Anti uti drugs pharmacology reference kd Tripathi book mbbs
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I have all the content needed. Now I'll compile a comprehensive, KD Tripathi-style pharmacology reference on anti-UTI drugs.
Anti-UTI Drugs - Pharmacology (MBBS Reference)
Note: KD Tripathi's Essentials of Medical Pharmacology is not directly in this library, but the content below is drawn from Goodman & Gilman, Katzung, and Lippincott Illustrated Reviews Pharmacology - the three core references that align closely with KD Tripathi's coverage of this topic for MBBS.
Classification of Drugs Used in UTI
I. Urinary Tract Antiseptics (act locally in urine, not systemic infections)
- Nitrofurantoin
- Methenamine mandelate / Methenamine hippurate
- Fosfomycin
II. Systemic Antibiotics Used for UTI
- Fluoroquinolones (ciprofloxacin, norfloxacin, ofloxacin)
- Trimethoprim-Sulfamethoxazole (Co-trimoxazole)
- Aminopenicillins (amoxicillin + clavulanate)
- Cephalosporins (oral - cephalexin, cefpodoxime)
- Aminoglycosides (gentamicin - for complicated/pyelonephritis)
I. URINARY TRACT ANTISEPTICS
A. Nitrofurantoin
Class: Synthetic nitrofuran
Mechanism of Action:
- Nitrofurantoin is activated by bacterial reductases (nitroreductases) into highly reactive intermediates
- These intermediates damage DNA and also disrupt RNA synthesis and ribosomal proteins (multiple targets)
- Bacteria reduce nitrofurantoin much faster than mammalian cells - accounts for selective toxicity
- Activity is enhanced in acidic urine (pH < 5.5)
Antimicrobial Spectrum:
- Active against: E. coli (most common UTI pathogen), Klebsiella, Enterococcus, Staphylococcus saprophyticus, Enterobacteriaceae
- Resistant: Proteus spp., Pseudomonas aeruginosa, many Enterobacter strains
- Bacteriostatic at 32 µg/mL; Bactericidal at ≥100 µg/mL
Pharmacokinetics:
- Well absorbed orally; macrocrystalline form better tolerated
- Two formulations:
- Macrocrystals (Macrodantin): slower absorption, 4x/day
- Macrocrystals + monohydrate (Macrobid): gel matrix, 2x/day
- Plasma t½ = 0.3-1 hour - excreted so rapidly that NO systemic antibacterial action achieved
- ~40% excreted unchanged in urine via glomerular filtration + tubular secretion
- Urine concentration: ~200 µg/mL (effective for lower UTI)
Uses:
- First-line for uncomplicated cystitis (lower UTI) - 5-7 days course
- NOT for pyelonephritis or upper UTI (inadequate tissue levels)
- NOT for prostatitis
