Ototoxicity in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Searching Images
ototoxicity cochlear hair cell damage aminoglycoside cisplatin mechanism
Now I have comprehensive information from Cummings Otolaryngology and KJ Lee's (related to the topics Scott Brown, Dhingra, Hazarika etc. cover). Let me compile the complete 50-mark answer.
OTOTOXICITY — Comprehensive 50-Marks Answer
(Aligned with RGUHS University ENT curriculum)
DEFINITION
Ototoxicity refers to the tendency of a drug or chemical agent to cause inner ear dysfunction, producing symptoms of hearing loss and/or vestibular disturbance. Inner ear tissues may be damaged either temporarily or permanently.
— Cummings Otolaryngology Head and Neck Surgery
CLASSIFICATION OF OTOTOXIC DRUGS
┌─────────────────────────────────────────────────────────────────┐
│ OTOTOXIC AGENTS │
├───────────────────┬───────────────────┬─────────────────────────┤
│ ANTIBIOTICS │ CHEMOTHERAPEUTICS│ MISCELLANEOUS │
│ │ │ │
│ • Aminoglycosides │ • Cisplatin │ • Loop Diuretics │
│ - Streptomycin │ • Carboplatin │ - Furosemide │
│ - Gentamicin │ • Nitrogen │ - Ethacrynic acid │
│ - Tobramycin │ mustard │ - Bumetanide │
│ - Kanamycin │ │ • Antimalarials │
│ - Amikacin │ │ - Quinine │
│ - Neomycin │ │ - Chloroquine │
│ - Netilmicin │ │ • Salicylates (Aspirin) │
│ • Erythromycin │ │ • Heavy metals │
│ │ │ • Opioids (abuse) │
└───────────────────┴───────────────────┴─────────────────────────┘
Relative Vestibulotoxicity vs Cochleotoxicity (Aminoglycosides):
SGT KAN mnemonic (Vestibulotoxic → Cochleotoxic order) Streptomycin → Gentamicin → Tobramycin → Kanamycin → Amikacin → Neomycin
| Drug Class | Duration | Primary Target | Site of Damage |
|---|---|---|---|
| Aminoglycosides | Permanent | Drug-specific (cochlear or vestibular) | Inner row OHCs at cochlear basal turn; Stria vascularis |
| Platinum compounds (Cisplatin) | Permanent | Cochlea | Inner row OHCs at cochlear basal turn; Stria vascularis |
| Loop Diuretics | Transient | Cochlea | Stria vascularis |
| Quinine | Transient | Cochlea | Stria vascularis; Organ of Corti |
| Salicylates | Transient | Cochlea | None (functional only) |
— KJ Lee's Essential Otolaryngology
AMINOGLYCOSIDE OTOTOXICITY
Incidence
- Overall auditory toxicity: ~20%
- Vestibulotoxicity: ~15% — Cummings
Risk Factors
┌──────────────────────────────────────────────┐
│ RISK FACTORS FOR OTOTOXICITY │
│ │
│ Patient Factors Drug Factors │
│ ─────────────── ──────────── │
│ • Renal dysfunction • High cumulative │
│ • Hepatic dysfunction dose │
│ • Bacteraemia • Concomitant loop │
│ • Fever diuretic │
│ • Pre-existing HL • Rapid infusion │
│ • Advanced age • Repeated courses │
│ • A1555G mitochondrial │
│ 12S rRNA mutation │
│ • Prior noise exposure │
└──────────────────────────────────────────────┘
Genetic Susceptibility
- The A1555G mutation in mitochondrial 12S rRNA makes human rRNA resemble bacterial rRNA — the drug's target.
- Found in ~17% of aminoglycoside-induced hearing loss patients.
- Particularly common in certain Chinese populations (~5–6% of population; responsible for 1/3 of aminoglycoside ototoxicity cases there).
