Noise Induced hearing loss in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
I now have comprehensive content. Let me compile the full 50-mark answer.
NOISE-INDUCED HEARING LOSS (NIHL)
A Comprehensive Answer for 50 Marks — RGUHS ENT Examination
1. DEFINITION AND EPIDEMIOLOGY
Noise-induced hearing loss (NIHL) is a permanent sensorineural hearing loss caused by repeated or sustained exposure to excessive levels of sound, resulting in irreversible damage to the cochlear hair cells.
- NIHL is second only to age-related hearing loss (presbycusis) as the most prevalent form of acquired hearing loss globally (Cummings, 7th ed., Ch. 154)
- Approximately 22 million workers in the USA alone are exposed to hazardous occupational noise
- Historically called "boilermaker's deafness" in the early 20th century
- Annual US disability payments for NIHL and tinnitus in military veterans exceed $1.1 billion
- NIHL is entirely preventable — this is its most clinically significant characteristic
2. PHYSICS OF SOUND — MEASUREMENT OF NOISE
Sound intensity is measured in decibels (dB). Three weighting scales are used:
| Scale | Use | Comments |
|---|---|---|
| dB(A) | Occupational monitoring | Discounts low-frequency; mimics human hearing at 40 dB |
| dB(C) | High-level impulse noise | Flatter curve; less discounting of low frequencies |
| dB(Z) | Unweighted | True total energy, 10–20,000 Hz |
Temporal patterns of noise:
- Continuous — steady-state (most occupational noise)
- Fluctuating — varies in level over time
- Intermittent — alternating periods of noise and quiet
- Impulsive — sudden explosive release of energy (gunfire, blasts)
- Impact — caused by collision of two objects (hammer, press)
3. FACTORS DETERMINING COCHLEAR DAMAGE
Four principal factors govern the effect of noise on the cochlea (KJ Lee's Essential Otolaryngology):
- Sound pressure level (dB SPL)
- Spectral composition (frequency content)
- Time distribution of exposure during the working day
- Cumulative noise exposure over days, weeks, years
4. OSHA PERMISSIBLE NOISE EXPOSURE LIMITS
(KJ Lee's Essential Otolaryngology, Table 14-13)
| Duration (hours/day) | Permissible SPL (dBA) |
|---|---|
| 8 | 90 |
| 6 | 92 |
| 4 | 95 |
| 2 | 100 |
| 1 | 105 |
| 0.5 | 110 |
| ≤0.25 | 115 |
Key rule: For every 5 dB increase, exposure time is halved (OSHA "5 dB exchange rate"). WHO/NIOSH uses a stricter 3 dB exchange rate.
Safe threshold: >85 dBA for 8 hours/day is considered hazardous. Single exposures >140 dB can cause immediate permanent damage (acoustic trauma).
5. CLASSIFICATION OF NIHL
┌──────────────────────────────────────────────────┐
│ NOISE-INDUCED HEARING LOSS │
└──────────────┬───────────────────────────────────┘
│
┌──────────┴──────────┐
│ │
▼ ▼
┌──────────────┐ ┌───────────────────┐
│ TEMPORARY │ │ PERMANENT │
│ THRESHOLD │ │ THRESHOLD SHIFT │
│ SHIFT (TTS) │ │ (PTS) │
└──────┬───────┘ └────────┬──────────┘
│ │
▼ ▼
Recovers within Does NOT recover
minutes to 48 hrs — irreversible
│ │
Reversible damage ┌─────┴──────────────┐
to stereocilia, │ │
pillar cells, ▼ ▼
auditory nerve NIHL (chronic ACOUSTIC TRAUMA
dendrites repeated TTS) (single intense
exposure, e.g.
