ASSR in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching Images
ASSR auditory steady state response diagram waveform
Searching Images
auditory evoked potential ABR ASSR comparison audiogram
Loading Image
Loading Image
Finding Sources
Now I have sufficient information from the textbooks. Let me compile a comprehensive 50-mark ASSR answer for RGUHS.
Auditory Steady-State Response (ASSR)
A Comprehensive Review for 50-Mark RGUHS Examination
1. INTRODUCTION & DEFINITION
The Auditory Steady-State Response (ASSR) is an objective, frequency-specific electrophysiological test used to estimate hearing thresholds. It is a continuous, sinusoidal, amplitude-modulated auditory evoked response generated by the auditory system when stimulated by modulated pure tones. Unlike the ABR which uses transient click/tone-burst stimuli, ASSR uses steady-state (continuous) stimuli and detects the response via statistical/mathematical algorithms rather than morphological waveform analysis.
— Cummings Otolaryngology Head and Neck Surgery; K.J. Lee's Essential Otolaryngology
2. HISTORICAL BACKGROUND
| Year | Milestone |
|---|---|
| 1981 | Galambos et al. described the 40 Hz response (early ASSR) |
| 1990s | Rees et al. recognized the importance of ~80 Hz modulation frequency in sleeping subjects |
| 1993 | Picton et al. defined ASSR in its current form |
| 2001 | MASTER (Multiple Auditory Steady-State Response) system developed by Picton – enabled simultaneous multi-frequency testing |
| 2002 onwards | Commercial ASSR systems (Bio-logic, Interacoustics AUDERA, Intelligent Hearing Systems) entered routine clinical use |
| Recent | Bone-conduction ASSR, binaural ASSR, neonatal ASSR protocols gaining evidence |
3. PHYSICS & STIMULUS CHARACTERISTICS
Stimulus Composition
ASSR uses amplitude-modulated (AM) tones — a carrier frequency (CF) modulated by a modulation frequency (MF):
ASSR Stimulus = Carrier Frequency (CF) × Modulation Frequency (MF)
CF = 500, 1000, 2000, 4000 Hz (test frequencies)
MF = 40 Hz (awake) or 70–110 Hz (sleep/sedation)
Mathematical representation:
S(t) = A [1 + m·cos(2π·fm·t)] · cos(2π·fc·t)Where: A = amplitude, m = modulation depth (typically 100%), fm = modulation frequency, fc = carrier frequency
Types of Modulation
- Amplitude Modulation (AM) — variation in amplitude at MF rate
- Frequency Modulation (FM) — variation in frequency at MF rate
- Mixed AM+FM (most commonly used clinically) — superior SNR
— K.J. Lee's Essential Otolaryngology, p. 337
4. NEUROPHYSIOLOGICAL BASIS
┌─────────────────────────────────────────────────────────────┐
│ NEURAL GENERATORS OF ASSR │
├──────────────────┬──────────────────────────────────────────┤
│ 40 Hz ASSR │ Primary Auditory Cortex (A1) │
│ │ Middle Latency Response generators │
│ │ Thalamo-cortical loops │
├──────────────────┼──────────────────────────────────────────┤
│ 80 Hz ASSR │ Brainstem (Inferior Colliculus) │
│ │ Cochlear Nucleus │
│ │ Superior Olivary Complex │
│ │ Auditory Nerve │
└──────────────────┴──────────────────────────────────────────┘
The Theoretical Assumption (K.J. Lee):
"The part of the cochlea stimulated by the carrier frequency (e.g., 1000 Hz) must be intact for the cochlea to respond to the modulation rate (e.g., 80 Hz), producing an ASSR."
