Endometriosis
Reading File
Finding Sources
Searching PubMed
"endometriosis"[MeSH Terms] AND ("diagnosis" OR "management")
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content across pathology, surgical, and pharmacological textbooks. Let me compile the full answer.
Endometriosis
Definition
Endometriosis is the presence of endometrial glands and stroma outside the uterine cavity. It is a common chronic inflammatory condition affecting 5-10% of women of reproductive age and nearly 40-50% of women with infertility.
- Robbins & Kumar Basic Pathology, p. 689
- Bailey and Love's Short Practice of Surgery, p. 1602
Pathogenesis
The exact mechanism remains elusive. Four main theories are proposed:
| Theory | Mechanism |
|---|---|
| Regurgitation (Sampson's) | Retrograde menstruation causes endometrial tissue to implant at ectopic pelvic sites via the fallopian tubes - the most widely accepted theory |
| Benign metastasis | Endometrial tissue spreads to distant sites (lung, brain, bone) via blood/lymphatics |
| Metaplastic theory | Coelomic (mesothelial) epithelium undergoes metaplasia into endometrial tissue - explains embryological müllerian remnants |
| Stem/progenitor cell theory | Bone marrow stem cells differentiate into ectopic endometrial tissue |
Endometriotic implants are not simply misplaced cells - they are biologically distinct, exhibiting elevated:
- Prostaglandin E2 and COX-2 (inflammation)
- VEGF (angiogenesis)
- Matrix metalloproteinases (MMPs)
- Aromatase - producing excess local estrogen from androgens, reinforcing estrogen dependency

Fig. 17.9 - Pathogenesis of endometriosis (Robbins & Kumar Basic Pathology)
Classification / Types
Three main types exist:
- Superficial peritoneal endometriosis - small lesions on pelvic peritoneum
- Ovarian endometriosis (endometriomas) - "chocolate cysts" filled with thick dark fluid, reported in 17-44% of cases; densely adherent to peritoneum
- Deep infiltrating endometriosis (DIE) - defined as endometrial-like tissue >5 mm beneath the peritoneum, involving uterosacral ligaments, vagina, bowel, bladder, or ureters; highest risk of malignant transformation
The ASRM classification system (I-IV: minimal, mild, moderate, severe) is commonly used operatively, though it has poor correlation with symptom severity.
Sites of Involvement
Common (pelvic):
- Ovaries (most common)
- Uterosacral ligaments
- Pouch of Douglas
- Fallopian tubes
- Pelvic peritoneum
- Bladder/ureters
Rare (extra-pelvic):
- Diaphragm (see laparoscopic image below)
- Lungs - causing catamenial haemoptysis or pneumothorax
- Bowel/rectosigmoid
- Periumbilical tissues and laparotomy scars
- Brain, bone (via haematogenous spread)