explosion)
5.1 Temporary Threshold Shift (TTS)
- Reversible SNHL from moderately intense exposure (e.g., concert, power tools)
- Accompanied by tinnitus, loudness recruitment, muffled sounds, diplacusis
- Recovery: minutes to 48 hours after exposure ends
- Pathology: reversible buckling of pillar cell bodies, reversible stereocilia damage, excitotoxic swelling of auditory nerve dendrites below IHCs
5.2 Permanent Threshold Shift (PTS) — NIHL
Diagnostic criteria (Cummings, Ch. 154):
- Permanent SNHL with damage principally to cochlear hair cells (primarily OHCs)
- History of long-term exposure to >85 dBA for 8 h/day
- Gradual bilateral symmetrical loss — begins at 3–6 kHz, maximal at 4 kHz
- Tinnitus is a common accompaniment
- No other etiology explains the loss
5.3 Acoustic Trauma
- Single brief exposure to an extremely intense sound (explosion, blast, gunshot)
- Sudden, often painful loss of hearing
- Can be unilateral or asymmetric
- May include tympanic membrane perforation (adding a conductive component)
- Military personnel and hunters are commonly affected
6. PATHOPHYSIOLOGY — CELLULAR AND MOLECULAR MECHANISMS
NOISE EXPOSURE
│
▼
Mechanical vibration of basilar membrane
│
▼
Excessive displacement of organ of Corti
│
├──────────────────────────────────────┐
▼ ▼
MECHANICAL INJURY METABOLIC / OXIDATIVE INJURY
(Immediate) (Delayed — hours to days)
│ │
▼ ▼
Disruption of tip links Excessive glutamate release
Stereocilia fusion/fracture → Excitotoxicity at IHC synapses
Outer hair cell loss │
(OHCs most vulnerable ▼
— basal turn first) Formation of Reactive Oxygen
│ Species (ROS) and free radicals
▼ │
Disruption of endocochlear ▼
potential (K⁺ cycle collapse) Mitochondrial dysfunction
│
▼
Apoptotic cell death cascade
(delayed, days-weeks post exposure)
│
▼
PERMANENT HAIR CELL LOSS
(OHC > IHC; basal > apical)
Key molecular players (Cummings, Ch. 154 — Recent Advances):
- Reactive Oxygen Species (ROS): Superoxide, hydroxyl radicals generated during and after noise
- Glutamate excitotoxicity: Overstimulation of AMPA/NMDA receptors on Type I afferents below IHCs → acute dendritic swelling → "cochlear synaptopathy"
