Artefacts observed in lung ultrasound
Reading File
search_medical_text
lung ultrasound artefacts A-lines B-lines pleural findings
search_medical_image
lung ultrasound artefacts A-lines B-lines consolidation pleural
GradeResponse
GradeResponse
Artefacts in Lung Ultrasound
Lung ultrasound (LUS) is fundamentally artefact-based — the normal aerated lung does not transmit ultrasound, so all diagnostically useful information comes from reverberation and reflection artefacts at the pleural interface.
1. A-Lines
| Feature | Detail |
|---|---|
| Appearance | Horizontal, hyperechoic lines parallel to the pleural line, equidistant from each other |
| Origin | Reverberation artefact: sound bouncing repeatedly between the pleural line and the transducer |
| Spacing | Equal to the distance between the skin and the pleural line |
| Significance | Normal aerated lung; also present in pneumothorax (distinguish by assessing lung sliding) |
A-lines represent the normal lung pattern. When accompanied by lung sliding (shimmering movement of the pleural line in real-time), they confirm normal aeration. When lung sliding is absent with pure A-lines, pneumothorax must be excluded.
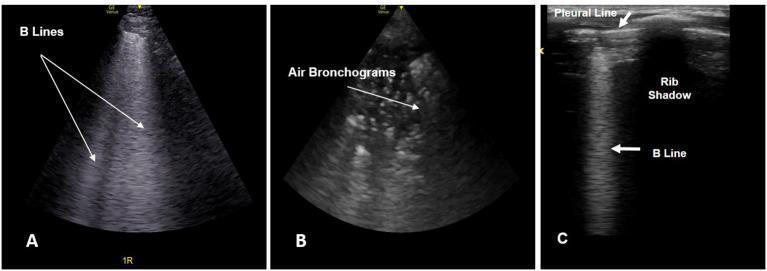
2. B-Lines (Comet-Tail Artefacts)
B-lines are the most clinically important LUS artefact. They arise from fluid-thickened interlobular septa generating a strong impedance mismatch at the pleural surface.
| Feature | Detail |
|---|---|
| Appearance | Vertical, hyperechoic, laser-like lines arising from the pleural line |
| Behaviour | Extend to the bottom of the screen without fading; erase A-lines; move with lung sliding |
| Must meet all 3 criteria | (1) Arise from pleural line, (2) reach the far field without fading, (3) move with respiration |
B-Line Patterns and Their Significance
| Pattern | Spacing | Clinical Interpretation |
|---|---|---|
| Isolated B-lines | 1–2 per zone | Normal in dependent zones (elderly, post-exercise) |
| Interstitial syndrome | 7 mm apart ("B7 lines") | Thickened interlobular septa (ILD, early pulmonary edema) |
| Pulmonary edema / confluent | < 3 mm apart ("B3 lines"), coalescing | Alveolar flooding, pulmonary edema, confluent bronchopneumonia |
| Irregular B-lines | Unevenly spaced | Pneumonia (non-uniform distribution) |
Rule: ≥ 3 B-lines per intercostal space = pathological ("B-line pattern" or "lung rockets")
(Bedside General and Cardiac Ultrasonography in the Evaluation of Critically Ill Patients, p. 13)
3. Pleural Line & Lung Sliding
Although not an artefact per se, assessment of the pleural line underpins all LUS interpretation:
- Normal lung sliding: The bright pleural line shimmers with respiration ("ants marching" in M-mode → seashore sign)
- Absent lung sliding: Seen in pneumothorax, pleurodesis, mainstem intubation, or apnoea
- M-mode in pneumothorax: Absence of lung sliding → barcode/stratosphere sign (all horizontal lines above and below M-mode trace)
4. Z-Lines
| Feature | Detail |
|---|---|
| Appearance | Short vertical artefacts from the pleural line, fading before reaching far field |
| Significance | Normal variant — do NOT erase A-lines, do not move with lung sliding (unlike B-lines) |
Z-lines must be distinguished from B-lines; their short extent and non-erasure of A-lines confirm their benign nature.
5. E-Lines (Subcutaneous Emphysema Artefact)
- Vertical hyperechoic artefacts arising from subcutaneous tissue, not the pleural line
- Seen in subcutaneous emphysema
- Prevent visualisation of the pleural line altogether
6. Air Bronchograms (within Consolidation)
While consolidation itself is a real finding (tissue-density echogenicity), the artefacts within it are diagnostically critical:
| Type | Appearance | Significance |
|---|---|---|
| Static air bronchograms | Fixed hyperechoic foci within consolidation | Suggest obstructive/atelectatic consolidation |
| Dynamic air bronchograms | Hyperechoic foci moving centrifugally with inspiration | Strongly suggest patent airways + pneumonia (rule out atelectasis) |
7. Shred Sign (Tissue–Air Interface)
- Irregular, jagged deep border of a consolidation
- Reflects partial aeration of alveoli adjacent to consolidated tissue
- Characteristic of pneumonia (contrasts with the smooth deep border of pleural effusion)
8. Lung Point
- A specific sign for pneumothorax (specificity ~100%)
- The point on the chest wall where the pneumothorax ends: alternating lung sliding (present) and absent sliding (pneumothorax) with respiration at the same location
- Seen in real-time as a sudden "flicker" of normal lung appearing at the pleural edge
Summary Table
| Artefact | Direction | Origin | Key Association |
|---|---|---|---|
| A-lines | Horizontal | Pleural reverberation | Normal lung / pneumothorax |
| B-lines | Vertical, to far field | Subpleural fluid/septa | Pulmonary edema, ILD, pneumonia |
| Z-lines | Vertical, fade early | Pleural line | Normal variant |
| E-lines | Vertical, from skin | Subcutaneous air | Subcutaneous emphysema |
| Shred sign | — | Tissue-air interface | Pneumonia |
| Lung point | — | PTX-lung border | Pneumothorax (specific) |
| Seashore sign | — | M-mode, sliding | Normal lung |
| Barcode sign | — | M-mode, no sliding | Pneumothorax |
| Dynamic air bronchogram | — | Within consolidation | Pneumonia (vs atelectasis) |
LUS artefact interpretation follows a systematic approach: assess lung sliding first, then classify the dominant pattern as A-line (aeration normal or PTX) vs B-line (interstitial/alveolar syndrome) vs consolidation, integrating clinical context for final diagnosis.
This is a shared conversation. Sign in to Orris to start your own chat.