External Abdominal Hernias: (Classification of hernias. General symptoms of hernias. Diagnosis. Types of hernia repair. Features of patient preparation for surgery and postoperative management. Complications of hernias. Strangulated hernia).
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Now I have all necessary content to provide a comprehensive, well-structured answer.
External Abdominal Hernias
1. Classification of Hernias
By Location (Type)
| Hernia | Anatomical Site | Key Features |
|---|---|---|
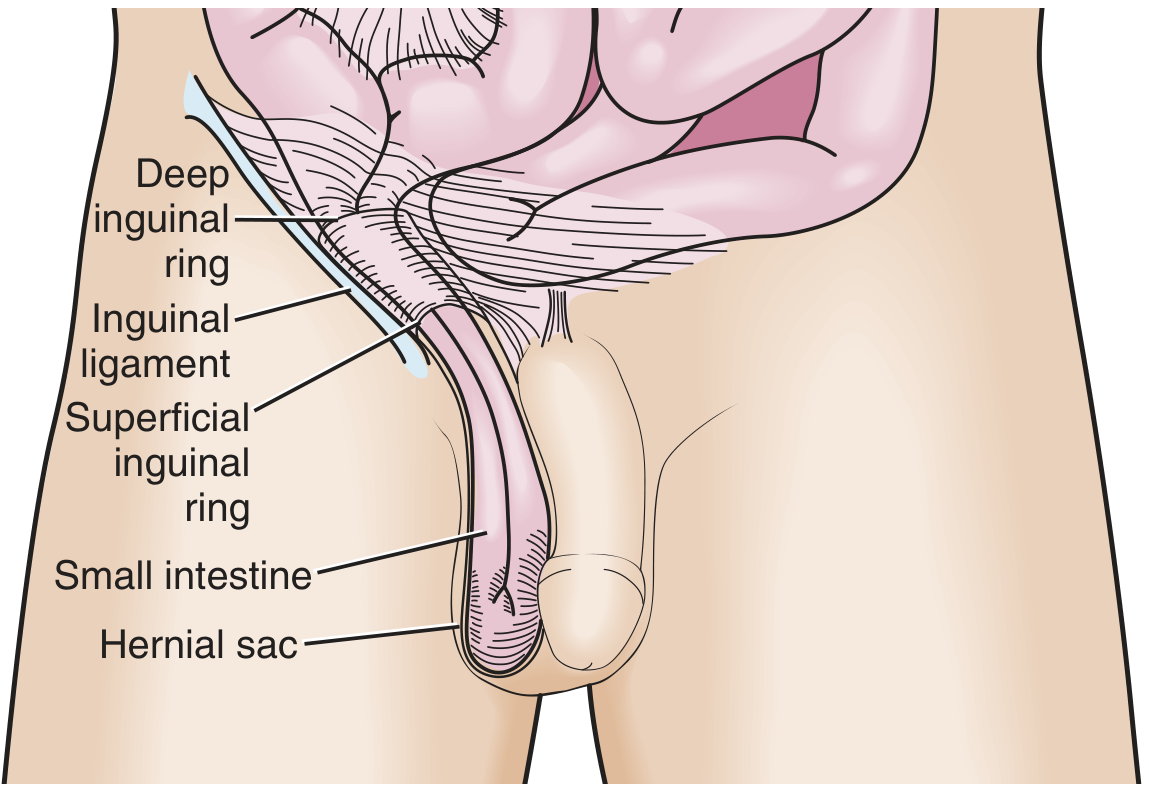
| Indirect Inguinal | Through deep inguinal ring → inguinal canal | Lateral to inferior epigastric vessels; most common hernia overall; more common in males |
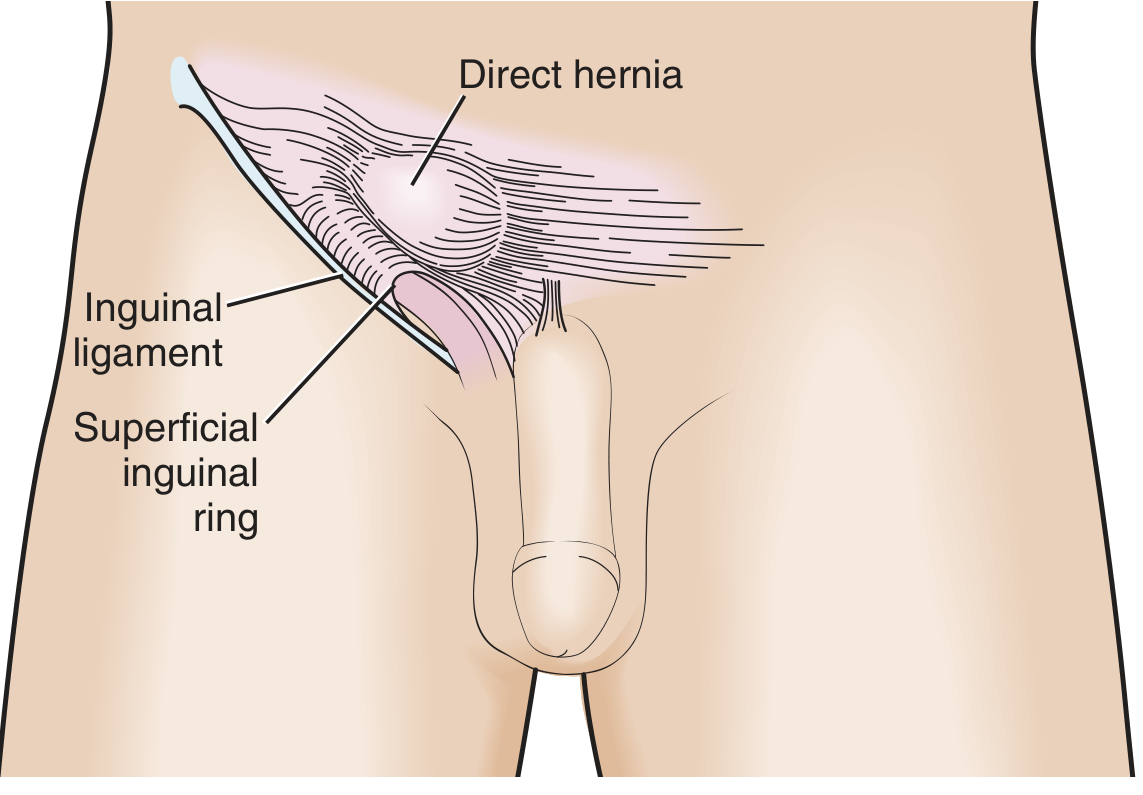
| Direct Inguinal | Through posterior wall of inguinal canal (Hesselbach's triangle) | Medial to inferior epigastric vessels; acquired, due to fascial weakening; lower incarceration risk (wide neck) |
| Pantaloon | Combination of direct + indirect | Difficult to reduce manually; usually found at surgery |
| Femoral | Below inguinal ligament, medial to femoral vein in femoral canal | More common in women; high incarceration risk (~45%) due to narrow ring |
| Umbilical | Through umbilical fibromuscular ring | Common in infants (congenital, often self-resolves by age 5); acquired in adults with raised intra-abdominal pressure |
| Epigastric | Through linea alba, between xiphoid and umbilicus | Usually small; contain preperitoneal fat in adults |
| Incisional | Through previous surgical wound | Complicates ~10–20% of laparotomies (up to 69% in high-risk groups) |
| Spigelian | Through defect at lateral rectus edge at semilunar/arcuate line | Rare; incarceration up to 20%; ultrasound helpful |
| Lumbar / Obturator / Paraduodenal | Various posterior/internal sites | Often diagnosed at laparotomy |
By Reducibility / Clinical Status
- Reducible: Contents return spontaneously or with gentle pressure
- Irreducible (Incarcerated): Contents cannot be reduced; not yet ischemic
- Strangulated: Blood supply compromised → ischemia/necrosis; surgical emergency
- Richter hernia: Only a portion of the bowel wall (antimesenteric) is incarcerated — strangulation can occur without complete bowel obstruction
By Aetiology
- Congenital (e.g., failure of processus vaginalis to close → indirect inguinal)
- Acquired (e.g., direct inguinal from fascial weakening with age; incisional after poor wound healing)
2. General Symptoms
A patient with a symptomatic hernia typically presents with:
- Visible/palpable bulge at the hernia site — often the primary complaint
- Aching or dragging discomfort, worsened by prolonged standing, straining, coughing, or exertion
- Impulse on coughing — bulge increases with Valsalva
- Reducibility — bulge disappears on lying down in uncomplicated hernias
- Bowel obstruction symptoms (if incarcerated) — colicky abdominal pain, nausea, vomiting, distension, absolute constipation
