Retrosigmoid approach in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Searching Images
retrosigmoid approach surgical anatomy craniotomy cerebellopontine angle
Reading File
Now I have comprehensive material. Let me compile the detailed 50-mark answer.
RETROSIGMOID APPROACH — A COMPREHENSIVE 50-MARK ANSWER
(As per RGUHS syllabus, with references from Cummings Otolaryngology, K.J. Lee's Essential Otolaryngology, and related sources)
1. INTRODUCTION & HISTORICAL BACKGROUND
The retrosigmoid approach (also called the suboccipital approach or posterior cranial fossa approach) is one of the three classic surgical routes to the cerebellopontine angle (CPA) and internal auditory canal (IAC). It is performed posterior to the sigmoid sinus, providing wide panoramic access to the posterior fossa without disturbing the labyrinth.
Historical milestones:
- First described by Sir Charles Ballance (1894) for acoustic neuroma surgery
- Cushing (1917) popularized bilateral suboccipital decompression
- Dandy (1925) introduced unilateral suboccipital approach with improved facial nerve identification
- Rand & Kurze (1965) introduced microsurgical technique
- Yasargil (1970s) refined microsurgical retrosigmoid technique
- Modern era: combination with endoscopy (key-hole retrosigmoid), intraoperative neurophysiological monitoring
2. SURGICAL ANATOMY OF THE CEREBELLOPONTINE ANGLE (CPA)
The CPA is a wedge-shaped subarachnoid cistern bounded by:
| Boundary | Structure |
|---|---|
| Anteromedial | Pons and medulla |
| Anterolateral | Petrous temporal bone |
| Lateral | Sigmoid sinus |
| Superior | Tentorium cerebelli |
| Inferior | Jugular foramen / foramen magnum |
Contents of CPA cistern:
- CN V (trigeminal) — superiorly
- CN VII & VIII bundle — entering IAC at porus acusticus
- CN IX, X, XI — inferiorly at jugular foramen
- AICA (anterior inferior cerebellar artery) — loops into IAC
- PICA (posteroinferior cerebellar artery)
- SCA (superior cerebellar artery)
The Internal Auditory Canal (IAC):
- Length: ~8–10 mm
- Divided by Bill's bar (vertical crest) and transverse crest
- Contains: facial nerve (anterosuperior), superior vestibular nerve (posterosuperior), cochlear nerve (anteroinferior), inferior vestibular nerve (posteroinferior)
3. INDICATIONS
Primary Indications:
- Acoustic neuroma (Vestibular Schwannoma)
- Best for tumors ≤2 cm CPA component with serviceable hearing
- Tumors with limited IAC involvement (not reaching fundus)
- CPA meningiomas (hearing preservation possible)
- Microvascular decompression (MVD)
- Trigeminal neuralgia (Jannetta procedure)
- Hemifacial spasm
- Glossopharyngeal neuralgia
- Non-acoustic CPA neoplasms — epidermoid cysts, facial schwannomas, meningiomas
- Facial nerve decompression (CPA–IAC segment)
- CPA arachnoid cysts
- Vascular lesions — AVMs, aneurysms of AICA/PICA
Advantages Over Other Approaches:
| Feature | Retrosigmoid | Translabyrinthine | Middle Fossa |
|---|---|---|---|
| Hearing preservation | ✅ Possible | ❌ No | ✅ Best |