- Prophylaxis of recurrent UTIs: 50-100 mg at bedtime (single daily dose)
- Preferred agent in pregnancy (except near term)
Dosage:
- Adults: 50-100 mg orally four times daily (macrocrystalline)
- OR 100 mg twice daily (macrocrystalline/monohydrate combination)
- Children: 5-7 mg/kg/day; 1 mg/kg/day for long-term prophylaxis
- Course: max 14 days; do not exceed (risk of toxicity)
Adverse Effects:
| System | Effect |
|---|---|
| GI | Nausea, vomiting, diarrhea (most common; reduced with macrocrystals) |
| Pulmonary | Pulmonary fibrosis, pneumonitis (prolonged use >1 month) |
| Neurological | Peripheral neuropathy (prolonged use, renal impairment) |
| Hematological | Hemolytic anemia (in G6PD deficiency) |
| Hepatic | Autoimmune hepatitis (rare, chronic use) |
| Hypersensitivity | Rash, fever, pulmonary infiltrates |
Contraindications:
- Renal insufficiency (CrCl <60 mL/min traditionally; some allow use if CrCl >30 mL/min for short courses)
- G6PD deficiency
- Neonates (<1 month) and pregnancy near term (risk of neonatal hemolysis)
- Hepatic insufficiency (relative)
Drug Interaction:
- Antagonizes the action of nalidixic acid and older fluoroquinolones (norfloxacin, ciprofloxacin)
- No cross-resistance with other antimicrobials
B. Methenamine Salts (Methenamine Mandelate / Methenamine Hippurate)
Mechanism of Action:
At acidic urine pH ≤ 5.5, methenamine hydrolyzes to release formaldehyde:
N₄(CH₂)₆ + 6H₂O + 4H⁺ → 6HCHO (formaldehyde) + 4NH₄⁺
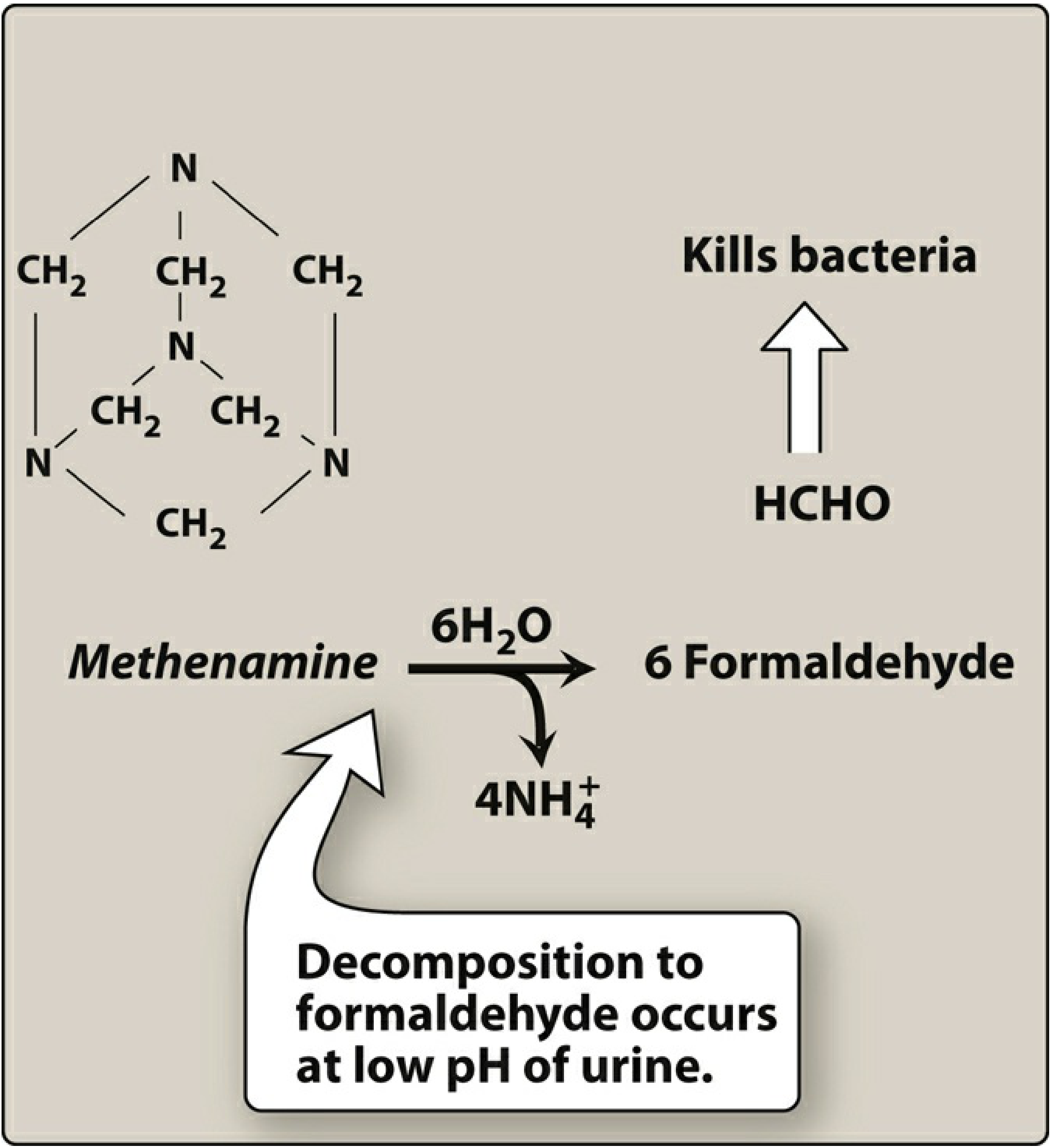
- Formaldehyde denatures proteins and nucleic acids - bactericidal
- At pH 7.4: almost no decomposition; at pH 5: 6% yield; at pH 5: 20% yield
- Reaction requires ~3 hours to reach 90% completion
- Combined with a weak acid (mandelic acid or hippuric acid) to maintain urinary acidity
- No resistance develops to formaldehyde - key advantage
Two formulations:
- Methenamine mandelate (salt of mandelic acid): mandelic acid itself is also antibacterial
- Methenamine hippurate (salt of hippuric acid): preferred in renal insufficiency (mandelic acid may precipitate in renal failure)
Antibacterial Spectrum:
- E. coli, Enterococcus, Staphylococcus
- Proteus spp. are relatively resistant - they produce urease, raising urine pH, thus preventing formaldehyde release
- Pseudomonas: some activity if urine is kept acidic
- Key advantage: does NOT select for resistant organisms
Pharmacokinetics:
- Orally absorbed; up to 30% decomposed by gastric acid (enteric coating prevents this)