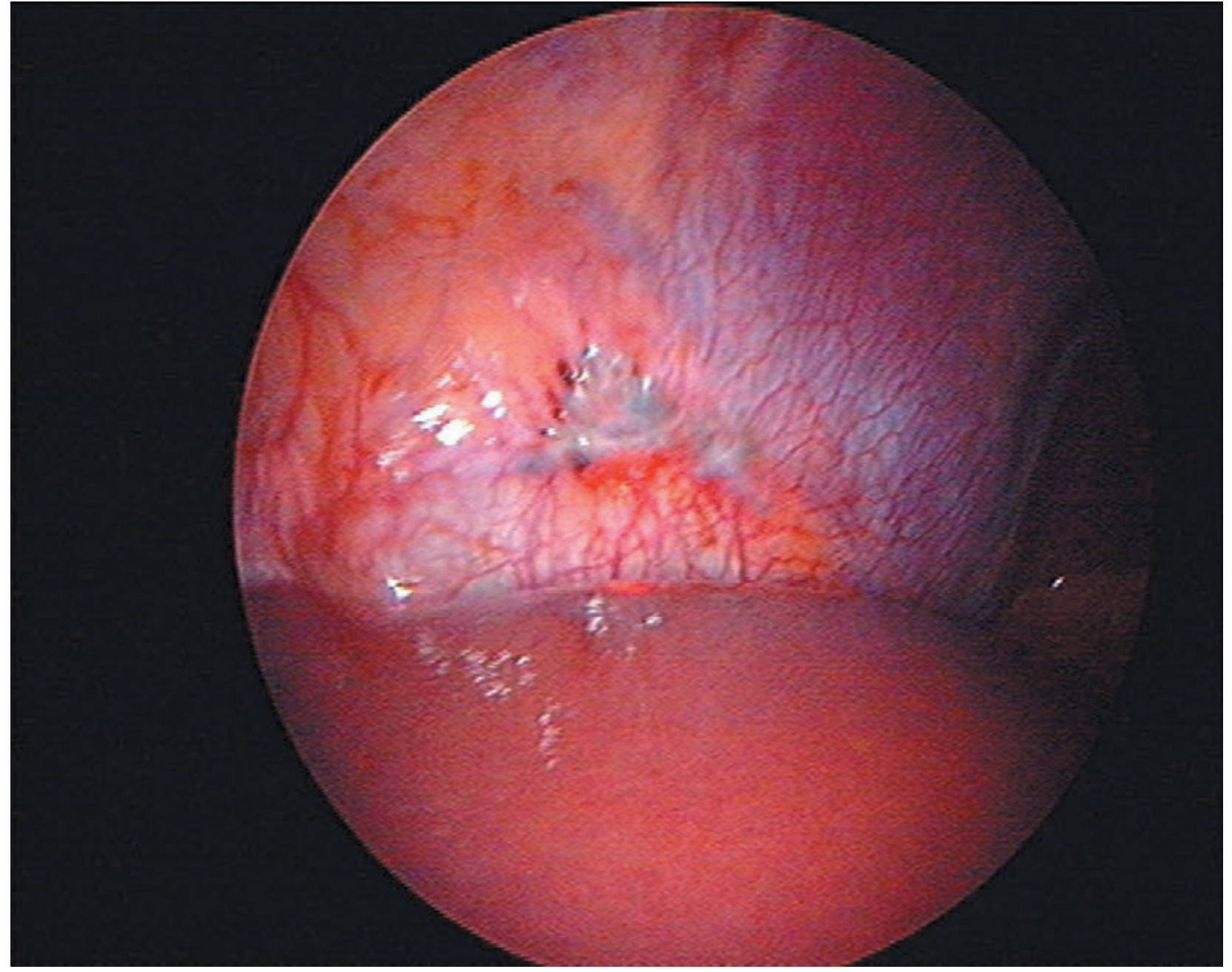
Fig. 87.11 - Endometriosis on the peritoneal surface of the diaphragm (Bailey & Love's)
Morphology
Grossly, lesions appear as:
- "Powder burn" / "gunshot" lesions - black, dark brown, or blue-black puckered nodules containing old haemorrhage with surrounding fibrosis (classic appearance)
- Atypical/subtle lesions - red flame-like, vesicular, polypoid, or haemorrhagic implants; serous/clear vesicles
- White plaques or scarring, yellow-brown peritoneal discoloration
- Endometriomas - large ovarian cysts containing thick "tar-like" fluid, due to cyclic bleeding into the cyst
Histologically: functioning endometrial glands + stroma undergo cyclic bleeding at ectopic sites, forming red-brown nodules (1-2 mm to 1-2 cm). Organisation of haemorrhage leads to fibrosis and adhesions that obliterate the pouch of Douglas and distort pelvic anatomy.
Clinical Features
Symptoms arise from cyclical bleeding at ectopic sites and inflammation. A significant proportion of women are asymptomatic.
Pain symptoms (most common):
- Dysmenorrhoea (cyclic pelvic pain with menstruation)
- Deep dyspareunia (pain during intercourse)
- Dyschezia (pain on defecation)
- Dysuria / haematuria
- Chronic non-cyclical pelvic pain
Other symptoms:
- Infertility (present in up to 50% of affected women)
- Fatigue
- Rectal bleeding (haematochezia) - if bowel involvement
- Cyclic haemoptysis / pneumothorax - if pulmonary involvement
Examination findings suggestive of endometriosis:
- Pelvic tenderness
- Fixed retroverted uterus
- Tender uterosacral ligaments
- Enlarged ovaries
- Deeply infiltrating nodules in the pouch of Douglas
- Visible blue-domed cystic lesions in the posterior fornix (vaginal DIE)
Note: examination may be entirely normal.
Diagnosis
| Method | Role |
|---|---|
| Laparoscopy + biopsy | Gold standard - direct visualisation and histological confirmation |
| Transvaginal ultrasound (TVUS) | Reliably detects endometriomas and severe/deep pelvic disease; misses superficial peritoneal lesions |
| Transrectal ultrasound | Useful for bowel and recto-vaginal endometriosis |
| MRI pelvis | Detects haemosiderin deposits; useful for DIE mapping, surgical planning |
| Sigmoidoscopy | Assesses bowel involvement; measures distance of rectal lesion from anal verge (critical for surgical planning) |
| CA-125 | Non-specific; may be elevated but not diagnostic |
A clinical diagnosis can be made empirically in women with typical symptoms, and medical treatment commenced without histological confirmation - laparoscopy is reserved for cases not responding to initial management or where infertility is a concern.