| CPA exposure | ✅ Panoramic | ✅ Good | ❌ Limited |
| IAC fundus visualization | ❌ Indirect | ✅ Direct | ✅ Direct |
| Cerebellar retraction | Needed | Minimal | Not needed |
| Tumor size | All sizes | All sizes | Small/intracanalicular |
4. CONTRAINDICATIONS
- Tumor extending to fundus of IAC (relative contraindication for hearing preservation)
- Non-serviceable hearing (translabyrinthine preferred for large tumors)
- High jugular bulb obscuring access
- High-riding sigmoid sinus limiting posterior fossa dural exposure
- Patient unfit for posterior fossa surgery
5. PREOPERATIVE EVALUATION
Clinical Assessment:
- Pure tone audiometry (PTA) + Speech discrimination score (SDS)
- Serviceable hearing (Gardner-Robertson Class I–II): PTA ≤50 dB, SDS ≥50%
- Vestibular function tests: caloric tests, VNG
- Complete cranial nerve examination (V, VII, VIII, IX, X)
- Facial nerve grading (House-Brackmann scale — baseline)
Imaging:
- MRI brain with gadolinium — gold standard
- Size, location, IAC extension to fundus
- Relationship to brainstem
- Fluid-attenuating sequences for hearing preservation planning
- CT temporal bone — mastoid pneumatization, jugular bulb height, sigmoid sinus position
- CT angiography / MRA — vascular anatomy, AICA loop
Audiological:
- BAER (Brainstem Auditory Evoked Response) — baseline for intraoperative monitoring
6. PATIENT POSITIONING
Park-Bench (Lateral/Semilateral) Position — Most Common:
- Patient lateral decubitus, affected side up
- Head fixed in Mayfield 3-point cranial fixation frame
- Head tilted 15° toward floor, rotated 15° toward ceiling (brings retrosigmoid area upward)
- Shoulder roll under opposite shoulder
- All pressure points padded
- Neutral cervical position to avoid jugular venous obstruction
Supine with Head Rotation:
- Simpler, used for osteoclastic craniectomy
- Head turned 90° to contralateral side
Sitting Position (Historical / Rarely Used):
- Advantages: gravity-assisted CSF drainage, reduced bleeding
- Risks: venous air embolism (major concern), paradoxical air embolism through PFO
- Requires: Doppler monitoring, G-suit, central venous catheter
- Largely abandoned except at specific centers
Prone Position:
- Rarely used; for midline lesions
7. SURGICAL TECHNIQUE — STEP-BY-STEP
FLOWCHART: RETROSIGMOID APPROACH — SURGICAL STEPS
PATIENT PREPARATION & POSITIONING
│
▼
SKIN INCISION (Post-auricular / Lazy-S)
│
▼
SOFT TISSUE DISSECTION
(Reflect scalp flap anteriorly)
(Subperiosteal reflection of neck muscles)
│
▼
BONE WORK — RETROSIGMOID CRANIOTOMY
(4×3 cm bone flap posterior to sigmoid sinus,
inferior to transverse sinus)
│
┌─────┴──────┐
│ │
CRANIECTOMY BONE FLAP
(osteoclastic) (osteoplastic)
│ │
└─────┬──────┘
▼
SIGMOID SINUS SKELETONIZATION
& MASTOIDECTOMY (if needed)
│
▼
DURAL INCISION (curvilinear/C-shaped)
(Dural traction sutures → retract sigmoid sinus anteriorly)
│
▼
CSF DRAINAGE FROM CPA CISTERN
(Gradual — prevents cerebellar herniation)
│
▼
CEREBELLAR RETRACTION