- Only the auditory system (not vestibular) is sensitized by this mutation. — Cummings
PATHOPHYSIOLOGY / MECHANISMS OF OTOTOXICITY
1. Aminoglycoside — Mechanism
FLOW CHART: Aminoglycoside Ototoxicity Pathway
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Aminoglycoside systemic administration
│
▼
Crosses into stria vascularis marginal cells
(via capillary circulation)
│
▼
Enters endolymph
│
▼
Enters hair cells via:
├── Mechanotransducer (MET) channels (primary)
└── TRPA1 non-selective cation channels
│
▼
Binds phosphatidylinositol on cell membrane
│
▼
Chelates iron → generates Reactive Oxygen Species (ROS)
│
▼
Targets intracellular organelles:
├── Mitochondria (primary target)
├── Endoplasmic reticulum
└── Binds cytosolic rRNA
│
▼
Outer Hair Cell (OHC) damage
[Starts at INNER ROW of OHCs]
[BASAL TURN first → apical progression]
│
▼
→ High-frequency SNHL first → progresses to lower frequencies
→ Stria vascularis damage
│
▼
IRREVERSIBLE hair cell loss
Key cellular mechanism of OHC death:
- ROS/RNS activate p53
- Activates caspase cascade: Caspase-8 → BID → BAX (translocates to mitochondria) → cytochrome-c leakage → Caspase-9 → Caspase-3/7 → Apoptosis — Cummings
2. Cisplatin — Mechanism
FLOW CHART: Cisplatin Ototoxicity Pathway
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Systemic cisplatin
│
▼
Long-term retention in cochlea
(platinum detectable 60 days after last dose)
│
▼
Activates cochlea-specific enzyme: NOX-3
(NADPH oxidase isoform unique to cochlea)
│
▼
↑↑ Superoxide production
│
▼
┌──────┴─────────┐
│ │
▼ ▼
H₂O₂ + Nitric oxide → Peroxynitrite
│ │
▼ (Fe²⁺ catalysed) ▼
Hydroxyl radical (•OH) Nitrotyrosine in
│ auditory neurons
▼
Reacts with membrane
polyunsaturated fatty acids
│
▼
4-Hydroxynonenal (highly toxic aldehyde)
│
▼
↓ Glutathione in basal turn OHCs
│
▼
Outer Hair Cell (OHC) apoptosis
[Basal turn OHCs most susceptible]
│
▼
High-frequency permanent bilateral SNHL
Cascade linkage confirmed: TRPV1 → NOX-3 → STAT1 → ROS → Hair cell apoptosis
— Cummings
COCHLEAR IMAGE — Anatomy of Damage
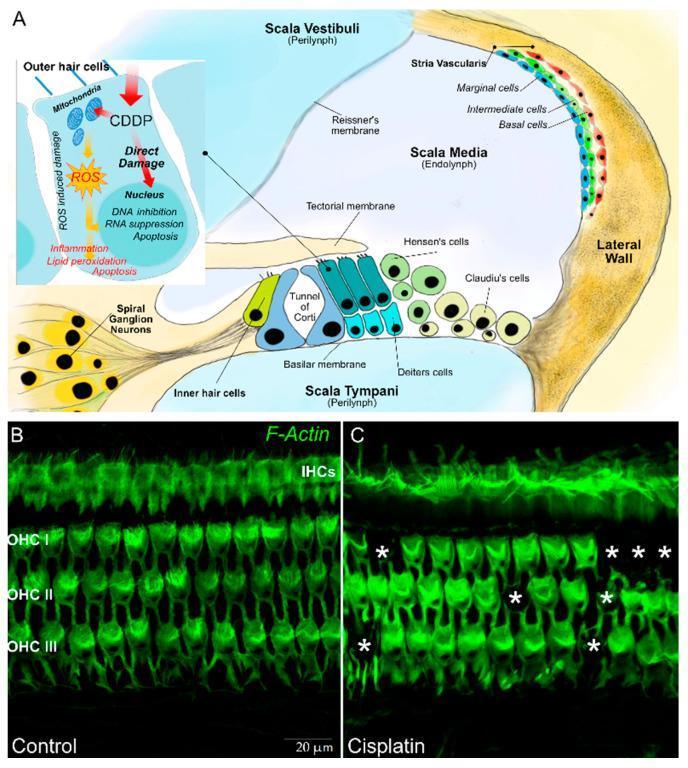
Panel A: Cochlear duct cross-section showing Scala vestibuli, Scala media (endolymph), Scala tympani, organ of Corti with IHC and 3 rows of OHCs, stria vascularis, spiral ganglion. Inset: CDDP → ROS → mitochondrial damage → apoptosis. Panels B&C: Fluorescence microscopy showing organized OHC rows in control vs gaps/loss in cisplatin-treated cochlea.
