3. Febrile Non-Hemolytic Transfusion Reaction (FNHTR)
The most frequent cellular transfusion reaction (~300 per 10⁵ units).
Mechanism: Two mechanisms:
- Pro-inflammatory cytokines released by leukocytes during storage accumulate in the blood component
- Recipient antibodies directed against donor leukocyte antigens
Clinical features: Chills, rigors, and a ≥1°C rise in body temperature (usually within 1-2 h of starting transfusion)
Diagnosis of exclusion - must rule out hemolysis and infection first.
Prevention: Prestorage leukocyte reduction (most effective); use of additive solutions in PCs.
Management: Slow/pause transfusion; antipyretics (though evidence for prevention is poor); monitor closely.
4. Allergic Reactions
Frequency:
- Mild: ~100 per 10⁵ units
- Severe anaphylaxis: ~5 per 10⁵ units
Mechanism: Plasma proteins in transfused components trigger histamine/serotonin release from platelets and leukocytes. Most reactions are not antibody-mediated.
Special risk - IgA deficiency (~1/700 people): IgA-deficient patients who have developed anti-IgA antibodies can develop severe anaphylaxis from even small volumes of plasma. They require IgA-deficient plasma and washed cellular components.
Clinical features:
| Mild | Severe (Anaphylaxis) |
|---|---|
| Rash, pruritus, urticaria | Bronchospasm, stridor |
| Localized edema | Hypotension, shock |
| Nausea, vomiting |
Management:
- Mild: Stop transfusion, antihistamine; restart if symptoms resolve
- Anaphylaxis: Stop immediately; epinephrine 0.3-0.5 mg SC; steroids, antihistamines, bronchodilators, IV fluids
5. Transfusion-Related Acute Lung Injury (TRALI)
Definition: New or worsening hypoxia + bilateral interstitial infiltrates on CXR, occurring during or within 6 hours of transfusion (delayed cases up to 72 h). Non-cardiogenic pulmonary edema. One of the leading causes of transfusion-related fatalities.
Frequency: 0.5-10 per 10⁵ units (BC-dependent)
Mechanism:
- Donor plasma contains anti-HLA class II (most common) or anti-HLA class I or anti-HNA antibodies
- These antibodies bind recipient cognate antigen on pulmonary endothelium and primed leukocytes
- Leukocytes aggregate in pulmonary vasculature → release inflammatory mediators → capillary leak → pulmonary edema
- Cytokine/chemokine-mediated TRALI (without HLA antibodies) also occurs
Risk factors in recipient: Smoking, chronic alcohol use, shock, liver surgery, cancer surgery, mechanical ventilation, positive fluid balance.
Prevention: Transfusing plasma/PCs from male donors and nulliparous women without anti-HLA antibodies has significantly reduced TRALI risk.
TRALI vs TACO distinction:
| Feature | TRALI | TACO |
|---|---|---|
| Mechanism | Lung inflammation | Fluid overload |
| Blood pressure | Hypotension | Hypertension |
| BNP | Normal or mildly elevated | Markedly elevated |
| Response to diuretics | Poor | Good |
| Onset | Within 6 h | During or shortly after |
Management: Supportive only - oxygen, mechanical ventilation if needed; diuretics are NOT indicated (unlike TACO).
6. Transfusion-Associated Circulatory Overload (TACO)
Currently the leading cause of transfusion-related death (TRALI risk has been mitigated by donor selection).
Frequency: ~10-100 per 10⁵ units
Mechanism: Excess volume administered faster than the cardiovascular system can accommodate.
Risk factors: Older age, renal failure, cardiac dysfunction, preexisting fluid overload, large volume or rapid transfusion rate.
Features: Dyspnea, hypoxia, bilateral pulmonary edema (predominantly alveolar pattern), systolic hypertension (distinguishes from TRALI), elevated BNP, fever.
Prevention: Identify at-risk patients; transfuse at ≤1 unit per 3-4 hours; use diuretics in stable patients.
Management: Stop transfusion; oxygen; diuretics.
7. Transfusion-Associated Graft-versus-Host Disease (TA-GvHD)
Rare but often fatal. Caused by engrafted donor T lymphocytes that cannot be rejected by a severely immunosuppressed recipient (e.g., BMT patients, congenital immunodeficiencies, HLA-homozygous patients receiving blood from HLA-compatible donors).
Features (5-10 days post-transfusion): Fever, characteristic skin rash, diarrhea, liver dysfunction, pancytopenia (distinguishes from transplant-associated GVHD where marrow is spared).