- Excreted via tubular secretion + glomerular filtration
- Avoid in hepatic insufficiency (ammonia released during hydrolysis)
Uses:
- Chronic suppressive therapy (long-term prophylaxis) to reduce frequency of recurrent UTIs
- NOT appropriate for acute UTI treatment
- Requires maintenance of urine pH <5.5 for efficacy (use acidifying agents: ascorbic acid, ammonium chloride)
Adverse Effects:
- GI distress (most common)
- High doses: albuminuria, hematuria, rash
- Methenamine mandelate: contraindicated in renal insufficiency (mandelic acid precipitates)
Important Interaction:
- Do NOT combine with sulfonamides (TMP/SMX): increases risk of crystalluria and mutual antagonism
C. Fosfomycin
Class: Phosphonic acid derivative (synthetic)
Mechanism of Action:
- Inhibits MurA (enolpyruvyl transferase) - the enzyme catalyzing the first step in bacterial cell wall (peptidoglycan) synthesis
- This mechanism is unique among antibacterials - no cross-resistance with other drugs
- Also reduces bacterial adherence to urothelial cells
- Bactericidal
Antimicrobial Spectrum:
- E. coli, Proteus, Enterococcus, S. saprophyticus (common uropathogens)
- Variable: Klebsiella, Enterobacter, Serratia
- Resistant: Pseudomonas, Acinetobacter
Pharmacokinetics:
- Oral form only available in most countries (fosfomycin tromethamine - dissolved powder)
- Oral bioavailability ~40%; t½ = 5-8 hours
- After 3 g oral dose: urine concentration = 1000-4000 µg/mL (very high)
- Systemic levels are low - action confined to urinary tract
Uses:
- First-line for uncomplicated acute cystitis - single 3 g oral dose (major advantage: single-dose regimen = excellent compliance)
- Prophylaxis: 3 g every 10 days
- Complicated UTI: 3 g every other day × 3 doses
Adverse Effects:
- Well tolerated overall
- GI distress, vaginitis, headache, dizziness (all uncommon)
II. SYSTEMIC ANTIBIOTICS FOR UTI
A. Fluoroquinolones (Ciprofloxacin, Norfloxacin, Ofloxacin, Levofloxacin)
Mechanism: Inhibit DNA gyrase (in gram-negatives) and Topoisomerase IV (in gram-positives) → bactericidal
Uses in UTI:
- Uncomplicated and complicated UTIs, pyelonephritis
- Norfloxacin is concentrated in urine - primarily used for UTI
- Ciprofloxacin/Levofloxacin - used for pyelonephritis, complicated UTIs, prostatitis
Note (KD Tripathi-important): Due to increasing resistance in E. coli and FDA warnings (tendinopathy, CNS effects, peripheral neuropathy), fluoroquinolones should be reserved for UTIs where alternatives are unsuitable.