(Slow, gentle — over 5-10 minutes)
│
▼
CPA EXPOSURE
(Identify flocculus, choroid plexus,
CN VII-VIII bundle)
│
▼
TUMOR IDENTIFICATION & DEBULKING
(If large: internal decompression first)
│
▼
FACIAL NERVE IDENTIFICATION
(Medially at brainstem first, then laterally)
(Nerve monitor used continuously)
│
▼
REMOVAL OF POSTERIOR LIP OF IAC
(Diamond bur drilling — limited by
posterior semicircular canal)
│
▼
COMPLETE TUMOR RESECTION
(Dissect tumor off facial nerve
toward porus acusticus)
│
▼
HEMOSTASIS + DURAL CLOSURE
(Fat graft — obliterate IAC + mastoid)
(Dura closed watertight)
│
▼
BONE FLAP REPLACEMENT / CRANIOPLASTY
│
▼
LAYERED WOUND CLOSURE + PRESSURE DRESSING
Step-by-Step Details:
A. INCISION
- Lazy-S (or reverse C-shaped) post-auricular incision, 2–3 cm behind the post-auricular crease
- Extends from above the pinna to the mastoid tip
- Skin flap reflected anteriorly, exposing the mastoid cortex and occipital bone
- Subperiosteal dissection reflects neck muscles (sternocleidomastoid, splenius capitis, semispinalis) inferiorly
B. CRANIOTOMY
Osteoplastic (bone-flap) craniotomy (preferred for acoustic neuroma):
- Burr hole placed at asterion (landmark for junction of transverse and sigmoid sinuses)
- Additional burr holes placed; bone flap elevated (~3×4 cm) using craniotome
- Flap preserved in saline / antibiotic solution for replacement at closure
Osteoclastic craniectomy (MVD, smaller tumors):
- Bone removed piecemeal with Kerrison rongeurs / drill
- Posterior boundary: 1–2 cm posterior to sigmoid sinus
- Superior boundary: transverse sinus
- Size: approximately 3×3 cm
- Sigmoid sinus identified anteriorly — key landmark
- Transverse sinus identified superiorly
Optional transmastoid skeletonization:
- Mastoidectomy → skeletonize sigmoid sinus
- Allows anterior retraction of sigmoid sinus → increases CPA exposure
- Identifies posterior semicircular canal → guides drilling of posterior IAC lip
- Fig. 179.30 — Cummings (p. 3448): Mastoidectomy in conjunction with retrosigmoid exposure permits anterior retraction of sigmoid sinus
C. DURAL OPENING
- C-shaped or curvilinear incision in posterior fossa dura, posterior to sigmoid sinus
- Incise carefully — avoid injury to vessels adherent to dura
- Dural flap tented with traction sutures → sinus retracted anteriorly
- Increases lateral working angle substantially
D. CSF DRAINAGE — CRITICAL STEP
- Slow, controlled CSF drainage from CPA cistern
- Inadequate drainage → cerebellum herniates through dural incision → cerebellar contusion/necrosis/hemorrhage
- CSF also drained from cisterna magna / foramen magnum region
- Lumbar drain can be placed preoperatively for large tumors
E. CEREBELLAR RETRACTION
- Cottonoid strips (with rubber glove backing) placed over cerebellar surface
- Slow, gentle retraction over 5–10 minutes
- Once adequate CSF drained, no external retractor needed — cerebellum falls away
- Exposes: flocculus, choroid plexus, CN VII–VIII bundle
