Q. Describe the clinical features, staging and management of malignancy of external auditory canal. in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Malignancy of the External Auditory Canal (EAC)
A Comprehensive Essay for 50 Marks | RGUHS ENT
INTRODUCTION
Carcinoma of the external auditory canal (EAC) is a rare but aggressive malignancy, constituting less than 0.2% of all head and neck cancers and approximately 1 in 1,000,000 population per year. Despite its rarity, the proximity of the EAC to critical neurovascular structures — the facial nerve, internal carotid artery, jugular bulb, otic capsule, dura, and parotid gland — makes management both challenging and consequential. Squamous cell carcinoma (SCC) is the most common histological type, followed in decreasing frequency by basal cell carcinoma (BCC), adenocarcinoma, adenoid cystic carcinoma (AdCC), mucoepidermoid carcinoma, ceruminoma, melanoma, and sarcoma.
"SCC is the most common primary malignancy of the temporal bone." — K.J. Lee's Essential Otolaryngology, p. 491
ANATOMY RELEVANT TO EAC MALIGNANCY
┌─────────────────────────────────────────────────────────────┐
│ EXTERNAL AUDITORY CANAL │
│ │
│ Outer 1/3: Cartilaginous (fibrocartilage) │
│ - Ceruminous glands, hair follicles │
│ - Fissures of Santorini → parotid spread │
│ │
│ Inner 2/3: Osseous (tympanic bone) │
│ - Thin skin, no adnexa │
│ - Close to: TM, middle ear, mastoid, facial n. │
│ │
│ LENGTH: ~25 mm | Lined by squamous epithelium │
└─────────────────────────────────────────────────────────────┘
↓ Anteriorly ↓ Superiorly ↓ Posteriorly
Parotid / TMJ Tegmen / Middle Mastoid
cranial fossa cortex
Lymphatic Drainage (Clinically critical for staging):
- Anterior canal wall / lateral pinna → Pre-auricular (parotid) nodes
- Posterior canal wall / upper pinna → Post-auricular nodes
- Floor of EAC / lobule → Superficial and deep cervical nodes (levels II–III)
- Nodes → ultimately drain into deep cervical chain (K.J. Lee's Essential Otolaryngology, p. 471)
AETIOPATHOGENESIS & RISK FACTORS
| Risk Factor | Mechanism |
|---|---|
| Chronic otitis externa / otitis media | Chronic irritation → dysplasia → carcinoma |
| Prior irradiation | DNA damage → second malignancy |
| Exposure to coal dust / petroleum byproducts | Occupational carcinogen |
| Immunosuppression | Reduced tumour surveillance |
| Rarely — Keratosis obturans | Chronic mucosal irritation |
