Explain mi
It looks like your message got cut off! Could you finish your thought? Were you asking about:
- MI (Myocardial Infarction / heart attack)?
- MI (Motivational Interviewing)?
- MI (Machine Intelligence / something tech-related)?
- Something else entirely?
First one
Reading File
Finding Sources
Searching PubMed
"myocardial infarction"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information to write a thorough, well-structured answer. Let me compile it all.
Myocardial Infarction (MI) - Heart Attack
Definition
A myocardial infarction (MI), commonly called a heart attack, is death of cardiac muscle due to prolonged ischemia - when blood supply to part of the myocardium is cut off long enough to cause irreversible cell death. It affects roughly 800,000 people in the US each year (nearly one MI every 40 seconds), causing approximately 400,000 deaths annually. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Types of MI
MI falls under the broader category of Acute Coronary Syndrome (ACS):
| Type | Key Feature | Mechanism |
|---|---|---|
| STEMI | ST elevation on ECG | Complete occlusion - transmural ischemia |
| NSTEMI | No ST elevation, + troponin | Partial occlusion - subendocardial damage |
| Unstable Angina (UA) | No ST elevation, - troponin | Partial occlusion - no necrosis yet |
STEMI accounts for 25-30% of ACS cases and carries the highest acute mortality (6-10% in modern care, but >30% untreated). - Washington Manual of Medical Therapeutics
Pathogenesis - How It Happens
The sequence of events in most MIs follows this chain (as described in Robbins Pathologic Basis of Disease):
- Plaque disruption - An atheromatous plaque is eroded or suddenly ruptured by endothelial injury, intraplaque hemorrhage, or mechanical forces, exposing subendothelial collagen and necrotic plaque contents to blood.
- Platelet activation - Platelets adhere, aggregate, and release thromboxane A2, ADP, and serotonin, causing further aggregation and vasospasm.
- Coagulation cascade - Tissue factor activation adds to the growing thrombus.
- Complete occlusion - Within minutes, the thrombus can fully occlude the coronary artery lumen.
When angiography is performed within 4 hours of MI onset, coronary thrombosis is demonstrated in almost 90% of cases.
In ~10% of cases, MI occurs without typical atherothrombosis - via vasospasm, embolism (from mural thrombus in atrial fibrillation, endocarditis vegetations, or prosthetic material), vasculitis, sickle cell disease, or cocaine use.
Cellular Timeline - What Happens to Heart Muscle
| Time After Occlusion | Event |
|---|---|
| Seconds | ATP depletion begins; aerobic metabolism stops |
| < 2 minutes | Loss of contractility |
| 10 minutes | ATP reduced to 50% of normal |
| 20-40 minutes | Irreversible cell injury (necrosis begins) |
| 40 minutes | ATP reduced to 10% of normal |
| > 1 hour | Microvascular injury |
| 6-12 hours | Necrosis is complete |
The subendocardial zone is the first to die - it receives blood last from epicardial vessels and faces the highest intramural pressures. With prolonged ischemia, a wavefront of necrosis moves outward from the subendocardium toward the epicardium. - Robbins Pathologic Basis of Disease
Necrotic myocytes release intracellular proteins (especially cardiac troponins) into the bloodstream - the basis of blood tests used to diagnose MI.
Clinical Presentation
Classic symptoms:
- Crushing, pressure-like, or squeezing chest pain (often radiating to the left arm, jaw, or back)
- Diaphoresis (sweating)
- Shortness of breath (dyspnea)
- Nausea and vomiting
- Sense of impending doom
Atypical presentations occur especially in women, elderly, diabetics, and post-surgical patients, who may present with confusion, unexplained hypotension, heart failure, or no chest pain at all. - Washington Manual
ECG Changes - Evolution Over Time
The ECG is essential. An ECG must be obtained within 10 minutes of arrival. Here is how changes evolve:
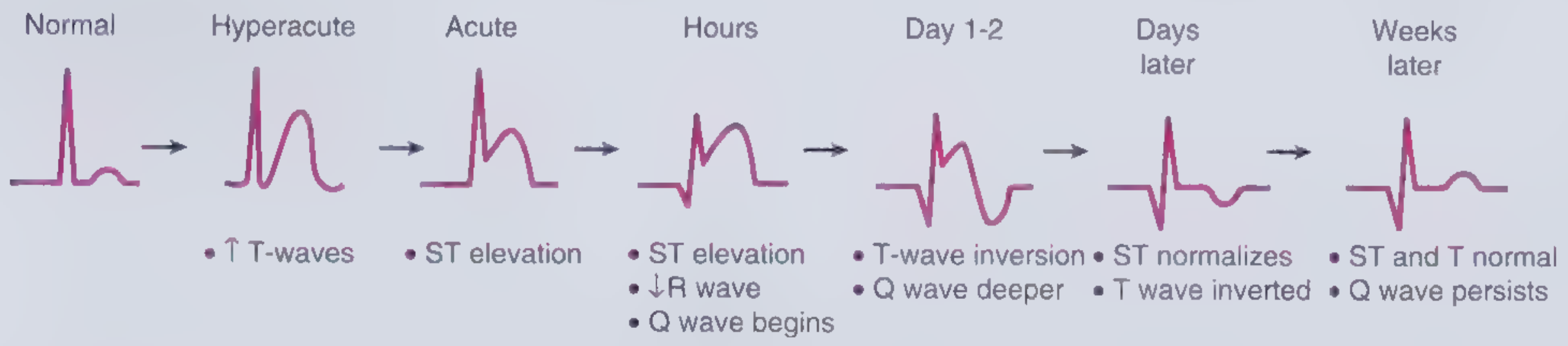
The three underlying electrical abnormalities causing ST elevation are (from Ganong's Review of Medical Physiology):
- Rapid repolarization in infarcted fibers (due to K+ channel opening) → current flows out of infarct → ST elevation
- Decreased resting membrane potential (from K+ loss) → current flows into infarct during diastole → TQ segment depression, recorded as ST elevation
- Delayed depolarization in infarcted fibers → infarcted area positive relative to healthy tissue → ST elevation
ECG localization of MI by territory:
| ST Elevation Leads | Territory | Culprit Artery |
|---|---|---|
| V2-V4 | Anterior wall | LAD |
| V1-V2 | Septum | Proximal LAD/septal branch |
| V5-V6 | Lateral wall | LCX |
| II, III, aVF | Inferior wall | RCA or LCX |
| I, aVL | High lateral wall | Diagonal or proximal LCX |
| V1-V6 + LBBB | Anterior + septal | Proximal LAD or left main |
- Washington Manual of Medical Therapeutics
Diagnosis
Three pillars:
- Symptoms - classic or atypical chest pain/discomfort
- ECG - ST elevation (STEMI) or ST depression/T-wave changes (NSTEMI/UA)
- Cardiac biomarkers - Cardiac-specific troponin I or T (most sensitive/specific); also CK-MB
Note: Troponins may be normal in the first 2-4 hours. Serial measurement is needed. Peak troponin level correlates with infarct size.
Treatment
Immediate goals: MONA + Reperfusion
Initial drugs (given immediately):
- Aspirin (ASA) 162-325 mg chewed immediately
- P2Y12 inhibitor (Ticagrelor 180 mg loading, or Clopidogrel/Prasugrel) - dual antiplatelet therapy (DAPT)
- Anticoagulation - Unfractionated heparin (UFH) 60 units/kg IV bolus, or LMWH (enoxaparin), or bivalirudin
- Nitroglycerin 0.4 mg SL (avoid in hypotension or right ventricular MI)
- Beta-blockers (metoprolol 25 mg PO) - avoid in heart failure, heart block, or bronchospasm
- High-intensity statin therapy
Reperfusion - the most critical step
Mortality is directly related to total ischemia time - the faster reperfusion, the better the outcome.
Primary PCI (preferred):
- Goal: door-to-balloon time < 90 minutes at a PCI-capable center
- Stenting of the culprit artery is standard
Fibrinolytic therapy (thrombolytics):
- Used when PCI is not available within 120 minutes
- Agents: Alteplase (tPA), tenecteplase, reteplase
- Must be given within 12 hours of symptom onset
Recent evidence update: A 2025 meta-analysis in Eur J Prev Cardiol (PMID: 39298680) found that beta-blockers for secondary prevention after MI may provide less benefit in patients without reduced ejection fraction or heart failure than traditionally assumed - an evolving area of guideline discussion.
Complications
| Complication | Timing | Details |
|---|---|---|
| Arrhythmias (VF, VT) | Minutes to hours | Accounts for ~50% of mortality; VF most common cause of death |
| Cardiogenic shock | Hours-days | Pump failure; high mortality |
| Papillary muscle rupture | Days | Acute severe mitral regurgitation |
| Ventricular septal defect (VSD) | Days | New systolic murmur |
| Free wall rupture | 3-7 days | Catastrophic; ~90% mortality with mechanical complications |
| Pericarditis (Dressler syndrome) | Weeks | Autoimmune; pleuritic chest pain |
| LV aneurysm | Weeks-months | Risk of thrombus and embolism |
Secondary Prevention (Post-MI)
- Aspirin indefinitely (81 mg/d)
- P2Y12 inhibitor (DAPT) for at least 12 months post-PCI with drug-eluting stent
- High-intensity statin (atorvastatin 40-80 mg or rosuvastatin 20-40 mg)
- ACE inhibitor or ARB (especially if EF < 40%, diabetes, or hypertension)
- Beta-blocker (especially if EF < 40% or with heart failure)
- Cardiac rehabilitation
- Risk factor modification: smoking cessation, blood pressure control, diabetes management
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease | Washington Manual of Medical Therapeutics | Ganong's Review of Medical Physiology | Frameworks for Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.