- Acute severe pain (if strangulated) — constant, unrelenting pain at the hernia site, systemic signs of sepsis
A crucial clinical point: femoral and obturator hernias may cause bowel obstruction without an obvious groin mass — careful groin examination is mandatory in any patient presenting with obstruction. — Mulholland and Greenfield's Surgery, p. 2429
3. Diagnosis
History and Physical Examination
- Elicit onset, duration, reducibility, and any episodes of acute pain or obstruction
- Examine the patient standing and supine; ask patient to cough or strain
- Assess reducibility, tenderness, and bowel sounds over the hernia
- Auscultation over the sac — bowel sounds confirm intestinal content
Imaging
- CT scan is the gold standard for complex, internal, or uncertain hernias (e.g., CT pelvis/abdomen with axial and coronal views to identify herniating segment and hernia orifice — see Figure 49.6 in Mulholland)
- Ultrasound is useful for Spigelian hernias and equivocal groin swellings; also used to guide reduction
- Plain radiograph: may show air-filled bowel loops in hernia sac in obstruction
4. Types of Hernia Repair
Tension-Based (Tissue) Repairs
- Shouldice repair: Multi-layer imbrication of the posterior inguinal wall; recurrence < 1% at the Shouldice Clinic (though not reproducible universally)
- Bassini repair: Classic primary tissue repair, now largely superseded
- Preferred in contaminated fields (strangulated hernia with bowel resection) to avoid mesh infection
Tension-Free Repairs (Preferred for Elective Cases)
- Lichtenstein (open anterior mesh): Polypropylene mesh placed over posterior inguinal wall; recurrence ≤ 2% at specialist centres; the standard tension-free repair
- Plug and patch: Mesh plug placed in internal ring + flat mesh overlay
- Preperitoneal mesh: Mesh placed posterior to transversalis fascia
Laparoscopic Repairs
- TAPP (Transabdominal PrePeritoneal): Mesh placed via laparoscope through the peritoneal cavity into the preperitoneal space
- TEP (Totally Extraperitoneal): Mesh placed entirely in the preperitoneal space without entering the peritoneal cavity — avoids intraperitoneal organ injury
- eTEP (Enhanced-View TEP): Extended dissection plane allowing larger mesh placement
- Robotic-assisted: Increasing adoption for both TAPP and TEP; equivalent outcomes to laparoscopic in experienced hands
- Laparoscopic approaches are associated with lower short- and long-term risks for intestinal obstruction and faster recovery
Ventral/Incisional Hernia Repair
- Onlay mesh: Mesh placed superficial to the anterior fascial repair
- Sublay (retromuscular/component separation): Mesh placed posterior to rectus muscles in the retromuscular plane — lower recurrence and infection rates
- Intraperitoneal onlay mesh (IPOM): Mesh placed intraperitoneally with anti-adhesion coating; laparoscopic or robotic