The fissures of Santorini in the anterior cartilaginous EAC allow tumour spread to the parotid gland. The bony EAC lacks these natural barriers, but when tumour erodes through it, spread to the middle ear, mastoid, and skull base occurs rapidly.
PATHOLOGY
Histological Types
EAC MALIGNANCIES
│
├── Squamous Cell Carcinoma (SCC) ─────── MOST COMMON (~60-70%)
│ └── Well / moderately / poorly differentiated
│
├── Basal Cell Carcinoma (BCC) ──────────── ~45% of all ear skin cancers
│ └── Serpiginous ulceration, lacks pearly edges in canal
│
├── Adenoid Cystic Carcinoma (AdCC) ─────── Perineural spread ++
│ └── Appears as small pimple; severe pain; slow growing
│
├── Ceruminous Adenocarcinoma ───────────── Arises from ceruminous glands
│
├── Mucoepidermoid Carcinoma
│
├── Malignant Melanoma ──────────────────── 7% of H&N sites involve ear
│
└── Sarcoma / Rhabdomyosarcoma (children)
CLINICAL FEATURES
Symptoms (in decreasing order of frequency)
| Symptom | Significance |
|---|---|
| Otalgia | Most common; deep-seated, unrelenting |
| Otorrhoea | Blood-stained / serosanguineous discharge; fails to respond to antibiotics |
| Hearing loss | Conductive (canal obstruction); SNHL indicates labyrinthine invasion |
| Facial nerve palsy | Invasion of fallopian canal → late sign; poor prognosis (→ T4) |
| Trismus | TMJ / infratemporal fossa involvement |
| Vertigo | Labyrinthine invasion — advanced disease |
| Parotid mass / neck nodes | Regional metastasis — grave prognosis |
| Headache | Dural or intracranial extension |
"Persistence of otitis externa despite adequate management by routine treatment measures should increase suspicion for carcinoma." — Cummings Otolaryngology, p. [Ch. 178]
Signs on Examination
- Polypoid / meaty / granular lesion in EAC
- Foul-smelling or blood-stained discharge
- BCC: serpiginous ulceration (no pearly rolled edges — thin canal skin)
- AdCC: epithelium-covered, nodular, intensely painful lesion
- Hard, fixed parotid mass / pre-auricular or cervical lymphadenopathy
- Facial nerve palsy (LMN type)
- Cranial nerve involvement in advanced stages (V, IX, X, XI, XII)
DIFFERENTIAL DIAGNOSIS
Malignant EAC Lesion (Blood-stained discharge + otalgia)
│
├── Malignant Otitis Externa (MOE / Skull base osteomyelitis)
│ - Pseudomonas; diabetic/elderly; granulation at BCC junction
│ - Radiologically indistinguishable → BIOPSY mandatory
│
├── Keratosis Obturans (EAC cholesteatoma)
│
├── Chronic Otitis Externa
│
└── Necrotising (Malignant) Otitis Externa
"CT and MRI alone cannot differentiate MOE from malignancy — biopsy of any unusual EAC tissue is mandatory." — Cummings Otolaryngology
INVESTIGATIONS