Adverse effects: Nausea, photosensitivity, QT prolongation, tendinitis/tendon rupture (boxed warning), peripheral neuropathy, CNS effects
B. Trimethoprim-Sulfamethoxazole (Co-trimoxazole / TMP-SMX)
Mechanism: Sequential blockade of folate synthesis
- Sulfamethoxazole blocks dihydropteroate synthase (inhibits PABA incorporation)
- Trimethoprim blocks dihydrofolate reductase
- Combined: synergistic bactericidal action
Uses: Uncomplicated UTI - standard 3-day course for cystitis
Avoid if: Local E. coli resistance >20% (check antibiogram); renal failure; G6PD deficiency (sulfa component); folate deficiency; pregnancy (3rd trimester)
Key interactions: Do NOT combine with methenamine (crystalluria risk)
Summary Table: UTI Drugs at a Glance
| Drug | MOA | Use | Key ADR | Key CI |
|---|---|---|---|---|
| Nitrofurantoin | Reactive intermediates → DNA/RNA damage | Uncomplicated cystitis, prophylaxis | Pulmonary fibrosis, neuropathy, hemolytic anemia (G6PD) | Renal failure, G6PD deficiency, neonates |
| Methenamine | Formaldehyde at pH <5.5 → protein denaturation | Long-term suppression/prophylaxis | GI distress, hematuria | Renal failure (mandelate), hepatic failure |
| Fosfomycin | Inhibits MurA → blocks cell wall synthesis | Acute cystitis (single dose) | GI distress (mild) | Rarely contraindicated |
| Fluoroquinolones | DNA gyrase/Topo IV inhibition | Complicated UTI, pyelonephritis, prostatitis | Tendinopathy, QT prolongation, neuropathy | Reserved - not first-line |
| TMP-SMX | Sequential folate blockade | Uncomplicated cystitis (3-day) | Crystalluria, hematotoxicity | Resistance >20%, G6PD deficiency |
Mnemonics for MBBS Exams
Drugs NOT for upper UTI/pyelonephritis:
- "Nitro Methane Fog" = Nitrofurantoin, Methenamine, Fosfomycin (all confined to lower urinary tract - do NOT use for pyelonephritis)
Nitrofurantoin ADRs - "P-N-H-G":
- Pulmonary fibrosis, Neuropathy, Hemolytic anemia (G6PD), GI distress
Methenamine needs acidic urine (pH <5.5):
- Proteus raises pH by urease → methenamine fails against Proteus
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics, 14e, p.1193; Katzung's Basic and Clinical Pharmacology, 16e, p.1395; Lippincott Illustrated Reviews Pharmacology, 8e, p.1043-1046
Anti utdrugs pharmacology reference kd Tripathi book mbbs
Reading File
This is the same question as before - I already have all the content from the previous session. Let me deliver the complete answer directly.
Anti-UTI Drugs - Pharmacology (MBBS / KD Tripathi Style)
Note: KD Tripathi's Essentials of Medical Pharmacology is not directly available in this library, but the content below is compiled from Goodman & Gilman, Katzung's Basic & Clinical Pharmacology (16e), and Lippincott Illustrated Reviews Pharmacology - the exact same topics KD Tripathi covers, in the same MBBS-oriented style.
Classification of Anti-UTI Drugs
A. Urinary Tract Antiseptics (act locally in urine, NOT systemic infections)
- Nitrofurantoin
- Methenamine mandelate / Methenamine hippurate
- Fosfomycin
B. Systemic Antibiotics Used for UTI
- Fluoroquinolones - Norfloxacin, Ciprofloxacin, Ofloxacin, Levofloxacin
- Trimethoprim-Sulfamethoxazole (Co-trimoxazole / TMP-SMX)
- Aminopenicillins - Amoxicillin + Clavulanate
- Oral Cephalosporins - Cephalexin, Cefpodoxime
- Aminoglycosides - Gentamicin (complicated UTI / pyelonephritis)
PART I - URINARY TRACT ANTISEPTICS
1. NITROFURANTOIN
Mechanism of Action
- Nitrofurantoin is activated by bacterial nitroreductases into highly reactive intermediates
- These intermediates cause DNA strand breakage, inhibit RNA synthesis, and disrupt multiple ribosomal proteins
- Bacteria reduce nitrofurantoin far more rapidly than mammalian cells - basis of selective toxicity
- Antibacterial activity is greatly enhanced in acidic urine (pH < 5.5)
Antimicrobial Spectrum
- Sensitive: E. coli (most common UTI pathogen), Klebsiella, Enterococcus, Staphylococcus saprophyticus, Enterobacteriaceae
- Resistant: Proteus spp., Pseudomonas aeruginosa, many Enterobacter strains
- Bacteriostatic at 32 µg/mL; Bactericidal at ≥100 µg/mL
- No cross-resistance with any other antimicrobial class
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Absorption | Rapid and complete oral absorption |
| Distribution | Rapid elimination - NO systemic antibacterial action |
| t½ | 0.3-1 hour (very short) |
| Urine concentration | ~200 µg/mL (adequate for lower UTI) |
| Excretion | ~40% unchanged in urine via GFR + tubular secretion |
Formulations:
- Macrocrystals (Macrodantin): slower dissolution, 4 times/day dosing
- Macrocrystals + monohydrate combination (Macrobid): gel matrix → twice daily dosing, better tolerated
Therapeutic Uses