- Cochlear synaptopathy (Hidden Hearing Loss): Selective loss of cochlear nerve synapses at IHCs without hair cell loss — normal audiogram but impaired speech-in-noise perception (Kujawa & Liberman, 2009)
- Atoh1 (Math1): Transcription factor essential for hair cell differentiation — target for gene therapy
- Intrinsic antioxidant defenses: Superoxide dismutase (SOD), catalase (CAT), glutathione peroxidase — genetic variants in CAT gene associated with increased NIHL susceptibility
7. ANATOMICAL BASIS OF THE 4 kHz NOTCH
The external auditory canal resonance amplifies sounds in the 2–5 kHz range by approximately 10–15 dB. This means:
- The cochlear region responding to 3–6 kHz (specifically the basal turn, ~10 mm from the stapes) receives disproportionately more energy during noise exposure
- OHCs in this region are the first to be damaged
- Result: the characteristic 4 kHz notch on audiogram — maximal hearing loss at 4 kHz with relative sparing at adjacent frequencies (Cummings, Ch. 154)
- In hunters/shooters: asymmetric 4 kHz notch worse in the ear opposite the gun-firing shoulder (KJ Lee)
8. AUDIOGRAM PATTERNS
Classic 4 kHz Notch (Early NIHL):
AUDIOGRAM — EARLY NIHL
Frequency: 250 500 1K 2K 3K 4K 6K 8K
─────────────────────────────────────────
0
10
20 ○────○────○────○
30 \
40 \
50 ╲ ← 4 kHz NOTCH
60 ╲__/
70 Recovery at 8K
Fig. 152.3 from Cummings — Predicted hearing thresholds (median and extreme values) after 20 and 40 years of occupational noise exposure at 90 dBA:
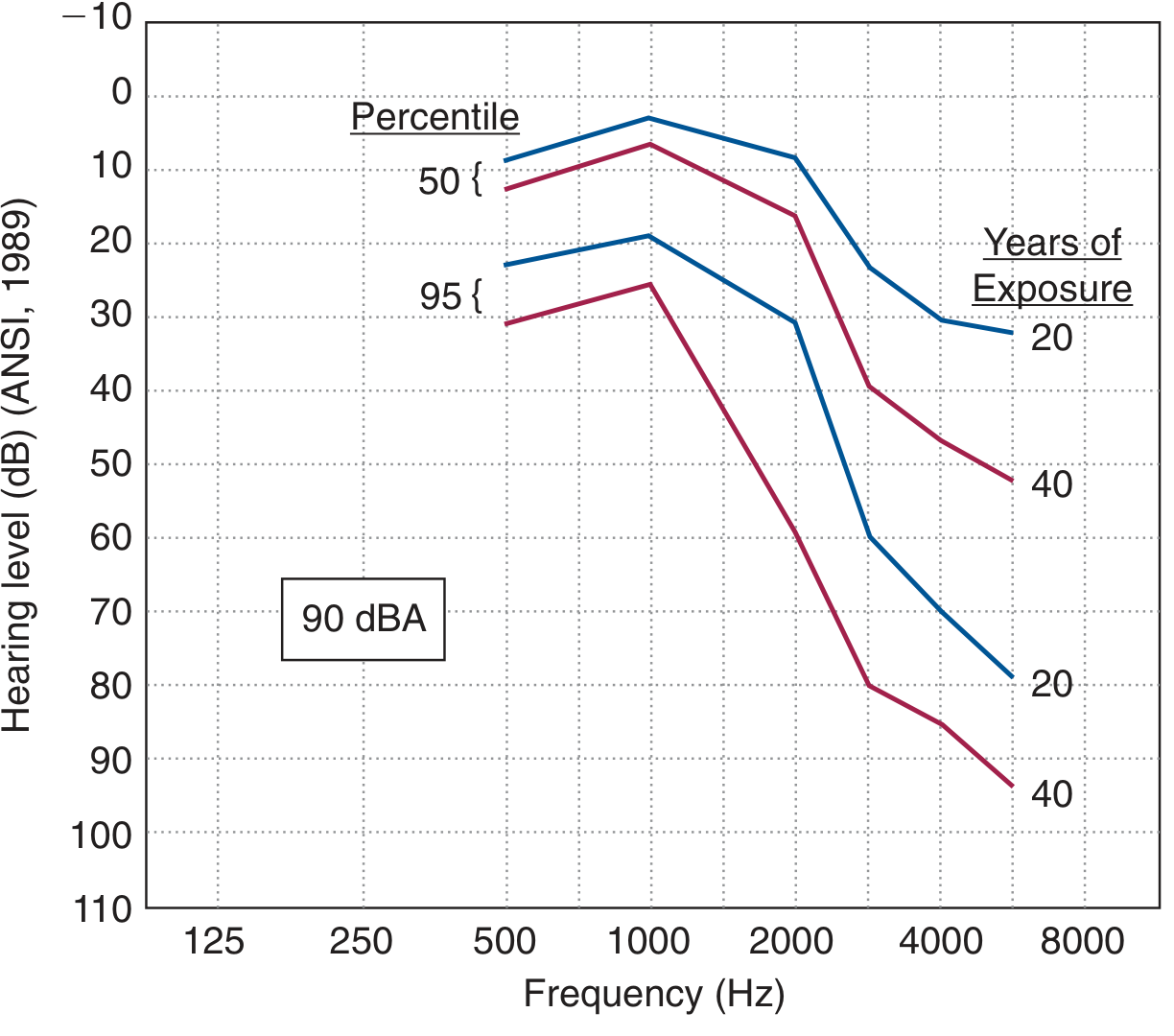
Predicted hearing thresholds (50th and 95th percentile) after 20 years (blue) and 40 years (red) of exposure to 90 dBA occupational noise — Cummings Otolaryngology, Ch. 152
Progression of NIHL (flowchart):
BRIEF / MODERATE NOISE EXPOSURE
│
▼
TTS at 3–6 kHz → Full recovery
│
[Repeated exposures]
│
▼
4 kHz notch appears (first 10–15 yrs = fastest progression)
│
[Continued exposure]
│
▼
Notch widens → 3, 4, 6 kHz all affected
│
[Long-term exposure]
│
▼
Lower frequencies (1, 2 kHz) involved
— Flat or downsloping audiogram
— Speech frequencies (500–2000 Hz) now affected
— Communicative disability begins
9. CHARACTERISTICS OF NIHL — DIAGNOSTIC CRITERIA