This means:
- CF determines cochlear place (tonotopic specificity)
- MF determines the neural following rate (temporal coding)
- When the cochlea at CF region is intact → sustained neural discharge phase-locked to MF → measurable ASSR
5. THE 40 Hz vs 80 Hz DICHOTOMY
| Feature | 40 Hz ASSR | 80 Hz ASSR |
|---|---|---|
| Generator | Auditory cortex | Brainstem |
| State sensitivity | Very sensitive to sleep/sedation | Stable during sleep and sedation |
| Use in neonates | Not reliable | Preferred |
| Amplitude | Higher (easier to detect) | Lower |
| Threshold correlation | Less accurate | Better threshold correlation |
| Clinical utility | Adults awake | Neonates, sedated patients |
6. FLOWCHART: HOW ASSR IS PERFORMED
┌──────────────────────────┐
│ PATIENT PREPARATION │
│ (Sleep/Sedation for │
│ infants; awake adults) │
└────────────┬─────────────┘
│
┌────────────▼─────────────┐
│ ELECTRODE PLACEMENT │
│ • Active: Cz (vertex) │
│ • Reference: mastoid │
│ • Ground: forehead │
└────────────┬─────────────┘
│
┌────────────▼─────────────┐
│ STIMULUS DELIVERY │
│ AM tones via insert │
│ earphones │
│ CF: 500,1000,2000,4000Hz│
│ MF: 70-100 Hz │
└────────────┬─────────────┘
│
┌────────────▼─────────────┐
│ SIGNAL ACQUISITION │
│ EEG recorded from scalp │
│ electrodes │
└────────────┬─────────────┘
│
┌────────────▼─────────────┐
│ FOURIER ANALYSIS (FFT) │
│ Transform EEG to │
│ frequency domain │
└────────────┬─────────────┘
│
┌────────────▼─────────────┐
│ STATISTICAL DETECTION │
│ F-test or phase │
│ coherence algorithm │
│ (p < 0.05 = PRESENT) │
└────────────┬─────────────┘
│
┌──────────────────┴──────────────────┐
│ │
┌───────────▼──────────┐ ┌────────────▼──────────┐
│ RESPONSE PRESENT │ │ RESPONSE ABSENT │
│ Reduce intensity │ │ Increase intensity │
│ (10 dB steps) │ │ (10 dB steps) │
└───────────┬──────────┘ └────────────┬──────────┘
│ │
└────────────────┬─────────────────────┘
│
┌────────────▼─────────────┐
│ THRESHOLD DETERMINATION │
│ Lowest level with │
│ significant response │
└────────────┬─────────────┘
│
┌────────────▼─────────────┐
│ CORRECTION FACTOR │
│ Added to convert ASSR │
│ threshold → Behavioral │
│ threshold equivalent │
└──────────────────────────┘
7. STATISTICAL RESPONSE DETECTION
This is a key advantage of ASSR over ABR. The response is detected objectively by algorithms:
Methods of Detection:
-
F-ratio test (ANOVA-based) — compares the energy at the MF to background EEG noise
- F = Signal variance / Noise variance
- Significant if F > critical value at p < 0.05
-
Phase Coherence (Rayleigh test) — measures consistency of phase across sweeps
- More robust at low SNR conditions
-
Weighted averaging — used in MASTER system
FFT of EEG
│
─────┴─────
│ │
Energy at Energy at
MF (Hz) adjacent bins
(signal) (noise)
│ │
└────┬────┘
│
F-ratio
│
p < 0.05?
┌───┴───┐
YES NO
│ │
RESPONSE NO RESPONSE
PRESENT PRESENT
— K.J. Lee's Essential Otolaryngology, p. 337: "A complex and sophisticated algorithm is performed that is specific to the manufacturer and ASSR unit to analyze the electrophysiological response."
8. SIMULTANEOUS MULTI-FREQUENCY TESTING (MASTER)
One of the most significant advantages of ASSR is simultaneous multi-frequency testing:
┌─────────────────────────────────────────────────────────┐
│ MASTER SYSTEM PROTOCOL │
│ │
│ RIGHT EAR │ LEFT EAR │
│ 500 Hz CF @ 77 Hz MF│ 500 Hz CF @ 85 Hz MF │
│ 1000 Hz CF @ 85 Hz MF│ 1000 Hz CF @ 93 Hz MF │
│ 2000 Hz CF @ 93 Hz MF│ 2000 Hz CF @ 101 Hz MF │
│ 4000 Hz CF @ 101 Hz MF│ 4000 Hz CF @ 109 Hz MF │
│ │
│ → 8 frequencies tested SIMULTANEOUSLY (both ears) │
│ → Each frequency uses UNIQUE modulation frequency │
│ → FFT separates responses at different MF peaks │
└─────────────────────────────────────────────────────────┘
This significantly reduces test time compared to ABR, which tests one frequency at a time.