- Key view: posterior fossa face of temporal bone + porus acusticus
F. TUMOR SURGERY — ACOUSTIC NEUROMA
- Identify CN VII and VIII at porus acusticus (medial)
- Debulk tumor internally (ultrasonic aspirator / bipolar + scissors) for large tumors
- Identify facial nerve at brainstem — critical before dissection
- Remove posterior lip of IAC with diamond burs (under irrigation)
- Lateral limit = posterior semicircular canal
- Previously exposed mastoid dura guides surgeon to canal location
- Dissect tumor from facial nerve — from CPA toward porus (medial → lateral)
- Cochlear nerve preservation for hearing conservation — avoid blood supply to IAC
- Fundus visualization: mirrors + endoscope (30°/70° rod-lens) if needed
- Cannot use Bill's bar (translabyrinthine advantage) — relies entirely on nerve monitor for lateral IAC
G. CLOSURE
- IAC packed with abdominal fat graft — prevents CSF leak
- Mastoid air cells waxed / obliterated with fat
- Dura closed in watertight fashion (4-0 braided nylon)
- Bone flap replaced and fixed with microplates/titanium or cranioplasty material (reduces post-op headache)
- Muscles, fascia, subcutaneous tissue, skin — layered closure
- Mastoid compressive dressing applied
8. INTRAOPERATIVE MONITORING
| Monitor | Purpose |
|---|---|
| Continuous facial nerve EMG | CN VII identification and preservation |
| BAER (intraoperative) | Cochlear nerve / hearing preservation |
| Antidromic facial nerve potentials | Direct monitoring; reported by Colletti & Fiorino in retrosigmoid approach (Cummings, p. 4313) |
| SSEP | Brainstem/cord integrity |
| ABR | Continuous hearing status |
| Doppler | Air embolism detection (sitting position) |
9. INTRAOPERATIVE IMAGES
Fig. 173.9 — Retrosigmoid craniotomy (Cummings Otolaryngology, p. 3314):
Retrosigmoid craniotomy: Skin flap reflected anteriorly, exposing the mastoid and cerebellar cortical bone. Craniotomy (~4×4 cm) exposes the sigmoid sinus anteriorly, transverse sinus superiorly, and the cerebellum. — Cummings Otolaryngology Head and Neck Surgery
Standard vs. Extended Retrosigmoid Approach — Surgical Corridor Comparison:
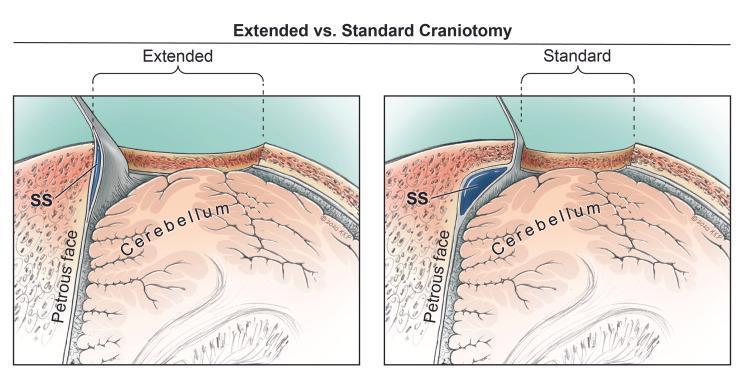
Superior axial view: Standard vs. Extended Retrosigmoid (RS) craniotomy. In the extended approach, skeletonization and anterior retraction of the sigmoid sinus (SS) significantly widens the surgical corridor to the cerebellopontine angle (petrous face).
Step-by-step Retrosigmoid Craniotomy (Intraoperative series):
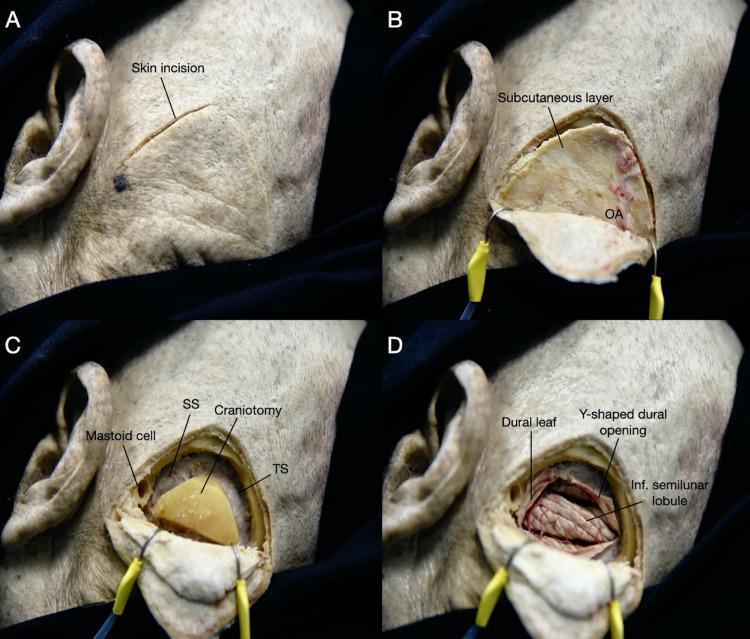
(A) Post-auricular incision; (B) Tissue dissection showing occipital artery; (C) Bone removal exposing sigmoid and transverse sinus margins; (D) Dura opened in Y-shaped fashion exposing posterolateral cerebellum.
Intraoperative view showing sigmoid sinus after bone removal:
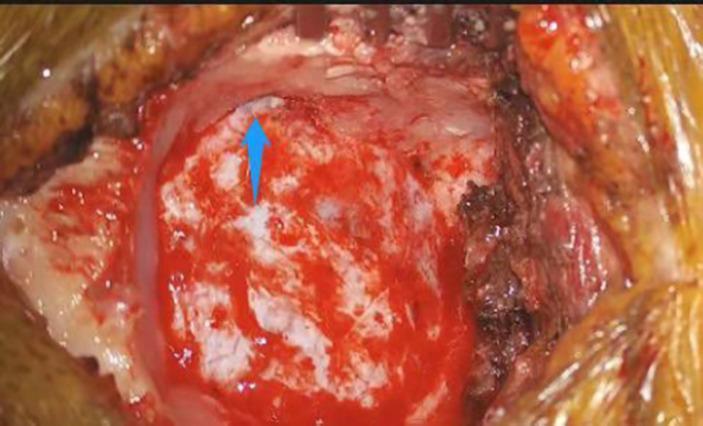
Intraoperative retrosigmoid craniotomy: Blue arrow marks the exposed sigmoid sinus — the critical anterior anatomical landmark defining the anterior boundary of this approach.