Prevention: Gamma irradiation of cellular blood components for at-risk patients (mandatory). Pathogen-reduction technologies that cross-link nucleic acids may also prevent TA-GvHD.
8. Post-Transfusion Purpura (PTP)
Rare (~1/10⁵). Thrombocytopenia and bleeding 5-12 days after PC (or RBCC) transfusion, predominantly in women. Caused by platelet-specific alloantibodies (most often anti-HPA-1a). Managed with IVIG, steroids, or plasma exchange.
B. Non-Immunologic Complications
9. Infectious Transmission
| Pathogen | Risk per 10⁶ products | Prevention |
|---|---|---|
| HIV-1/2 | ~0.1/10⁶ donations; 0.1-1 infection/10⁶ | Serology + NAT |
| HBV | ~0.5/10⁶ donations; <0.5/10⁶ | Serology + NAT |
| HCV | 0.2-1/10⁶ donations | NAT testing |
| Bacterial (PC) | 10-20/10⁶ donations; 5-30 sepsis/10⁶ | Bacterial detection, pathogen reduction |
| Yersinia (RBCC) | Grows at 4°C | Serology, culture |
| Treponema pallidum | ~1/10⁶ donations | Serology |
| West Nile virus, Babesia | Emerging risks | NAT + surveillance |
Window period - the period early after infection when pathogen titers are too low for detection - remains the main residual risk despite improved NAT testing. - Harrison's 22E, Table 118-5
Bacterial contamination of PCs (room-temp storage) remains the most frequent infectious risk. Features: abrupt fever and chills during transfusion → septic shock, DIC. Management: broad-spectrum antibiotics after cultures.
10. Iron Overload (Chronic Transfusion)
Each RBCC contains 200-250 mg of elemental iron. In chronically transfused patients (thalassemia, sickle cell, myelodysplasia), iron accumulates because there is no physiologic excretion mechanism.
End-organ damage: Cardiac failure/arrhythmia, hepatic fibrosis/cirrhosis, endocrine dysfunction (diabetes, hypogonadism).
Assessment: Serum ferritin, MRI liver, liver biopsy.
Treatment: Iron chelation (deferoxamine, deferasirox, deferiprone).
C. Massive Transfusion Complications
Definition: Transfusion of ≥50% of total blood volume over 3 hours, or >5-10 units of RBCCs.
| Complication | Mechanism | Management |
|---|---|---|
| Dilutional coagulopathy | Loss of clotting factors + dilution with RBCs | FFP + platelets in 1:1:1 ratio with RBCs; tranexamic acid (antifibrinolytic) |
| Hypocalcemia | Citrate anticoagulant chelates ionized Ca²⁺; circumoral paresthesia, cardiac effects | IV calcium gluconate (separate line) |
| Hyperkalemia | K⁺ leaks from stored/irradiated RBCs; risk in neonates and renal failure | Insulin + glucose, calcium gluconate, furosemide; use washed or fresh RBCCs |
| Hypothermia | Transfusing 4°C blood | Inline blood warmer |
| Metabolic alkalosis | Citrate metabolized to bicarbonate | Usually self-limited |
Massive Transfusion Protocol (MTP): For severely injured/hemorrhaging patients, blood bank provides a cooler with low-titer O whole blood (LTOWB) or type-O RBCs + AB/A plasma. Subsequent coolers deliver RBCs : FFP : platelets in 1:1:1 ratio. O-negative blood is reserved for females of childbearing age when type is unknown. Lactated Ringer's solution should be avoided with transfusion (calcium binds citrate). - Sabiston Textbook of Surgery
Hypofibrinogenemia (common in massive hemorrhage): Treat empirically with cryoprecipitate (contains fibrinogen, Factor VIII, vWF), guided by point-of-care thromboelastometry. Most bleeding patients are hyperfibrinolytic - give tranexamic acid as early as possible. - Bailey & Love's Surgery
Quick Reference: Reaction Summary
| Reaction | Timing | Key Feature | Action |
|---|---|---|---|
| Acute hemolytic (AHTR) | During / <24 h | Hemoglobinuria, DIC, renal failure | Stop; fluids; monitor kidneys |
| Febrile non-hemolytic (FNHTR) | 1-6 h | Fever, chills only | Slow/pause; antipyretics |
| Allergic (urticaria) | Minutes to 2 h | Urticaria, rash | Antihistamine; can restart |
| Anaphylaxis | Minutes | Shock, bronchospasm | Stop; epinephrine |
| TRALI | <6 h | Pulmonary edema + hypotension | Stop; supportive |
| TACO | During or shortly after | Pulmonary edema + hypertension | Stop; diuretics |
| Delayed hemolytic (DHTR) | 3-10 days | Worsening anemia, jaundice | Supportive; monitor |
| TA-GvHD | 5-10 days | Rash, diarrhea, pancytopenia | Prevent with irradiation |
| Post-transfusion purpura | 5-12 days | Thrombocytopenia | IVIG, steroids |
| Sepsis (bacterial) | During / shortly after | High fever, rapid deterioration | Stop; blood cultures; antibiotics |
Sources: Harrison's Principles of Internal Medicine 22E (2025), Chapter 118; Bailey and Love's Short Practice of Surgery 28th Ed.; Sabiston Textbook of Surgery; Harrison's Table 118-5.