1. Biopsy
- Mandatory — punch biopsy of granular tissue
- Beware pseudoepitheliomatous hyperplasia (benign mimic requiring expert histopathological review)
2. Audiological Assessment
- Pure tone audiometry: conductive vs sensorineural loss
- Tuning fork tests
3. Imaging
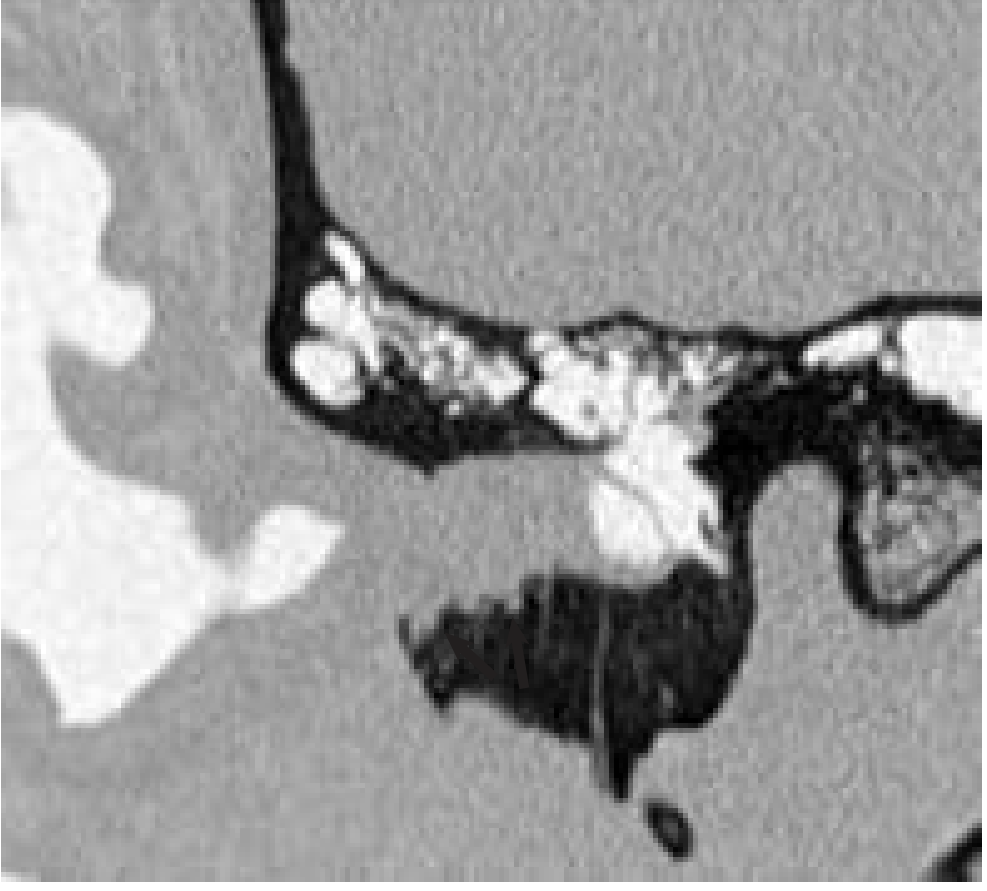
HRCT Temporal Bone (First-line)
- Demonstrates bony destruction of EAC walls
- Extent to middle ear, mastoid, otic capsule, carotid canal
- Heterogeneously enhancing mass with aggressive bone destruction
MRI Temporal Bone + Neck
- T1WI: Low signal mass with peripheral enhancement
- T2WI: Heterogeneous high signal
- Superior to CT for: dural, intracranial, perineural (AdCC), and soft tissue involvement
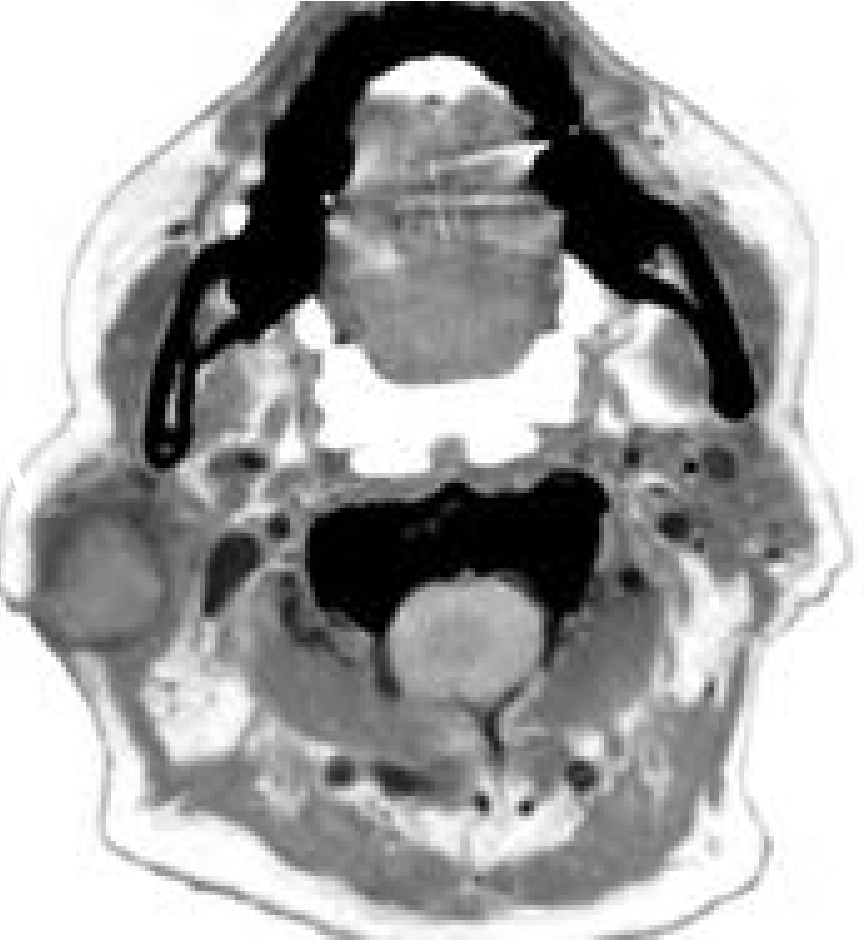
CT Neck with Contrast
- Parotid/pre-auricular and cervical lymphadenopathy
- Necrotic nodes = established metastatic disease
CT Chest / PET-CT
- Distant metastasis (lung most common)
- PET-CT increasingly used for staging and post-treatment surveillance
STAGING
Modified University of Pittsburgh Staging System (Arriaga & Janecka, modified by Moody et al. 2000)
The most widely used system for SCC of the temporal bone / EAC
(K.J. Lee's Essential Otolaryngology, p. 491; Cummings Otolaryngology Ch. 178)
┌──────────────────────────────────────────────────────────────────────────┐
│ MODIFIED UNIVERSITY OF PITTSBURGH TNM STAGING (EAC / Temporal Bone) │
├─────────┬──────────────────────────────────────────────────────────────── ┤
│ T Stage │ Extent of Disease │
├─────────┼────────────────────────────────────────────────────────────────┤
│ T1 │ Tumor limited to EAC — no bony erosion, no soft tissue │
│ │ extension │
├─────────┼────────────────────────────────────────────────────────────────┤
│ T2 │ Limited bony EAC erosion (not full-thickness) OR │
│ │ < 0.5 cm soft tissue involvement │
├─────────┼────────────────────────────────────────────────────────────────┤
│ T3 │ Full-thickness bony EAC erosion with < 0.5 cm soft tissue │
│ │ involvement OR involves middle ear AND/OR mastoid │
├─────────┼────────────────────────────────────────────────────────────────┤
│ T4 │ Erodes medial wall of middle ear to involve: │
│ │ cochlea, labyrinth, petrous apex, jugular foramen, │
│ │ carotid canal, dura; OR > 0.5 cm soft tissue (TMJ, │
│ │ styloid, parotid); OR facial nerve palsy │
└─────────┴────────────────────────────────────────────────────────────────┘
NODAL STATUS:
N0 — No regional lymph node metastasis
N+ — Regional lymph node metastasis (→ automatically Stage III/IV)