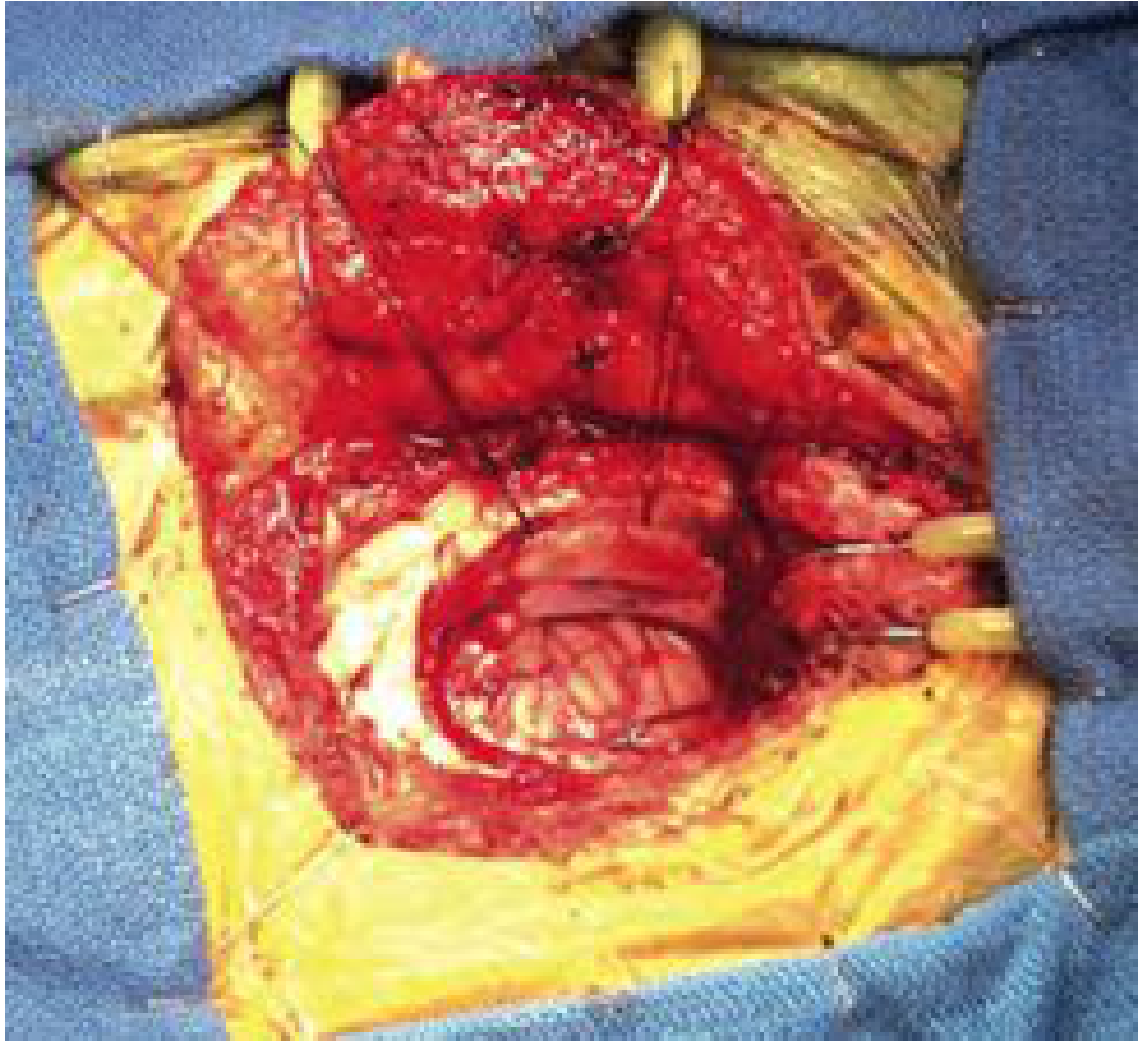
CPA Exposure with Cranial Nerve Identification:
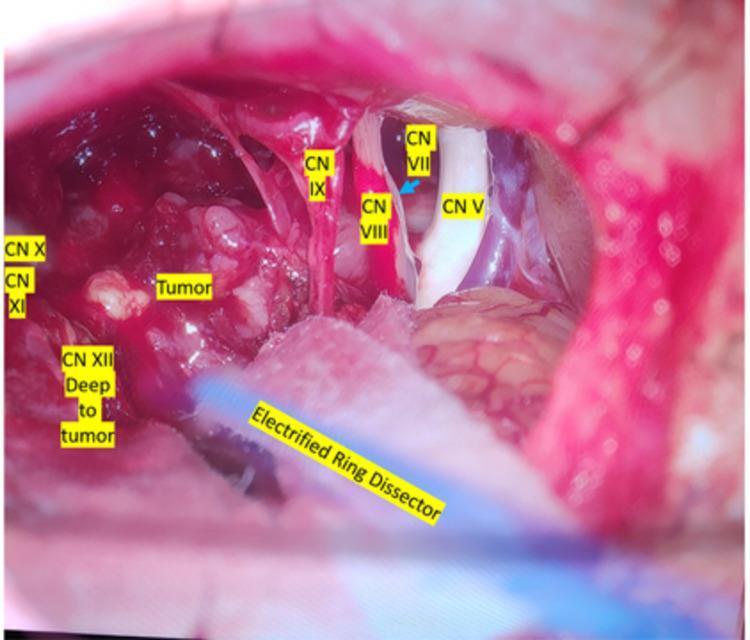
Left CPA exposure through retrosigmoid approach: CN V (superior), CN VII–VIII bundle, CN IX–XI (inferior). Electrified ring dissector used for intraoperative nerve monitoring during tumor dissection.
10. SELECTION OF SURGICAL APPROACH — DECISION FLOWCHART
ACOUSTIC NEUROMA / CPA LESION
│
┌─────────────┴─────────────┐
│ │
HEARING SERVICEABLE? HEARING NOT SERVICEABLE
(PTA ≤50 dB, SDS ≥50%) │
│ ▼
YES │ TRANSLABYRINTHINE APPROACH
│
┌───────┴────────┐
│ │
TUMOR SIZE TUMOR SIZE
≤1.5 cm (intra- >2 cm, CPA component
canalicular/small)
│ │
▼ ▼
MIDDLE FOSSA RETROSIGMOID (SUBOCCIPITAL)
APPROACH APPROACH
(fundus visible, (panoramic CPA exposure)
young patient)
RETROSIGMOID APPROACH — Further decision:
│
┌───────────────┴──────────────┐
│ │
TUMOR NOT AT FUNDUS TUMOR AT FUNDUS
│ │
▼ ▼
HEARING PRESERVATION HEARING PRESERVATION
ATTEMPTED UNLIKELY / TRANSLABYRINTHINE
(30–65% success rate) PREFERRED
(Based on Cummings Otolaryngology, p. 3451 — Selection of Surgical Approach)
11. POSTOPERATIVE MANAGEMENT
- Immediate: ICU/HDU monitoring for 24 hours
- Neurological observation: hourly GCS, cranial nerve assessment
- Wound: mastoid compressive dressing for 24–48 hours
- CSF leak prevention: head-of-bed elevation 30°, avoid Valsalva
- Medications: steroids (dexamethasone), antiemetics, analgesics
- Hearing: ABR tested on day 1 post-op
- Facial nerve: House-Brackmann grading documented
- Early mobilization: Day 1–2 post-op
- Vestibular rehabilitation: started early for balance compensation
12. COMPLICATIONS
Intraoperative:
| Complication | Prevention |
|---|---|
| Sigmoid/transverse sinus injury | Careful bone removal; bipolar cautery ready |
| Cerebellar contusion | Slow CSF drainage; gentle retraction over ≥5 min |
| Air embolism | Avoid sitting position; Doppler monitoring |
| CN VII/VIII injury | Continuous nerve monitoring |
| AICA injury | Careful vascular dissection |
Postoperative:
| Complication | Incidence | Management |
|---|---|---|
| CSF leak (most common) | 5–10% | Fat graft, lumbar drain, re-exploration |
| Meningitis (aseptic/bacterial) | 2–5% | Antibiotics; related to intradural bone dust |
| Cerebellar haematoma | <1% | Re-exploration |