- First-line for uncomplicated cystitis (lower UTI) - 5 to 7 day course
- Prophylaxis of recurrent UTIs: 50-100 mg single dose at bedtime
- Preferred in pregnancy (except near-term/at term)
- NOT for pyelonephritis - inadequate tissue/renal parenchymal levels
- NOT for prostatitis - does not penetrate prostatic tissue
Dosage
- Adults: 100 mg orally 4 times daily (macrocrystals) OR 100 mg twice daily (combination form)
- Children: 5-7 mg/kg/day in divided doses; 1 mg/kg/day for long-term prophylaxis
- Maximum course: 14 days; repeated courses separated by rest periods
Adverse Effects
| System | Effect |
|---|---|
| GI (most common) | Nausea, vomiting, diarrhea - less with macrocrystals |
| Pulmonary | Pulmonary fibrosis, pneumonitis (prolonged use >1 month) |
| Neurological | Peripheral neuropathy (prolonged use, especially with renal impairment) |
| Hematological | Hemolytic anemia in G6PD deficiency |
| Hepatic | Autoimmune hepatitis (rare, chronic use) |
| Hypersensitivity | Rash, fever, pulmonary infiltrates |
Contraindications
- Renal insufficiency (CrCl <60 mL/min - traditionally; avoid in significant renal failure)
- G6PD deficiency
- Neonates (<1 month) and pregnancy at/near term (risk of neonatal hemolytic anemia)
- Hepatic insufficiency
Drug Interaction
- Antagonizes the action of nalidixic acid and some fluoroquinolones (norfloxacin, ciprofloxacin)
2. METHENAMINE SALTS
Available as:
- Methenamine mandelate (salt of mandelic acid)
- Methenamine hippurate (salt of hippuric acid)
Mechanism of Action
At urine pH ≤ 5.5, methenamine is hydrolyzed to release formaldehyde:
N₄(CH₂)₆ + 6H₂O + 4H⁺ → 6 HCHO (formaldehyde) + 4NH₄⁺
- Formaldehyde denatures proteins and nucleic acids → bactericidal
- At pH 7.4: almost no decomposition; at pH 6: only 6% yield; at pH 5: 20% yield
- Hydrolysis reaction takes ~3 hours to reach 90% completion
- No organism develops resistance to formaldehyde - key long-term advantage
- Combined with mandelic acid or hippuric acid to keep urine pH acidic
Why Proteus is Resistant
Proteus spp. produce urease → splits urea → raises urine pH → prevents formaldehyde release → drug fails
Pharmacokinetics
- Orally absorbed; enteric coating prevents ~30% gastric decomposition
- Excreted via GFR + tubular secretion into urine
- Avoid in hepatic failure (ammonia released during hydrolysis can cause encephalopathy)
Therapeutic Uses
- Long-term suppressive/prophylactic therapy for recurrent UTIs
- NOT suitable for acute UTI treatment (slow onset, requires acidic urine maintenance)
- Needs concurrent urinary acidification (ascorbic acid, ammonium chloride)
Adverse Effects
- GI distress (most common)
- Higher doses: albuminuria, hematuria, rash
- Methenamine mandelate - contraindicated in renal failure (mandelic acid precipitates)
- Methenamine hippurate - safer in renal insufficiency
Important Drug Interaction
- Do NOT combine with sulfonamides (TMP-SMX): mutual antagonism + increased risk of crystalluria
3. FOSFOMYCIN
Mechanism of Action
- Inhibits MurA (enolpyruvyl transferase) - enzyme catalyzing the first step in peptidoglycan (cell wall) synthesis
- This target is unique - no cross-resistance with any other antibiotic class
- Also reduces bacterial adherence to urothelial epithelium
- Bactericidal
Antimicrobial Spectrum
- Sensitive: E. coli, Proteus, Enterococcus, S. saprophyticus
- Variable: Klebsiella, Enterobacter, Serratia
- Resistant: Pseudomonas aeruginosa, Acinetobacter
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Form | Fosfomycin tromethamine - oral powder dissolved in water |
| Bioavailability | ~40% |
| t½ | 5-8 hours |
| Urine concentration | 1000-4000 µg/mL after single 3 g dose (very high) |
| Systemic levels | Low - action confined to urinary tract |
Therapeutic Uses
- First-line for uncomplicated acute cystitis - SINGLE 3 g oral dose (best compliance)
- Complicated UTI: 3 g every other day × 3 doses
- Prophylaxis: 3 g every 10 days
Adverse Effects
- Well-tolerated overall
- Mild GI distress, vaginitis, headache, dizziness (all uncommon)
PART II - SYSTEMIC ANTIBIOTICS FOR UTI
4. FLUOROQUINOLONES
Examples: Norfloxacin, Ciprofloxacin, Ofloxacin, Levofloxacin
Mechanism: Inhibit DNA gyrase (gram-negatives) and Topoisomerase IV (gram-positives) → bactericidal
| Drug | Main UTI Use |
|---|---|
| Norfloxacin | Uncomplicated UTI (concentrates in urine) |
| Ciprofloxacin | Complicated UTI, pyelonephritis, prostatitis |
| Levofloxacin | Pyelonephritis, complicated UTI |
Current Status (KD Tripathi important point): Increasing resistance in E. coli + FDA boxed warnings (tendinopathy, peripheral neuropathy, CNS effects) mean fluoroquinolones are now reserved - not first-line for simple UTIs. Use when alternatives are unsuitable.