Blood transfusion and complications
I just covered this topic in detail in my previous response. Here's a concise summary of everything included:
Blood Transfusion & Complications - Summary
Blood Products
| Product | Key Use | Storage |
|---|---|---|
| RBCC (packed RBCs) | Anemia, hemorrhage | 2-4°C, 21-35 days |
| Platelets | Thrombocytopenia | Room temp, ≤5 days |
| FFP | Coagulopathy | -18°C, 12 months |
| Cryoprecipitate | Low fibrinogen, hemophilia A | -18°C, 12 months |
Pre-transfusion Testing
- ABO + D (Rh) phenotyping
- Antibody screen
- Crossmatch (for alloimmunized/frequently transfused patients)
- Patient identity verification
Complications - Quick Reference
Immunologic
| Reaction | Timing | Key Feature | Management |
|---|---|---|---|
| Acute hemolytic (AHTR) | During / <24 h | Hemoglobinuria, DIC, renal failure | Stop transfusion; IV fluids; monitor kidneys |
| Delayed hemolytic (DHTR) | 3-10 days | Worsening anemia, jaundice | Supportive; monitor |
| Febrile non-hemolytic (FNHTR) | 1-6 h | Fever + chills only (most common reaction) | Slow/pause; antipyretics |
| Allergic (mild) | Minutes-2 h | Urticaria, pruritus | Antihistamine; can restart |
| Anaphylaxis | Minutes | Bronchospasm, shock | Stop; epinephrine 0.3-0.5 mg SC |
| TRALI | <6 h | Non-cardiogenic pulmonary edema + hypotension | Stop; supportive only (no diuretics) |
| TACO | During/after | Pulmonary edema + hypertension, elevated BNP | Stop; O₂; diuretics |
| TA-GvHD | 5-10 days | Rash, diarrhea, pancytopenia | Prevent with irradiation of products |
| Post-transfusion purpura | 5-12 days | Thrombocytopenia (anti-HPA-1a) | IVIG, steroids |
TRALI vs TACO: TRALI = hypotension + normal BNP; TACO = hypertension + elevated BNP. TACO is now the #1 cause of transfusion fatality.
Non-Immunologic
- Infectious: HIV, HBV, HCV (very low risk with NAT testing); bacterial contamination of platelets is the most common infectious risk
- Iron overload: 200-250 mg Fe per unit; treat with chelation (deferasirox, deferoxamine) in chronically transfused patients (thalassemia, SCD)
Massive Transfusion Complications (>50% blood volume in 3 h)
| Complication | Cause | Treatment |
|---|---|---|
| Dilutional coagulopathy | Loss + dilution of clotting factors | 1:1:1 ratio (RBC:FFP:platelets); tranexamic acid |
| Hypocalcemia | Citrate chelates Ca²⁺ | IV calcium gluconate |
| Hyperkalemia | K⁺ leaks from stored RBCs | Insulin/glucose, calcium, furosemide |
| Hypothermia | Cold blood (4°C) | Inline blood warmer |
| Hypofibrinogenemia | Consumption + dilution | Cryoprecipitate |
Massive Transfusion Protocol (MTP): Low-titer O whole blood (LTOWB) or RBC:FFP:Platelets in 1:1:1 ratio. O-negative reserved for females of childbearing age with unknown type. Tranexamic acid given early (most patients are hyperfibrinolytic).
Please let me know if you'd like me to go deeper on any specific aspect - mechanisms, a particular reaction, management protocols, or blood group serology.
This is a shared conversation. Sign in to Orris to start your own chat.