METASTATIC STATUS:
M0 — No distant metastasis
M1 — Distant metastasis (→ automatically Stage IV)
Overall Stage Grouping (University of Pittsburgh)
| Stage | Criteria |
|---|---|
| Stage I | T1 N0 M0 |
| Stage II | T2 N0 M0 |
| Stage III | T3 N0 M0 or T1/T2/T3 N+ M0 |
| Stage IV | T4 any N M0 or Any T any N M1 |
"Involvement of lymph nodes is a poor prognostic finding and automatically places the patient in an advanced stage." — Cummings Otolaryngology (Box 178.2)
Pittsburgh vs. Other Staging Systems
| System | Basis | Notes |
|---|---|---|
| Pittsburgh (Modified) | CT + clinical + intraop | Most widely used |
| Stell & Maran Staging | 4-stage clinical system | Based on bone involvement |
| AJCC Skin SCC staging | Size-based T staging | For pinna/skin; not EAC-specific |
| UICC | Generic soft tissue | Not tailored to temporal bone |
AJCC Pinna/Skin SCC T-Staging (for comparison):
| T | Size |
|---|---|
| T1 | ≤ 2 cm |
| T2 | 2–5 cm |
| T3 | > 5 cm |
| T4 | Deep structure invasion (bone, cartilage, muscle) |
MANAGEMENT
Management Algorithm
SUSPECTED EAC MALIGNANCY
│
Biopsy (Histopathology)
│
┌────────────────┴────────────────┐
BENIGN MALIGNANT
│ │
Follow up HRCT + MRI Temporal Bone
CT Neck + Chest
PET-CT (if T3/T4)
Audiogram
│
STAGING (University of Pittsburgh)
│
┌──────────┬──────────┬─────────┴──────────┐
T1 T2 T3 T4
│ │ │ │
Sleeve Lateral Sub-total Total/near-total
Resection TBR (LTBR) TBR (STBR) TBR ± parotidectomy
│ │ │ ± neck dissection
│ └──────────┴─────────────────────┤
Parotidectomy if parotid involved │
Neck dissection if N+ (or T3/T4) │
│
POST-OPERATIVE XRT
(T2 and above — all cases)
± Concurrent chemotherapy
(T4, +ve margins, N+)
Surgical Options
1. Sleeve Resection (Canaloplasty)
- Indication: T1 — tumour limited to skin of EAC, no bone invasion
- Technique: Skin of bony EAC + cartilaginous EAC portion ± tympanic membrane excised; bony canal left intact
- Margin: Must be histologically negative
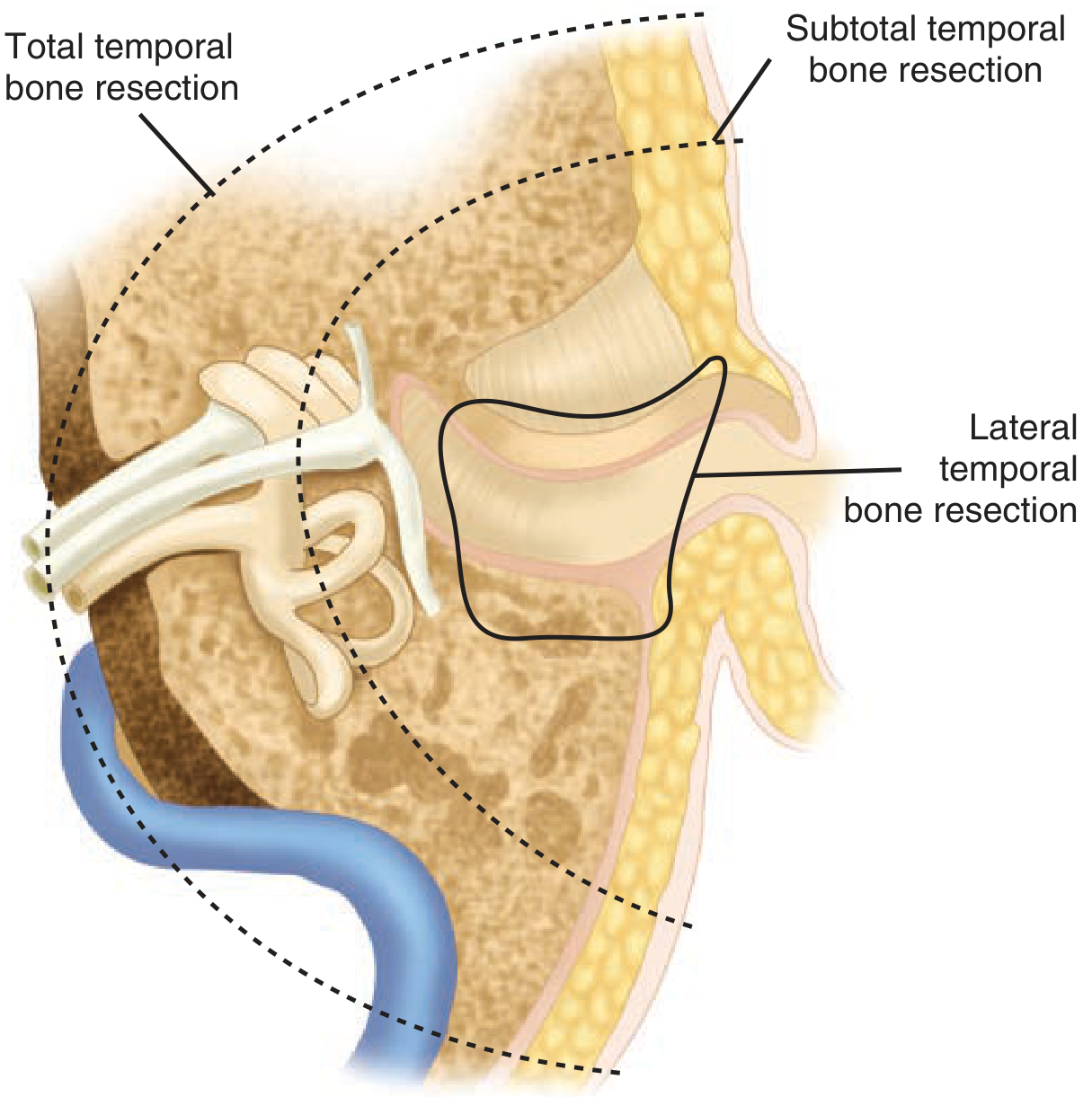
2. Lateral Temporal Bone Resection (LTBR)
- Indication: T2 (limited bony erosion) and early T3
- Removes: EAC en bloc — bony EAC + tympanic membrane + malleus + incus + cartilaginous canal
- Facial nerve preserved if not involved
- Technique:
- C-shaped post-auricular incision into cervical crease
- Intra-canal incision in cartilaginous EAC encompassing the lesion
- Flap elevated anteriorly to zygomatic root
- Subperiosteal mastoidectomy
- Canal sectioned at bony-cartilaginous junction → closed in layers