CLINICAL FEATURES
Cochleotoxicity (Hearing Loss)
- Bilateral, symmetric, sensorineural hearing loss
- High-frequency loss first (8 kHz, then extends downward)
- Permanent with aminoglycosides and cisplatin
- Preceded/accompanied by tinnitus (2–36% with cisplatin)
- May have ear pain (cisplatin)
- OAE abnormalities precede subjective hearing loss (early monitoring tool)
Vestibulotoxicity
- Oscillopsia (visual blurring during head movement)
- Gait imbalance, ataxia
- Symptoms worse in darkness
- Bilateral vestibular loss → difficult to compensate
- Recovery of oscillopsia from aminoglycosides is rarely complete
- Rotational testing: low-frequency responses affected first and most severely — Cummings
Salicylate Ototoxicity
- Tinnitus consistently at 6–8 g/day of aspirin
- Dose-dependent, reversible SNHL (resolves within 72 hours of stopping)
- Caloric responses also reduced
- Mechanism: prostaglandin inhibition → vasoconstriction of cochlear vasculature; inhibition of outer hair cell electromotility (prestin inhibition)
Loop Diuretic Ototoxicity
- Typically reversible, bilateral symmetric SNHL, sudden onset
- Block Na⁺-K⁺-2Cl⁻ symporter → alter strial metabolism → electrolyte imbalance in endolymph → ↓ endocochlear potential
- Greater with ethacrynic acid than furosemide
- Synergistic toxicity with aminoglycosides (most dangerous combination)
Quinine Ototoxicity
- Cinchonism: tinnitus, headache, nausea, disturbed vision
- Primarily cochleotoxic; usually transient
- Permanent loss at high doses or in sensitive patients
- Mechanism: reversible vasculitis and ischaemia of inner ear
- Degeneration in organ of Corti and stria vascularis
CISPLATIN — CLINICAL OTOTOXICITY DETAILS
Risk Factors for Cisplatin Ototoxicity:
- Young age (<5 years) or elderly
- Male children
- Cumulative dose >400 mg/m²
- Noise exposure
- Combination with other ototoxic drugs
- Nutritional depletion and anaemia
- Cranial irradiation (>48 Gy cochlear dose particularly dangerous in nasopharyngeal carcinoma)
Key Clinical Points:
- SNHL in >50% of patients; tinnitus in 7%
- Ultra-high frequency audiometry (>8 kHz) may show 100% incidence with high doses (150–225 mg/m²)
- Hearing loss at 8 kHz after 2 cycles predicts future need for hearing support
- Carboplatin: more ototoxic than initially thought; high-dose (2 g/m²) causes HL in 82% of children
MONITORING OF OTOTOXICITY
OTOTOXICITY MONITORING PROTOCOL
═══════════════════════════════
Pre-treatment:
├── Baseline pure-tone audiogram (250 Hz–8 kHz)
├── Ultra-high frequency audiometry (>8 kHz)
├── OAE (DPOAE/TEOAE)
├── ABR (in children/non-cooperative patients)
└── Vestibular function tests (if applicable)
During treatment:
├── Repeat UHF audiometry after each 2 cycles (cisplatin)
├── Monitor serum drug levels (aminoglycosides — peak & trough)
└── Monitor renal function (creatinine, GFR)
Post-treatment:
├── 6-weekly audiometry during treatment
├── 3-monthly for 1 year post completion
└── Refer for hearing aids/cochlear implants if significant SNHL
GRADING (Chang/Brock/SIOP-Boston scale widely used):
Grade 0 — No change from baseline
Grade 1 — High frequency loss (>8 kHz) only
Grade 2 — ≥20 dB at 4 kHz and above
Grade 3 — ≥20 dB at 2 kHz and above
Grade 4 — Requires hearing aids/cochlear implants
TOPICAL OTOTOXIC AGENTS
- Neomycin, gentamicin, tobramycin topical ear preparations are ototoxic if tympanic membrane is not intact
- With intact TM: no significant ototoxicity clinically
- With perforation/chronic OM: reduced permeability of inflamed round window, dilution by purulent fluid, and hyperaemic absorption reduce (but do not eliminate) toxicity
- AAO-HNS (2004) recommends against aminoglycoside topical use in the middle ear unless no alternative is available
- Intratympanic gentamicin is used therapeutically for chemical labyrinthectomy in Menière's disease — Cummings
PROTECTION AGAINST OTOTOXICITY
Against Aminoglycoside Ototoxicity:
- Salicylate pre-treatment (reduces aminoglycoside ototoxicity — paradoxically)
- Single daily dosing rather than multiple doses (reduces cochlear accumulation)
- Monitoring serum peak & trough levels
- Avoid concomitant loop diuretics
Against Cisplatin Ototoxicity — Antioxidants:
┌──────────────────────────────────────────────────────┐
│ OTOPROTECTIVE AGENTS (CISPLATIN) │
├─────────────────────┬────────────────────────────────┤
│ Systemic │ Intratympanic (preferred — │
│ │ avoids interference with │
│ │ antitumour effect) │
├─────────────────────┼────────────────────────────────┤
│ • N-acetylcysteine │ • Dexamethasone │
│ • α-Tocopherol │ • siRNA against NOX-3 │
│ • Lipoic acid │ • Sodium thiosulfate │
│ • D-methionine │ (6 hrs after cisplatin) │
│ • Amifostine │ │
│ • Sodium thiosulfate│ │
│ • Ebselen │ │
└─────────────────────┴────────────────────────────────┘
Phase 3 Trial Result: Sodium thiosulfate (6 hrs after cisplatin) protected against cisplatin-induced hearing loss in children without compromising antitumour efficacy.