| Feature | Description |
|---|---|
| Type | Sensorineural hearing loss |
| Symmetry | Bilateral, symmetric (asymmetric in acoustic trauma) |
| Frequency | Begins at 3–6 kHz, max at 4 kHz |
| Progression | Fastest in first 10–15 yrs; slows thereafter |
| Severity | Almost never reaches profound loss from noise alone |
| Tinnitus | Very common accompaniment |
| Associated symptoms | Recruitment, diplacusis, difficulty hearing in noise |
| History | Long-term hazardous noise exposure |
10. SOURCES OF VARIABILITY IN NIHL
Environmental Factors:
- Level, duration, frequency content of noise
- Continuous vs. impulse noise (impulse more damaging per unit energy)
- Chemical co-exposures (ototoxic solvents — toluene, styrene, carbon disulfide — potentiate NIHL)
Individual / Genetic Susceptibility Factors:
- Conductive hearing loss is protective (acts like earplug)
- Absence of the acoustic reflex (mediated by stapedius) may increase susceptibility
- Genetic variants in CAT (catalase), SOD2, and other oxidative stress genes
- Increased susceptibility with age, pigmentation (melanin may be protective), pre-existing cochlear disease
11. DIAGNOSIS
Clinical Assessment:
- History: Occupational/recreational noise exposure history, tinnitus, difficulty hearing in noise
- Pure Tone Audiometry (PTA): Hallmark 4 kHz notch; bone and air conduction thresholds similar (pure SNHL)
- Speech Audiometry: Speech Discrimination Score (SDS) moderately reduced
- Tympanometry: Type A (normal middle ear)
- Acoustic Reflexes: Present unless severe loss
Diagnostic Flowchart:
Patient with hearing loss + noise exposure history
│
▼
Pure Tone Audiometry
│
┌──────┴────────┐
│ │
4 kHz notch? Flat/Downsloping?
(bilateral) (consider other
│ causes)
▼
Tympanometry — Type A (normal)
│
▼
Bone Conduction = Air Conduction
(confirming SNHL)
│
▼
OAE Testing (DPOAE)
(reduced/absent at 3–6 kHz)
│
▼
Rule out other causes:
— Presbycusis (affects ALL high freq)
— Ototoxicity (may include all frequencies)
— Sudden SNHL (unilateral, acute)
│
▼
CONFIRM NIHL DIAGNOSIS
Early Detection — Extended High-Frequency Audiometry & OAEs:
- Distortion Product OAEs (DPOAEs): Detect outer hair cell dysfunction before threshold changes appear on conventional audiogram
- The DPOAE graph from Cummings (Fig. 154.5) demonstrates genetic strain differences in cochlear recovery after noise — CBA mice show minimal DPOAE recovery vs. MOLF mice:
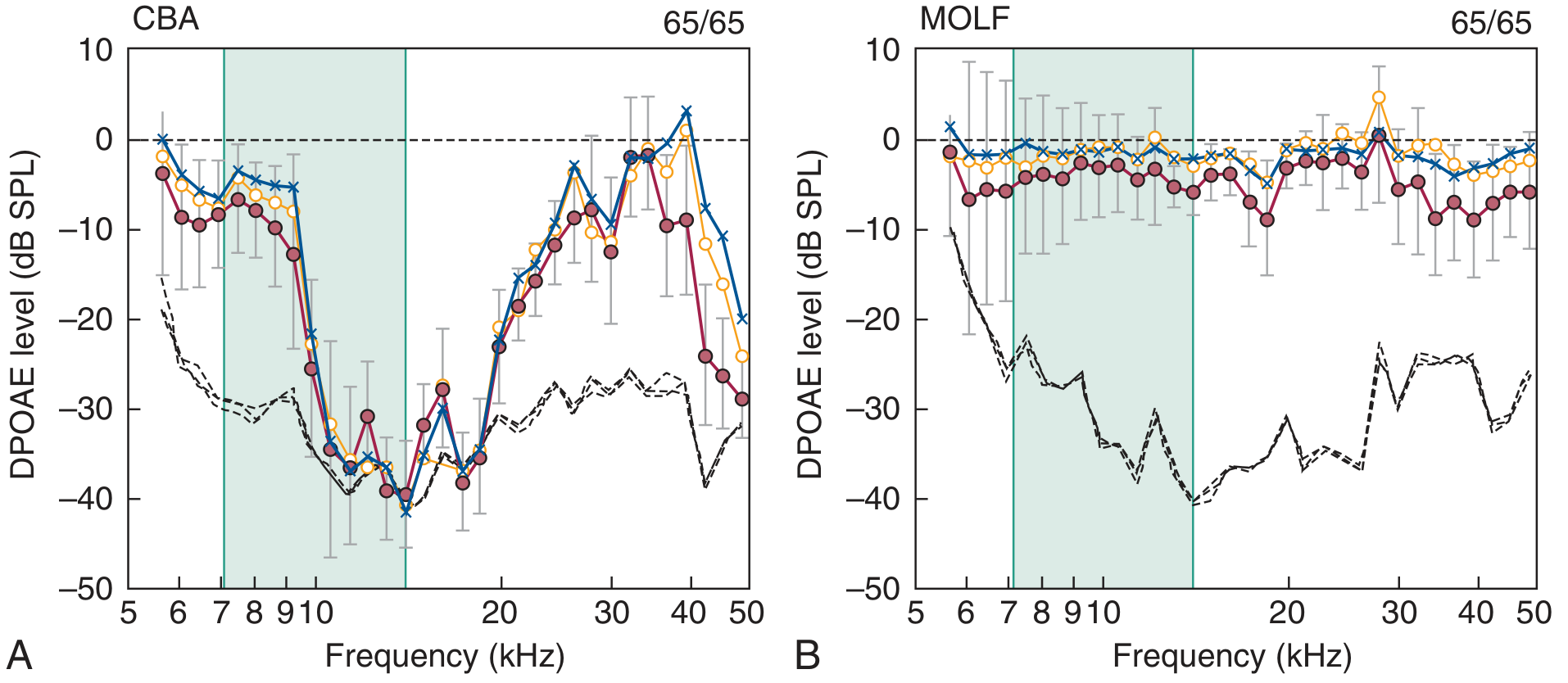
Preexposure minus postexposure DPOAE levels in CBA mice (A, minimal recovery) vs. MOLF mice (B, near-complete recovery) — demonstrating genetic susceptibility to NIHL — Cummings Ch. 154
12. DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Feature |
|---|---|
| Presbycusis | Bilateral, symmetric, all high frequencies, no noise notch |
| Ototoxicity | Drug history; may affect all frequencies |
| Sudden SNHL | Unilateral, acute onset |
| Ménière's disease | Episodic vertigo, fluctuating low-frequency loss |
| Acoustic neuroma | Unilateral, asymmetric |
13. HEARING CONSERVATION PROGRAM (HCP)
┌─────────────────────────────────────────────────┐
│ HEARING CONSERVATION PROGRAM │
│ (4 Components) │
└────────────┬────────────────────────────────────┘
│
┌────────┼───────────────────┐
▼ ▼ ▼ ▼
ASSESSMENT CONTROL PROTECTION MONITORING
│ │ │ │
Sound level Engineering Hearing Annual
meter & controls: protection audiometry
dosimetry — Barriers devices (pre-employ-
(measure — Noise (earplugs, ment +
noise dose) reduction earmuffs) periodic)
— Job rotation
(KJ Lee's Essential Otolaryngology)
Engineering Controls (Hierarchy):
- Elimination — remove noise source
- Substitution — quieter equipment
- Engineering controls — barriers, sound-absorbing materials, isolation
- Administrative controls — job rotation, reduced exposure time
- Personal Protective Equipment (PPE) — hearing protection devices (last resort)
Hearing Protection Devices:
- Earplugs (foam, pre-molded, custom): NRR 15–30 dB
- Earmuffs: NRR 20–30 dB
- Combined (plug + muff): additive 5 dB additional over highest rating
14. MANAGEMENT OF ESTABLISHED NIHL
ESTABLISHED NIHL
│
├─────────────────────────────────────────┐
▼ ▼
MEDICAL REHABILITATION
│ │
No curative ┌──────────┴───────────┐
treatment currently │ │
available Hearing aids Assistive
│ (digital frequency- listening