- Temporalis muscle / TPF flap preserved for reconstruction
3. Subtotal Temporal Bone Resection (STBR)
- Indication: T3 (middle ear and/or mastoid involvement)
- Removes: LTBR specimen + petrous apex, otic capsule drilling to negative margins
- Petrous ICA and dura preserved if uninvolved
- Parotidectomy + neck dissection frequently required
4. Total Temporal Bone Resection (TTBR)
- Indication: T4 — extension to cochlea, carotid canal, jugular foramen, dura
- Includes: STBR + sigmoid sinus ± petrous carotid artery
- No proven survival benefit over STBR + adjuvant therapy in most series
- Very few centres offer this procedure
- Sacrifice of facial nerve almost inevitable → immediate cable graft reconstruction
5. Parotidectomy and Neck Dissection
- Parotidectomy: when tumour reaches parotid via fissures of Santorini or direct extension
- Prophylactic parotidectomy ± neck dissection: recommended for T3 and T4 disease even when N0 (occult nodal rate ~10–20%)
- Therapeutic neck dissection: for N+ disease
- Regional failure after surgery is the most common cause of death
Summary: Surgery by Stage
| Stage | Surgical Procedure |
|---|---|
| T1 | Sleeve resection (wide local excision) |
| T2 | Lateral Temporal Bone Resection (LTBR) |
| T3 | Subtotal TBR (STBR) + consider parotidectomy + ND |
| T4 | STBR or Total TBR + parotidectomy + ND + adjuvant RT + consider concurrent chemo |
ADJUVANT THERAPY
Radiotherapy
- Standard recommendation: post-operative radiation for T2 and above
- Dose: 60–66 Gy (conventional fractionation) to temporal bone ± bilateral neck
- May include contralateral neck and parotid nodal basins in advanced cases
- Positive margins + RT → still almost uniformly fatal in carcinomas of the EAC
- SCC and BCC: radiosensitive
- AdCC: Intermediate; post-op RT reduces local recurrence
Chemotherapy
- Concomitant chemoradiotherapy (cisplatin-based) considered for:
- T4 tumours
- Positive/close surgical margins
- Nodal disease (N+)
- Perineural invasion (especially AdCC)
- Not established as primary therapy
Palliative Radiation
- For T4 patients where en bloc resection would be excessively deforming or futile
- Acceptable alternatives: lateral TBR + subtotal petrosectomy or total petrosectomy with chemoradiotherapy
SPECIAL HISTOLOGICAL TYPES
Adenoid Cystic Carcinoma (AdCC) of EAC
- Arises from ceruminous glands
- Perineural spread — hallmark feature; extensive skip lesions along nerve sheaths
- Clinically: intense otalgia, small pimple-like lesion
- Imaging: MRI essential to delineate perineural extension