| Facial palsy | Variable (10–30%) | Nerve monitoring; rehabilitation |
| Hearing loss | If attempted preservation: 35–70% failure | Patient counseling |
| Severe post-op headaches | ~10% | Bone flap replacement; avoid muscle-dura adhesion |
| Hydrocephalus | 1–3% | VP shunt |
| Wound infection | 1–2% | Antibiotics |
Note on postoperative headaches (Cummings, p. 3449): A 10% incidence of severe postoperative headaches is reported. This is related to:
- Intradural bone dust from drilling the posterior IAC lip
- Scar and muscle adhesion to dura
Replacing the bone flap with microplates or cranioplasty with synthetic materials has significantly reduced this complication.
13. RESULTS & OUTCOMES
Hearing Preservation:
- Success rate: 30–65% depending on selection criteria (Cummings, p. 3449)
- Best results: tumor <1.5 cm, limited IAC involvement, not reaching fundus
- Cochlear implantation is an option if hearing conservation fails post-operatively
Facial Nerve Preservation:
- Comparable rates to translabyrinthine approach
- Some centers report slightly better rates with translabyrinthine (due to direct Bill's bar identification)
- Modern series (with monitoring): >95% anatomical preservation for tumors <2 cm
Tumor Control:
- Gross total resection: >95% for acoustic neuromas <2 cm
- Recurrence: ~2–3% at 5 years
14. COMPARISON: THREE STANDARD CPA APPROACHES
┌─────────────────────────────────────────────────┐
│ CPA TUMOR SURGERY — APPROACH COMPARISON │
└─────────────────────────────────────────────────┘
FEATURE │ RETROSIGMOID │ TRANSLABYRINTHINE│ MIDDLE FOSSA
─────────────────┼─────────────────┼──────────────────┼─────────────
Hearing │ Preserved │ Always lost │ Best preserved
Preservation │ (30–65%) │ │
─────────────────┼─────────────────┼──────────────────┼─────────────
IAC fundus │ ❌ Indirect │ ✅ Direct │ ✅ Direct
visualization │ │ │
─────────────────┼─────────────────┼──────────────────┼─────────────
CPA exposure │ Widest/Panoramic│ Wide │ Limited (<1cm)
─────────────────┼─────────────────┼──────────────────┼─────────────
Tumour size │ Any size │ Any size │ Intracanalicular
─────────────────┼─────────────────┼──────────────────┼─────────────
Cerebellar │ Required │ Minimal │ Not needed
retraction │ │ │
─────────────────┼─────────────────┼──────────────────┼─────────────