Mesh significantly reduces recurrence vs. primary tissue repair. Contamination (bowel resection, enterotomy) increases wound infection, fistula, reoperation, and mortality risk with synthetic mesh — clinical judgment and surgeon experience guide mesh vs. tissue repair in emergency settings. — Mulholland and Greenfield's Surgery, pp. 2431–2432
5. Patient Preparation for Surgery and Postoperative Management
Preoperative Preparation
- Optimise comorbidities: Correct electrolyte and metabolic disturbances; optimise glycaemic control; treat pulmonary disease (smoking cessation reduces risk of pulmonary and wound complications)
- Nutritional optimisation: Address hypoalbuminaemia; carbohydrate loading as part of ERAS protocols reduces postoperative ileus
- Weight reduction for morbidly obese patients reduces hernia recurrence and wound complications
- Bowel preparation: Not routinely required for elective inguinal hernia; may be indicated for ventral/incisional hernia repair where bowel injury risk is significant
- Antibiotics: Single dose prophylaxis for mesh repair
- Fluid resuscitation: Essential in emergency/strangulated cases — IV fluids, correct fluid/electrolyte deficits; nasogastric decompression if obstructed
Anesthetic Considerations
- Elective inguinal hernia repair is commonly performed under local anaesthesia + sedation, regional (spinal), or general anaesthesia
- Local anaesthesia preferred in high-risk patients to minimize urinary retention risk
- Spinal anaesthesia is associated with comparable outcomes; general anaesthesia used for laparoscopic cases
Postoperative Management (ERAS)
- Early mobilisation: Encouraged from day of surgery; reduces ileus and pulmonary complications
- Early oral feeding: Stimulates propulsive bowel motility and immune function; reduces anastomotic dehiscence risk
- Pain management: Multimodal analgesia (NSAIDs + paracetamol ± local nerve block); minimise opioids to reduce ileus and urinary retention
- Fluid management: Avoid perioperative fluid overload; standardise perioperative fluid protocols
- Urinary catheter: Not routinely required; remove early to facilitate mobilisation
- Wound care: Monitor for seroma, haematoma, or infection
- Activity restriction: Avoid heavy lifting for 4–6 weeks post open repair; return to normal activities sooner after laparoscopic repair
6. Complications of Hernias
Complications Related to the Hernia Itself
| Complication | Features |
|---|---|
| Incarceration | Irreducible hernia; no blood supply compromise yet; surgical urgency |
| Strangulation | Vascular compromise → ischemia → gangrene; surgical emergency |
| Bowel obstruction | Second only to adhesions as the most frequent cause of SBO in western countries |
| Richter hernia strangulation | Partial wall necrosis without complete obstruction — easily missed |
Complications of Hernia Repair
Urinary retention — most common early complication; predisposed by general/regional anaesthesia, opioid use, older age, BPH, overhydration, prolonged operative time. Managed with intermittent catheterisation ± alpha-blockers (tamsulosin, prazosin).