- Treatment: wide surgery + post-op radiotherapy
- Proton beam / carbon ion therapy: 5-year local control >70% (K.J. Lee's, p. 491)
- Prognosis: late metastases (lung) even after apparent cure; 10-year survival better than expected
Basal Cell Carcinoma (BCC) of EAC
- Most common malignancy of the ear overall (~45%)
- Presents as erythematous lesion with raised margins
- Serpiginous ulceration in the canal (no pearly edges — thin adherent skin)
- Treatment: wide local excision; may require cartilage excision, skin graft, or local flaps
- Post-op RT in advanced or recurrent cases
RECONSTRUCTION
- Meatoplasty / split-skin graft: T1–T2 after sleeve resection
- Temporalis muscle flap / TPF flap: obliteration of cavity after LTBR
- Rectus abdominis free flap or pectoralis major flap: large defects after auriculectomy + STBR/TTBR
- Facial nerve grafting: cable graft (sural / great auricular nerve) at time of resection
PROGNOSIS AND OUTCOMES
| Stage | Approximate 5-Year Survival |
|---|---|
| T1 | ~80–85% |
| T2 | ~60–70% |
| T3 | ~30–50% |
| T4 | ~15–25% |
| N+ disease | Significant ↓ (Stage III/IV automatically) |
| Positive margins | Near 0% despite adjuvant RT |
Poor prognostic factors:
- Facial nerve palsy (T4 automatic → poor)
- Positive surgical margins
- Lymph node metastasis
- Dural invasion
- Delayed diagnosis
RECENT ADVANCES
| Advance | Detail |
|---|---|
| PET-CT | Superior staging and post-treatment surveillance; identifies occult nodes and distant mets |
| Proton beam / Carbon ion therapy | Used for AdCC and skull base extension; 5-year local control >70% |
| Intensity Modulated Radiotherapy (IMRT) | Better dose conformality, spares cochlea, parotid gland, brainstem |
| Endoscopic-assisted surgery | Minimally invasive approaches for T1 lesions |
| Robotic surgery | Emerging for parotid-neck dissection component |
| Targeted therapy | EGFR inhibitors (cetuximab) in recurrent/metastatic SCC |
| Immunotherapy | Pembrolizumab / nivolumab for recurrent/metastatic SCC (PD-L1+) |
| 3D navigation | Intraoperative CT navigation for skull base resections |
| Free flap reconstruction | Reduced morbidity; enables more aggressive resection |
| Sentinel lymph node biopsy | Under investigation for N0 EAC SCC |
FLOWCHART SUMMARY
CLINICAL PRESENTATION
Otalgia + Blood-stained discharge + Granular EAC polyp
│
┌──────────▼──────────┐
│ CLINICAL EXAM │
│ + Audiometry │
└──────────┬──────────┘
│
┌──────────▼──────────┐
│ BIOPSY (Mandatory) │
│ Histopathology │
└──────────┬──────────┘