Facial nerve │ Brainstem first │ Brainstem + fundus│ Fundus first
identification │ │ │
─────────────────┼─────────────────┼──────────────────┼─────────────
Post-op headache │ 10% │ Rare │ Rare
─────────────────┼─────────────────┼──────────────────┼─────────────
Best for │ CPA tumors with │ Large tumors / │ Small intra-
│ serviceable │ non-serviceable │ canalicular
│ hearing │ hearing │ in young pts
15. RECENT ADVANCES
1. Endoscope-Assisted Retrosigmoid Approach
- Keyhole retrosigmoid craniotomy + rigid endoscope (30°/70°)
- Visualizes fundus of IAC without drilling posterior semicircular canal
- Reduces the principal limitation of this approach (indirect fundus visualization)
- Used for: MVD, small intracanalicular tumors, cholesteatoma of CPA
- Fully endoscopic retrosigmoid approach reported for acoustic neuromas
2. Robotic-Assisted Surgery
- Da Vinci system adaptations for CPA — early experimental phase
- Theoretical advantage: tremor-free dissection in narrow corridor
3. Intraoperative MRI
- Real-time assessment of tumor residual during resection
- Alters surgical decisions in ~20–30% of cases
- Increases gross total resection rates
4. Intraoperative CT with Navigation
- Neuronavigation / image guidance integrated with retrosigmoid approach
- Precise IAC drilling without damaging posterior SCC
- Reduces risk of CSF fistula
5. Enhanced Neuromonitoring
- Continuous transcranial motor evoked potentials (MEP)
- Antidromic facial nerve action potentials (Colletti & Fiorino — Cummings, p. 4313)
- Intraoperative ABR with automated real-time analysis
6. Hearing Preservation Modifications
- Arriaga & Gorum: posterior semicircular canal resection with retrosigmoid approach for enhanced lateral IAC exposure while preserving hearing (reported 2/3 success rate)
- Cochlear implantation post-operatively when hearing conservation fails (combined with retrosigmoid dissection)
7. Modified Retrosigmoid Approaches
- Retrosigmoid-transjugular approach: access to jugular foramen tumors
- Retrosigmoid-transtentorial approach: access to upper CPA + Meckel's cave
- Far-lateral retrosigmoid: access to anterior foramen magnum + lower CN pathology
8. Stereotactic Radiosurgery vs. Surgery
- Gamma Knife / CyberKnife: alternative for tumors <3 cm