Counsel on: specific amplification) devices
— Avoid further noise (FM, infrared)
— Hearing protection │
— Tinnitus management Auditory therapy /
aural rehabilitation
Hearing Aids: Digital hearing aids provide frequency-specific amplification matched to the audiogram configuration — a major advantage over older analog devices for the notched audiogram of NIHL.
15. PREVENTION
Primary Prevention:
- Regulatory enforcement (OSHA limits: <90 dBA for 8 h)
- Hearing conservation programs in industry
- Public education (personal music devices, recreational noise)
- Pre-employment audiometry
Secondary Prevention:
- Annual audiometric surveillance
- Early identification of TTS (OAE screening)
- DPOAE monitoring in at-risk populations
Tertiary Prevention:
- Rehabilitation with hearing aids
- Cochlear implant (when profound loss)
16. RECENT ADVANCES (RGUHS Focus)
16.1 Cochlear Synaptopathy / "Hidden Hearing Loss"
- Kujawa & Liberman (2009): noise exposure causes selective loss of IHC synapses and spiral ganglion neurons without hair cell death
- Audiogram remains normal → the term "hidden hearing loss"
- Clinically manifests as impaired speech discrimination in noise despite normal pure-tone thresholds
- Detected by ABR wave I amplitude reduction and suprathreshold tests
16.2 Pharmacological Otoprotection (Cummings, Ch. 154)
Targeted at reducing ROS formation and excitotoxicity:
| Agent | Mechanism | Status |
|---|---|---|
| N-acetyl cysteine (NAC) | Glutathione precursor; antioxidant | Phase II/III trials |
| D-methionine | Antioxidant | Phase II trials |
| Magnesium | Reduces cochlear vasoconstriction | Some evidence |
| Ebselen | Glutathione peroxidase mimic | Promising (Goldman-Cecil) |
| AM-111 (brimapitide) | JNK inhibitor — anti-apoptotic | Phase III for acoustic trauma |
| Vitamin C + E + β-carotene + Mg | Combination antioxidant | Animal/human trials |
No agent is currently FDA-approved for NIHL prevention or treatment.
16.3 Gene Therapy
- Atoh1 (Math1) overexpression: Viral vector delivery induces new hair cell production in deafened adult guinea pig — substantially improved hearing thresholds (Kawamoto et al.)