Amifostine: Protected hearing in medulloblastoma children — 14.5% needed hearing aids vs 37.1% controls (P=0.005).
Important: No FDA-approved pharmacological agent exists to prevent or reverse platinum-induced hearing loss.
— Cummings
RADIATION OTOTOXICITY
- Head and neck/skull base irradiation causes SNHL
- Cochlear dose >48 Gy significantly increases risk (especially with concomitant cisplatin — nasopharyngeal carcinoma)
- IMRT (Intensity-Modulated Radiotherapy): Only 13% with grade 3/4 HL vs 64% with conventional RT
- Mechanism: strial damage, spiral ganglion degeneration, cochlear fibrosis — Cummings
HYDROCODONE ABUSE OTOTOXICITY
- Rapidly progressive bilateral SNHL (12 cases reported)
- Unilateral in 4/12 cases; vestibular symptoms in 1/12
- Steroid-resistant — does not respond to corticosteroids
- Cochlear implant successful (7/8 cases)
- Mechanism: μ-type opioid receptors in spiral and Scarpa's ganglia; δ- and κ-type receptors in hair cells — Cummings
RECENT ADVANCES
╔══════════════════════════════════════════════════════════════════╗
║ RECENT ADVANCES IN OTOTOXICITY ║
╠══════════════════════════════════════════════════════════════════╣
║ ║
║ 1. MOLECULAR TARGETS: ║
║ • TRPA1 channel blockade prevents AG hair cell uptake ║
║ • siRNA against NOX-3 prevents cisplatin ototoxicity ║
║ • TRPV1–NOX-3–STAT1 cascade identified in cisplatin HL ║
║ • KSR1 scaffold protein — MAPK pathway activation in OHC ║
║ ║
║ 2. GENETIC TESTING: ║
║ • A1555G mitochondrial 12S rRNA mutation screening ║
║ before aminoglycoside therapy ║
║ • Multiple pharmacogenetic associations found for ║
║ cisplatin susceptibility ║
║ ║
║ 3. NOVEL DRUG DELIVERY: ║
║ • Intratympanic drug delivery (avoids systemic effects) ║
║ • Cisplatin nanoparticles with localised cochlear delivery ║
║ • Hydrogel-based round window membrane drug delivery ║
║ ║
║ 4. BIOMARKERS: ║
║ • UHF audiometry + DPOAEs as early biomarkers ║
║ • Long-term platinum retention in cochlea demonstrated ║
║ (explains delayed-onset hearing loss post-cisplatin) ║
║ ║
║ 5. OTOPROTECTION: ║
║ • Phase 3 trial: Sodium thiosulfate protects vs cisplatin ║
║ • AMPHIA trial ongoing (D-methionine) ║
║ • CPI-455 (histone demethylase inhibitor) — preserves ║
║ hair cells and spiral ganglion neurons post-cisplatin ║
║ ║
║ 6. NEW AGENTS: ║
║ • Apramycin (veterinary AG) — significant antimicrobial ║
║ efficacy with claimed minimal ototoxicity (ongoing study) ║
║ • ERK pathway inhibitors (gentamicin-induced OHC damage) ║
║ ║
╚══════════════════════════════════════════════════════════════════╝
SUMMARY DIAGRAM — OVERALL OTOTOXICITY FRAMEWORK
OTOTOXIC AGENT
│
┌─────────────┴──────────────┐
│ │
COCHLEA VESTIBULE
(Cochleotoxicity) (Vestibulotoxicity)
│ │
Outer Hair Cells Type I Hair Cells
(Basal turn first) (Crista ampullaris,
Stria vascularis Macula utriculi/sacculi)
│ │
SNHL (High freq first) Oscillopsia, Ataxia,
Tinnitus Dizziness, Imbalance