- Current consensus: microsurgical retrosigmoid for young patients, good hearing, growing tumors; radiosurgery for elderly, small stable tumors
- Wait-and-scan: for small incidentally found tumors
9. Minimally Invasive / Keyhole Techniques
- Small (2.5 cm) retrosigmoid craniotomy with endoscope
- Equivalent tumor control with less morbidity in selected patients
- Shorter hospital stay, reduced blood loss
16. IMPORTANT POINTS FOR EXAM (RGUHS)
- Dandy's approach = original suboccipital = modern retrosigmoid
- Key landmark: Sigmoid sinus (anterior) + Transverse sinus (superior)
- Asterion = junction of lambdoid, occipitomastoid, parietomastoid sutures = burr hole landmark
- Critical step: CSF drainage before cerebellar retraction
- Hearing preservation rate: 30–65%
- Post-op headache: 10% — reduced by bone flap replacement
- Limitation: Cannot directly visualize IAC fundus (Bill's bar inaccessible)
- MVD (Jannetta's procedure for trigeminal neuralgia): exclusively retrosigmoid approach
- Bone flap vs. craniectomy: Osteoplastic bone flap reduces post-op headache incidence
- Fat graft: mandatory to obliterate IAC and mastoid air cells — prevents CSF leak
REFERENCES
- Cummings Otolaryngology Head and Neck Surgery (7th Ed.) — Chapter 173 (Facial Nerve Surgery) & Chapter 179 (Acoustic Neuroma / CPA Surgery), pp. 3314, 3448–3452
- K.J. Lee's Essential Otolaryngology (11th Ed.) — Skull Base Surgery chapter
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery (8th Ed.) — CPA approaches
- Dhingra's Diseases of Ear, Nose and Throat — Surgical approaches to temporal bone
- Hazarika's Ear Nose Throat — Retrosigmoid (suboccipital) approach
- Zakir Hussain's ENT — Posterior fossa approaches
- Stell and Maran's Head and Neck Surgery — Skull base surgery
- Colletti V, Fiorino F — Antidromic facial nerve monitoring in retrosigmoid approach for acoustic neuroma (Cummings, p. 4313)
- Arriaga MA, Gorum M — Posterior semicircular canal resection for enhanced retrosigmoid approach with hearing preservation (Cummings, p. 3452)
- Jannetta PJ — Microvascular decompression via retrosigmoid approach
This comprehensive answer covers anatomy, indications, step-by-step technique, monitoring, complications, recent advances, and comparison tables, suitable for a 50-mark RGUHS long-answer question.
This is a shared conversation. Sign in to Orris to start your own chat.