- Bailey and Love's Short Practice of Surgery, p. 1603
Management
1. Conservative (watchful waiting)
Appropriate for asymptomatic or mildly symptomatic women not seeking fertility.
2. Medical Management
All hormonal therapies aim to suppress ovarian estrogen production, causing endometrial atrophy at ectopic sites. They treat symptoms but do not permanently cure the disease.
| Drug | Mechanism | Notes |
|---|---|---|
| Combined oral contraceptive pill (COCP) | Suppresses gonadotropins → inhibits estrogen biosynthesis | First-line; well-tolerated |
| Progestogens (medroxyprogesterone, dienogest) | Decidualization of ectopic tissue, anti-proliferative | Effective for pain; dienogest widely used |
| Levonorgestrel IUS (Mirena) | Local progestogenic effect | Used off-label; good for menorrhagia + pain |
| GnRH agonists (leuprolide, goserelin, nafarelin) | Downregulate pituitary GnRH receptors → medical castration | "Add-back" therapy (low-dose oestrogen or norethindrone 5 mg) required if >6 months, to limit hypoestrogenic effects and bone loss |
| GnRH antagonist - Elagolix | Oral receptor antagonist; suppresses gonadotropins | Effective for dysmenorrhoea and pelvic pain; risk of hot flashes, dyslipidaemia, bone mineral density reduction |
| Danazol | Synthetic androgen; inhibits pituitary-ovarian axis via feedback | FDA-approved but rarely used - significant androgenic side effects (hirsutism, hepatotoxicity) |
| NSAIDs | Prostaglandin inhibition | Simple analgesia for pain control |
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 303-307
3. Surgical Management
Conservative surgery (laparoscopic):
- Ablation or excision of endometriotic lesions
- Adhesiolysis to restore pelvic anatomy
- Cystectomy for endometriomas
- Aim: remove ectopic tissue while preserving fertility
- Bowel integrity testing (methylene blue / air insufflation) should be performed if bowel dissection is needed
- Ureteral stents should be considered in bladder/trigonal endometriosis
Definitive surgery:
- Hysterectomy + bilateral salpingo-oophorectomy (BSO) + total excision of endometriotic disease - offers best chance of cure; reserved for women who have completed their family
Surgical risks include bowel, bladder, and ureteric injury (~2 in 1000 women); risk is higher in DIE, repeat operations, and cases involving rectal lesions close to the anal verge (5-8 cm) where anastomotic leak risk is elevated.
Endometriosis and Infertility
- Infertility present in 25-40% of infertile women
- Mechanisms include: tubal involvement, impaired oocyte maturation, pelvic adhesions, altered peritoneal environment (elevated inflammatory cytokines), and possibly impaired implantation
- Surgical correction of anatomical distortion may improve natural fertility; IVF is the primary option for tubal-factor infertility
Malignant Transformation
- Overall risk is low
- Primarily associated with deep infiltrating endometriosis and ovarian endometriomas
- Most common histological type arising in endometriosis: endometrioid and clear cell carcinomas of the ovary
Key Points Summary
- Common (5-10% of reproductive-age women), estrogen-dependent, chronic inflammatory condition
- Leading pathogenic theory: retrograde menstruation
- Classic presentation: dysmenorrhoea + dyspareunia + infertility
- Gold standard diagnosis: laparoscopy with biopsy
- Medical treatment suppresses ovarian function; surgery excises disease
- Definitive cure: hysterectomy + BSO in women who have completed childbearing
- Recurrence is common after conservative treatment
Sources:
- Robbins & Kumar Basic Pathology (9780323790185), p. 689
- Bailey and Love's Short Practice of Surgery, 28th Ed. (9780367548117), pp. 1602-1604
- Goodman & Gilman's The Pharmacological Basis of Therapeutics (9781264258079), pp. 303-307
Recent evidence note: A 2025 systematic review (PMID 39373298) highlights that the median diagnostic delay for endometriosis remains 4-11 years globally, driven by symptom normalisation and overlap with other conditions. A 2026 meta-analysis (PMID 40705433) demonstrates significant benefit of physiotherapy for endometriosis-associated pelvic pain - an emerging non-pharmacological option not yet reflected in older textbooks.
This is a shared conversation. Sign in to Orris to start your own chat.