9. CLINICAL APPLICATIONS
A. Threshold Estimation in Neonates/Infants
- Gold standard complementary test alongside click ABR in newborn hearing screening
- Provides frequency-specific thresholds at 500, 1000, 2000, 4000 Hz
- Particularly valuable when behavioral audiometry is unreliable (< 6 months developmental age)
B. Severe-to-Profound Hearing Loss
- Critical advantage over ABR: ASSR can differentiate between severe (70–90 dB) and profound (>90 dB) hearing loss
- ABR saturates at ~90–100 dB nHL; ASSR systems can test up to 120 dB SPL
- Essential before cochlear implant candidacy selection
C. Confirmation of ABR Findings
- ASSR and ABR thresholds show moderate-to-strong correlation (varies by study)
- Cummings (2019): "ASSR is often used to confirm ABR results"
- ASSR is complementary, not a replacement for ABR
D. Bone Conduction ASSR
- Can estimate bone conduction thresholds
- Helps determine air-bone gap in conductive hearing loss (0.5–4 kHz)
- Data validation limited; masking is complex
E. Pseudohypacusis (K.J. Lee)
- Because it is an objective test, ASSR/ABR is powerful for detecting functional/non-organic hearing loss
- Cannot be voluntarily suppressed by the patient
F. Pre-fitting of Hearing Aids
- Provides frequency-specific audiometric data in patients who cannot perform behavioral audiometry
- Guides hearing aid selection and programming
10. ASSR THRESHOLD vs BEHAVIORAL THRESHOLD
ASSR thresholds are generally higher (worse) than behavioral thresholds by a correction factor:
| Frequency | Correction Factor (mean) |
|---|---|
| 500 Hz | ~10–15 dB |
| 1000 Hz | ~10 dB |
| 2000 Hz | ~8–10 dB |
| 4000 Hz | ~5–8 dB |
Estimated Behavioral Threshold = ASSR Threshold − Correction Factor
This correction is necessary because ASSR thresholds reflect neural detection thresholds rather than perceptual thresholds.
11. ABR vs ASSR — COMPARATIVE TABLE
| Parameter | ABR | ASSR |
|---|---|---|
| Stimulus | Click / Tone burst | Amplitude-modulated tones |
| Stimulus type | Transient | Continuous (steady-state) |
| Response domain | Time domain (waveform) | Frequency domain (FFT) |
| Detection | Visual (subjective) | Statistical algorithm (objective) |
| Frequency specificity | Moderate | High |
| Number of frequencies | One at a time | Up to 8 simultaneously |
| Test time | Longer | Shorter |
| Severe-profound HL | Limited | Superior |
| Neonatal use | Gold standard | Complementary |
| State dependence | Less affected at 80 Hz | MF-dependent |
| Retrocochlear info | Yes (Wave I–V) | No |
| Bone conduction | Well validated | Limited data |
— Cummings Otolaryngology; K.J. Lee's Essential Otolaryngology
12. ADVANTAGES OF ASSR
(K.J. Lee's Essential Otolaryngology, p. 337)
- Estimates severe-to-profound hearing loss — information unavailable from click or tone-burst ABR
- Reasonably frequency-specific — pure-tone audiogram equivalent
- Automated statistical analysis — removes examiner subjectivity
- Objective for both subject and examiner