Ileus — more common after laparoscopic than open repair; usually resolves spontaneously.
Haematoma / Seroma — common, especially after mesh repairs; most resolve spontaneously.
Wound infection — risk increases with contamination, obesity, diabetes; mesh infection may require mesh removal.
Chronic groin pain (inguinodynia) — significant morbidity; occurs in up to 10% after open repair; possibly reduced with laparoscopic approach and careful nerve identification/preservation.
Recurrence:
- Tissue repairs: ~10%+
- Tension-free mesh repairs: ≤ 2% at specialist centres
- Factors increasing recurrence: contaminated field, emergency repair, sutured repair without mesh, early postoperative complications, reoperation for recurrence
- Incisional hernias: 20–50% recurrence with primary suture repair
Visceral / Vascular injury — rare; bowel or iliac vessel injury in laparoscopic repairs.
Testicular complications — ischaemic orchitis, testicular atrophy (injury to testicular vessels).
Mesh-related complications — chronic mesh pain, mesh migration, mesh erosion into bowel (rare), mesh infection (higher risk in contaminated fields).
7. Strangulated Hernia
Definition
Strangulation occurs when the blood supply to hernia contents (usually bowel, omentum, or ovary) is cut off by the hernia ring. Venous obstruction occurs first → oedema and swelling → arterial occlusion → ischaemia → gangrene within hours.
Incarceration Risks by Hernia Type
| Hernia | Risk |
|---|---|
| Femoral | ~45% (highest) — narrow rigid ring |
| Indirect inguinal (infant < 3 months) | ~30% |
| Spigelian | ~20% |
| Incisional | ~17% |
| Umbilical (adult) | Higher than child |
| Direct inguinal | Low (wide neck) |
Clinical Features
- Severe, constant pain at the hernia site — no longer relieved by reducing the hernia
- Tender, tense, irreducible swelling — erythema and oedema of overlying skin in late cases
- Systemic signs: fever, tachycardia, leucocytosis → signs of sepsis with perforation
- Bowel obstruction symptoms if lumen is compromised (absent in Richter hernia until > 50% circumference involved)
- Absence of cough impulse — contents are strangulated and fixed
Management — Surgical Emergency
- Resuscitation: IV fluids, correct electrolytes and acid-base; IV broad-spectrum antibiotics (covering gram-negatives and anaerobes); nasogastric decompression if obstructed
- Urgent surgery: Do not delay — the hernia is reduced, contents assessed for viability
- Viable bowel: Reduce and leave; repair the hernia defect
- Non-viable bowel: Resect + primary anastomosis or stoma depending on contamination and patient stability
- Mesh use in strangulation: Controversial. For inguinal hernias, current evidence does not treat mesh as contraindicated, but open tissue repair is generally preferred to save mesh for recurrence should it occur. For ventral hernias without ischemia, mesh can be used; with bowel resection and contamination, mesh risks (infection, fistula) increase significantly
- Postoperative care: ICU if septic; wound surveillance; may require staged repair
Femoral hernias are particularly prone to incarceration and bowel necrosis due to the small size of the hernia inlet. When hernia is identified as the cause of obstruction, the patient is quickly resuscitated, given antibiotics, and taken to the operating room. — Mulholland and Greenfield's Surgery, p. 2429
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine, pp. 1039–1044 | Mulholland and Greenfield's Surgery: Scientific Principles and Practice – 7e, pp. 2429–2432, 3707–3729
This is a shared conversation. Sign in to Orris to start your own chat.