Adverse effects: Nausea, photosensitivity, QT prolongation, tendinitis/tendon rupture, peripheral neuropathy
5. TRIMETHOPRIM-SULFAMETHOXAZOLE (Co-trimoxazole / TMP-SMX)
Mechanism: Sequential blockade of folate synthesis
- Sulfamethoxazole → inhibits dihydropteroate synthase (blocks PABA incorporation)
- Trimethoprim → inhibits dihydrofolate reductase
- Combined effect: synergistic bactericidal action
Use: Uncomplicated UTI - standard 3-day course for cystitis
Avoid when:
- Local E. coli resistance >20% (check local antibiogram)
- Renal failure, G6PD deficiency, pregnancy (3rd trimester), folate deficiency
- Never combine with methenamine (crystalluria + antagonism)
Summary Comparison Table
| Drug | Class | MOA | Primary Use | Key ADR | Key CI |
|---|---|---|---|---|---|
| Nitrofurantoin | Nitrofuran | Reactive intermediates → DNA/RNA damage | Uncomplicated cystitis, prophylaxis | Pulmonary fibrosis, neuropathy, hemolysis (G6PD) | Renal failure, G6PD-def |
| Methenamine | Urinary antiseptic | Formaldehyde at pH <5.5 → protein denaturation | Long-term UTI suppression/prophylaxis | GI distress, hematuria | Hepatic failure, renal failure (mandelate) |
| Fosfomycin | Phosphonic acid | Inhibits MurA → blocks cell wall synthesis | Acute cystitis (single dose) | Mild GI only | Rarely |
| Fluoroquinolones | Quinolone | DNA gyrase/Topo IV inhibition | Complicated UTI, pyelonephritis, prostatitis | Tendinopathy, QT prolongation, neuropathy | Pregnancy, children (relative) |
| TMP-SMX | Antifolate | Sequential folate blockade | Uncomplicated cystitis (3-day) | Crystalluria, rash, hematotoxicity | Resistance >20%, G6PD-def |
High-Yield Exam Points (KD Tripathi Style)
1. Drugs ONLY for lower UTI (NOT pyelonephritis):
Nitrofurantoin, Methenamine, Fosfomycin - all three fail to achieve adequate tissue levels in renal parenchyma
2. Drug of choice - uncomplicated cystitis:
Nitrofurantoin (5-7 days) OR Fosfomycin (single dose) OR TMP-SMX (3 days) - all first-line
3. Drug of choice - recurrent UTI prophylaxis:
Nitrofurantoin (50-100 mg at bedtime) or Methenamine (long-term suppression)
4. Nitrofurantoin ADR mnemonic - "PNHG":
Pulmonary fibrosis, Neuropathy, Hemolytic anemia (G6PD), GI distress
5. Methenamine mechanism key points:
Needs pH <5.5 | Fails against Proteus (urease raises pH) | No resistance develops | Do NOT combine with sulfonamides
6. Fosfomycin unique features:
Single-dose regimen | Unique MOA (MurA inhibition) | No cross-resistance | Also active against Proteus (unlike nitrofurantoin)
7. Fluoroquinolone for prostatitis:
Trimethoprim and fluoroquinolones concentrate in prostatic fluid - preferred for bacterial prostatitis
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics, 14e - Katzung's Basic & Clinical Pharmacology, 16e - Lippincott Illustrated Reviews Pharmacology, 8e (pp. 1043-1046)
This is a shared conversation. Sign in to Orris to start your own chat.