- Records simultaneous responses — faster assessment (MASTER)
- High-level testing up to 120 dB SPL
- Does not rely on subjective waveform interpretation
- Useful in malingering/pseudohypacusis
13. DISADVANTAGES OF ASSR
(K.J. Lee's Essential Otolaryngology, p. 337)
- Requires quiet patient state — sleep or sedation needed in infants/toddlers
- Possible artifactual response — cardiac, myogenic, or electrical artifacts can mimic ASSR
- Limited anatomic site of lesion information — cannot differentiate cochlear from retrocochlear pathology
- Difficult with bone conduction — may require masking
- Overestimation of thresholds at near-normal hearing levels
- Cannot distinguish profound hearing loss from auditory neuropathy
- More research needed — normative data limited; sedative effects on results incompletely characterized
- Varying threshold correlation with ABR across studies
14. FLOWCHART: ASSR IN NEONATAL HEARING ASSESSMENT PATHWAY
NEWBORN
│
▼
┌─────────────────┐
│ NHS SCREENING │
│ OAE / AABR │
└────────┬────────┘
│
┌───────┴───────┐
PASS REFER
│ │
▼ ▼
Discharge Diagnostic ABR
(click + tone burst)
│
┌──────────┴──────────┐
NORMAL ABNORMAL
│ │
PASS ┌────────▼────────┐
│ ASSR testing │
│ (frequency │
│ specific │
│ thresholds) │
└────────┬────────┘
│
┌────────────────┤
│ │
Near-normal Severe/Profound
thresholds thresholds
│ │
Hearing aids/ Cochlear implant
monitoring candidacy
evaluation
15. ASSR IN RELATION TO OTHER AEPs
CLASSIFICATION OF AUDITORY EVOKED POTENTIALS
│
├── EARLY (< 10 ms) — Brainstem
│ ├── ECochG (Electrocochleography)
│ └── ABR (Waves I–V)
│
├── MIDDLE LATENCY (10–50 ms) — Thalamocortical
│ ├── Middle Latency Response (MLR) — Na, Pa, Nb, Pb
│ └── 40 Hz ASSR (overlapping MLR generators)
│
├── LATE / CORTICAL (> 50 ms)
│ ├── N1-P2 (CERA)
│ └── P300 / MMN (cognitive)
│
└── STEADY-STATE (frequency domain)
├── 40 Hz ASSR — cortical generator
└── 80 Hz ASSR — brainstem generator ← CLINICALLY PREFERRED
ASSR synonyms (K.J. Lee):
- Auditory Steady-State Evoked Potential (ASSEP)
- 40-Hz response
- Steady-State Evoked Potential (SSEP)
- Amplitude Modulation Following Response (AMFR)
- Envelope Following Response (EFR)
- Frequency Following Response (FFR)
16. CLINICAL IMAGES
ASSR + ABR Waveforms in Unilateral Hearing Loss
The image below shows ABR (panels A, B) and ASSR (panel C) recordings in a pediatric patient with right-sided hearing loss, alongside DPOAE DP-grams (E, F) and MRI (G, H):
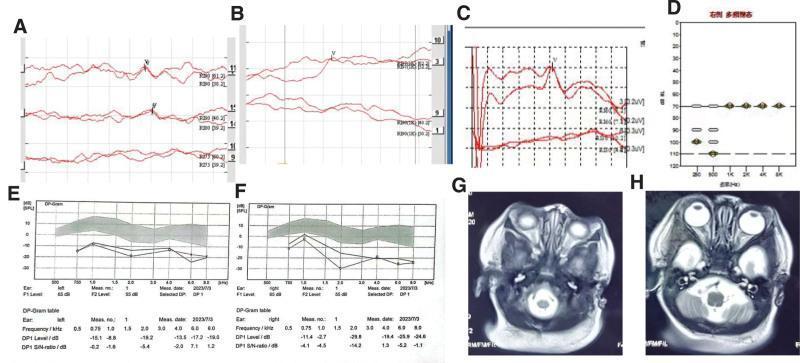
Red traces show diminished Wave V peaks at high dB levels in the right ear, with ASSR confirming significant threshold shift. DPOAE absent bilaterally.
ASSR Temporal Modulation Transfer Functions (TMTF)
The following shows individual ASSR amplitudes (µV) vs. modulation frequency (Hz) across 25 subjects — demonstrating inter-subject variability in cortical ASSR generators:
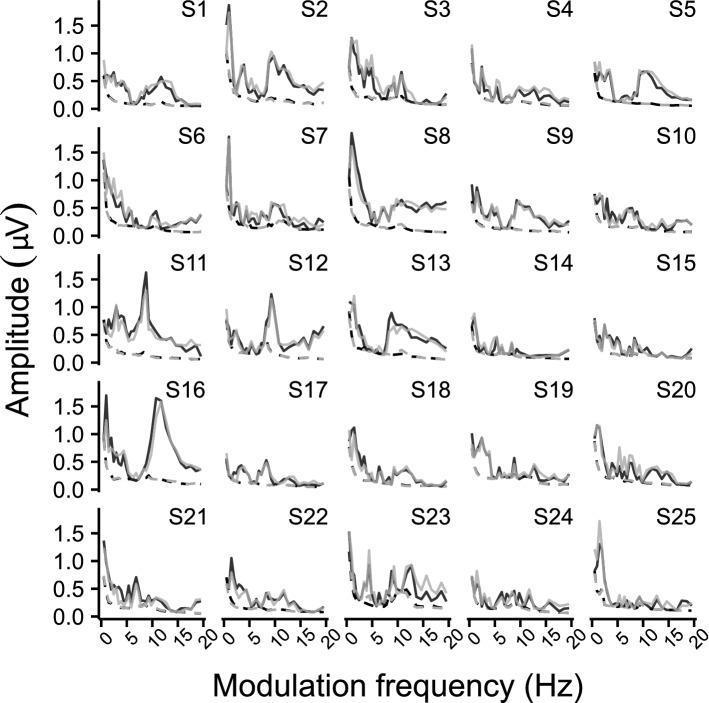
Solid lines = ASSR amplitude; dashed lines = neural noise floor. Black = left hemisphere, gray = right hemisphere.