│ │
┌──────┴──────────────────────┐ │
│ MECHANISMS │ │
│ • ROS/RNS generation │ │
│ • Iron chelation │ │
│ • Mitochondrial damage │ │
│ • Apoptotic cascade │ │
│ (Caspase 3/7/8/9) │ │
│ • NOX-3 activation │ │
│ (cisplatin only) │ │
└─────────────────────────────┘ │
│ │
MONITORING MONITORING
Audiogram (UHF) Caloric test
OAE, ABR vHIT, VEMP
Drug levels Rotational chair
│
PREVENTION / TREATMENT
├── Antioxidants (NAC, α-tocopherol, D-methionine)
├── Sodium thiosulfate (cisplatin)
├── Avoid nephrotoxic drugs concurrently
├── Single daily dosing (aminoglycosides)
├── Genetic screening (A1555G mutation)
├── Intratympanic dexamethasone
└── Hearing aids / Cochlear implants (if severe)
QUICK REFERENCE TABLE — IMPORTANT FACTS FOR EXAMS
| Feature | Aminoglycosides | Cisplatin | Loop Diuretics | Salicylates | Quinine |
|---|---|---|---|---|---|
| Type of HL | Permanent SNHL | Permanent SNHL | Transient SNHL | Transient SNHL | Usually transient |
| Frequency affected first | High (8 kHz) | High (4–8 kHz) | All (flat) | All (flat) | All |
| Primary site of damage | OHC + Stria vascularis | OHC (basal turn) | Stria vascularis | None (functional) | Stria + OoC |
| Tinnitus | Yes | Yes (2–36%) | Yes | Yes (at 6–8 g/day) | Yes (cinchonism) |
| Vestibulotoxicity | Yes (streptomycin, gentamicin most) | Minimal | No | No | Rare |
| Dose-dependence | Yes | Yes (>400 mg/m²) | Yes | Yes (>2.7 g) | Yes |
| Genetic factor | A1555G mt rRNA | Multiple SNPs | No | No | No |
REFERENCES (Textbook Sources)
- Cummings Otolaryngology Head and Neck Surgery (6th ed., Flint et al.) — Chapter on Ototoxicity: pp. 3010–3025
- KJ Lee's Essential Otolaryngology (11th ed.) — Ototoxicity section, pp. 226–227
- Goodman & Gilman's The Pharmacological Basis of Therapeutics — Aminoglycoside and loop diuretic ototoxicity
- Dhingra's Diseases of Ear, Nose and Throat — Ototoxic drugs (standard RGUHS reference)
- Hazarika's Textbook of ENT — Drug-induced hearing loss
- Scott Brown's Otorhinolaryngology Head and Neck Surgery — Inner ear pharmacology and ototoxicity
- Zakir Hussain's ENT — Ototoxicity (Indian PG reference)
- Stell & Maran's Head and Neck Surgery — Relevant otology section
Key Exam Points to Remember for RGUHS 50-Marks:
- Define → Classify (with table) → Mechanism (flowchart for AG + cisplatin separately) → Clinical features (cochleo vs vestibulo) → Monitoring protocol → Protection/treatment → Recent advances
- The mnemonic SGT KAN for aminoglycoside vestibulo→cochleotoxic order
- A1555G mutation = genetic predisposition to AG ototoxicity
- NOX-3 = cochlea-specific enzyme activated by cisplatin
- Sodium thiosulfate = most promising otoprotectant (Phase 3 trial positive)
- No FDA-approved drug currently exists to prevent cisplatin ototoxicity
- Loop diuretics + aminoglycosides = most dangerous synergistic combination
This is a shared conversation. Sign in to Orris to start your own chat.