│
┌────────────▼────────────┐
│ RADIOLOGICAL STAGING │
│ HRCT Temporal bone │
│ MRI + CT Neck/Chest │
│ PET-CT (T3/T4) │
└────────────┬────────────┘
│
┌────────────▼────────────────────────────────┐
│ MODIFIED PITTSBURGH STAGING SYSTEM │
└─────┬──────┬──────┬────────────────┬────────┘
│ │ │ │
T1 T2 T3 T4
│ │ │ │
Sleeve LTBR STBR STBR/TTBR
Resect. +Parotid +Parotid+ND
±ND +Flap recon
│ │ │ │
└──────┴──────┴────────────────┘
│
PORT-OP RADIOTHERAPY (T2+)
± CONCURRENT CHEMOTHERAPY
(T4, N+, +ve margins)
│
SURVEILLANCE (6-monthly imaging)
│
RECURRENCE? → Salvage surgery
or Palliation
KEY POINTS FOR EXAMINATION (RGUHS)
- Most common malignancy of EAC = SCC (followed by BCC, AdCC)
- Commonest presenting symptom = Otalgia + blood-stained otorrhoea
- Facial palsy = T4 (poor prognosis) — automatic upstaging
- Staging system used = Modified University of Pittsburgh (Arriaga & Janecka, modified by Moody 2000)
- T1 → sleeve resection; T2 → LTBR; T3 → STBR; T4 → STBR/TTBR
- Positive margins = near universally fatal even with post-op RT
- MOE vs carcinoma — biopsy mandatory to differentiate
- AdCC = perineural spread; intense pain; proton beam therapy
- BCC = most common ear skin malignancy (45%); serpiginous ulceration
- Post-op RT mandatory for T2 and above
REFERENCES / TEXTBOOK CITATIONS
| Source | Contribution |
|---|---|
| Cummings Otolaryngology Head and Neck Surgery (Ch. 135, 178) | Clinical features, imaging, staging, management algorithm, CT images |
| K.J. Lee's Essential Otolaryngology (Ch. 24, Tables 24-4, 24-5) | Pittsburgh staging table, surgical approaches by stage, tumour classification |
| Schwartz's Principles of Surgery, 11th Ed. (Ch. 18) | Temporal bone resection diagram (lateral, subtotal, total) |
| Stell & Maran's Head and Neck Surgery | Original staging concept, 4-stage system |
| Dhingra's Diseases of Ear, Nose and Throat | Clinical overview, BCC/SCC comparison |
| Hazarika's Textbook of ENT | Regional management perspective |
| Arriaga MA, Janecka IP (1990) | Original Pittsburgh staging proposal |
| Moody SA et al. (Am J Otol, 2000) | Modified Pittsburgh staging — facial palsy → T4 |
| Higgins TS & Antonio SA | Role of radiotherapy in EAC SCC |
"En bloc or complete gross surgical resection of EAC malignancies is the primary therapy for all tumour stages, with an adjunctive role for radiotherapy. Positive margins, despite postoperative radiotherapy, have an almost uniform fatal result."
— Cummings Otolaryngology Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.