17. RECENT ADVANCES
A. Bone Conduction ASSR
- Provides frequency-specific BC thresholds, useful in conductive/mixed hearing loss
- Limitation: masking difficulties; inter-device variability
- Studies show BC-ASSR correlates reasonably with BC-ABR at 0.5–4 kHz (Cummings, 2019)
B. Cortical ASSR (40 Hz) in Auditory Processing
- 40 Hz ASSR is being investigated as a biomarker for schizophrenia and autism spectrum disorder — gamma-band (40 Hz) ASSR is reduced in schizophrenia (Kaplan & Sadock)
- May reflect thalamocortical connectivity
C. ASSR with Narrow-Band CE-Chirp Stimuli
- CE-chirp stimulus compensates for cochlear traveling wave delay
- Results in larger amplitude ASSR, better SNR, shorter test time compared to pure tone AM stimuli
D. Multiple Auditory Steady-State Response (MASTER)
- Simultaneous bilateral, multi-frequency testing
- Reduces test time by ~60–70% vs sequential ABR
- Particularly valuable in sedated neonates (limited sedation window)
E. Automated ASSR (A-ASSR)
- Integrated into newborn screening protocols in some centres
- Automated pass/refer output without audiologist interpretation
- Challenges: higher refer rates than AABR
F. ASSR in Auditory Neuropathy Spectrum Disorder (ANSD)
- ASSR is absent or severely degraded in ANSD (unlike OAEs which are present)
- Helps differentiate cochlear from neural pathology
G. Objective Audiogram via ASSR
- Concept of generating a predicted audiogram from ASSR thresholds with frequency-specific correction factors
- Being incorporated into AI-aided audiological assessment platforms
18. LIMITATIONS SPECIFIC TO RGUHS EXAMINATION EMPHASIS
The following points are frequently tested in long-answer RGUHS questions:
- ASSR cannot replace ABR as the gold standard in neonatal hearing assessment — it is complementary (Cummings)
- The 80 Hz ASSR is preferred over 40 Hz in sleeping infants because 40 Hz responses are state-dependent and suppressed during sleep
- ASSR provides the only objective means of estimating thresholds in the severe-to-profound range beyond ABR's upper limit
- The correction factor is essential to convert ASSR thresholds to estimated behavioral thresholds
- ASSR cannot localize the site of lesion (cochlear vs retrocochlear)
19. SUMMARY TABLE
| Feature | Detail |
|---|---|
| Full form | Auditory Steady-State Response |
| Stimulus | AM (or AM+FM) tones |
| Carrier frequency | 500, 1000, 2000, 4000 Hz |
| Modulation frequency | 40 Hz (cortical) or 70–110 Hz (brainstem) |
| Response detection | Statistical (F-test/phase coherence) |
| Neural generator (80 Hz) | Brainstem (IC, cochlear nucleus) |
| Neural generator (40 Hz) | Auditory cortex |
| Preferred MF in neonates | 70–100 Hz (state-independent) |
| Main advantage | Frequency-specific, objective, severe-profound HL |
| Main limitation | Cannot distinguish ANSD, no retrocochlear info |
| Clinical use | Threshold estimation, CI candidacy, neonatal screening |
| Textbook references | Cummings, K.J. Lee, Scott Brown, Dhingra, Hazarika |
REFERENCES (Standard Textbooks for RGUHS)
- Cummings Otolaryngology – Head and Neck Surgery, 7th Ed — Chapter on Pediatric Audiology (ASSR as complementary to ABR, threshold estimation in severe-profound HL)
- K.J. Lee's Essential Otolaryngology, 11th Ed — Chapter on Audiologic Tests (Auditory Steady-State Evoked Potentials, Advantages/Disadvantages)
- Scott Brown's Otorhinolaryngology, Head and Neck Surgery — Paediatric Audiology chapter (threshold estimation, neonatal hearing)
- Stell and Maran's Head and Neck Surgery — Audiological assessment section
- Dhingra's Diseases of Ear, Nose and Throat, 7th Ed — ERA/Objective Audiometry chapter
- Hazarika's Textbook of ENT and Head & Neck Surgery — Electrophysiological tests chapter
- Zakir Hussain's Principles of Audiology — ASSR principles, clinical applications
- Picton et al. (2003) — "Human auditory steady-state responses" — Ear and Hearing — foundational reference for MASTER system
- Lins et al. (1996) — Comparison of ASSR and ABR thresholds — Ear and Hearing
- Celik et al. (2016) — ASSR vs ABR threshold correlation study (cited in Cummings)
Examiner's Note (RGUHS 50-mark format): For full marks, cover: definition + physics/stimulus + neural basis + 40 Hz vs 80 Hz comparison + procedure/electrode placement + statistical detection + MASTER system + clinical applications + advantages/disadvantages + comparison with ABR + recent advances. Include at least 2 flowcharts and 1 comparative table in the answer.
This is a shared conversation. Sign in to Orris to start your own chat.