- First human clinical trials using cochlear gene therapy are now underway (Cummings, 2023)
16.4 Stem Cell Therapy
- Exploration of cochlear stem cell niches for hair cell regeneration
- Supporting cells (Deiters' cells) can be redirected to hair cell fate by Atoh1 overexpression
16.5 Music-Induced Hearing Loss (MIHL)
- Increasing recognition of "leisure noise" as a major public health problem
- WHO estimates 1.1 billion young people at risk from personal audio devices
- Safe listening guidelines: 60% volume for no more than 60 minutes/day ("60/60 rule")
16.6 Biomarkers
- Serum cochlin-tomoprotein (CTP) — a candidate biomarker for cochlear injury
- Urinary 8-OHdG (oxidative stress marker) elevated in NIHL workers
17. LEGAL ASPECTS
- NIHL is a compensable occupational disease under workmen's compensation laws
- Medicolegal criteria require careful separation of NIHL from presbycusis (age correction using ISO 1999 tables)
- The 4 kHz notch is the diagnostic fingerprint — 4 kHz thresholds are paradoxically often excluded from standard impairment calculations (Fletcher index uses 500, 1000, 2000 Hz average), making NIHL relatively less likely to cross disability thresholds despite significant cochlear injury
18. SUMMARY FLOWCHART — NIHL FROM EXPOSURE TO MANAGEMENT
HAZARDOUS NOISE EXPOSURE
(>85 dBA for 8 h, or impulse >140 dB)
│
▼
COCHLEAR MECHANICAL + METABOLIC INJURY
(OHCs, IHC synapses, spiral ganglion)
│
┌──────┴──────┐
▼ ▼
TTS PTS
(recovers) (permanent)
│ │
Repeated ┌────┴────────┐
exposure │ │
│ NIHL Acoustic
└────► (chronic) Trauma
│ (single blast)
▼
4 kHz NOTCH
on audiogram
│
▼
DIAGNOSIS (PTA, OAE, speech tests)
│
▼
┌───────┴────────┐
▼ ▼
PREVENTION REHABILITATION
(HCP, HPDs, (hearing aids,
otoprotection) counselling,
gene therapy — future)
REFERENCES (Textbook-Based)
- Cummings Otolaryngology Head and Neck Surgery (7th ed.) — Chapter 154 (Le Prell CG): Noise-Induced Hearing Loss, pp. 2969–3039; Chapter 152: Noise-Induced Hearing Loss and Acoustic Trauma
- KJ Lee's Essential Otolaryngology (11th ed.) — Chapter 14: Noise-Induced Hearing Loss and Industrial Audiology, pp. 324–327
- Dhingra's Diseases of Ear, Nose and Throat — Classification, TTS, PTS, audiological features, industrial deafness
- Hazarika's Textbook of ENT and Head-Neck Surgery — Occupational hearing loss, OSHA standards, audiogram patterns
- Scott-Brown's Otorhinolaryngology (8th ed.) — Cochlear physiology, noise physiology, hair cell vulnerability, genetic susceptibility
- Stell & Maran's Head and Neck Surgery — Otological aspects, hearing conservation
- Zakir Hussain's ENT — Classification, management, medicolegal aspects
QUICK REVISION TABLE — NIHL AT A GLANCE
| Parameter | Value |
|---|---|
| Type of HL | SNHL |
| Symmetry | Bilateral, symmetric |
| Earliest frequency affected | 4 kHz (3–6 kHz range) |
| Safe exposure limit (OSHA) | 90 dBA / 8 h |
| Hazardous threshold (WHO/NIOSH) | 85 dBA / 8 h |
| Impulse noise danger threshold | >140 dB SPL |
| Fastest progression period | First 10–15 years |
| Primary pathology | OHC loss (basal turn first) |
| Investigation of choice | Pure tone audiometry |
| Early detection test | DPOAE / high-freq audiometry |
| Key recent advance | Cochlear synaptopathy; gene therapy (Atoh1) |
| Treatment | No cure; hearing aids; prevention |
Sources: Cummings Otolaryngology Head and Neck Surgery (7th ed.), pp. 2969–3039 | KJ Lee's Essential Otolaryngology (11th ed.), p. 324 | Cummings Ch. 152 | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.