Inter trochantric fracture
Reading File
Finding Sources
Searching PubMed
"intertrochanteric fracture"[MeSH Terms] AND management
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Now I have comprehensive information. Let me compile a detailed answer.
Intertrochanteric Fracture
Definition and Overview
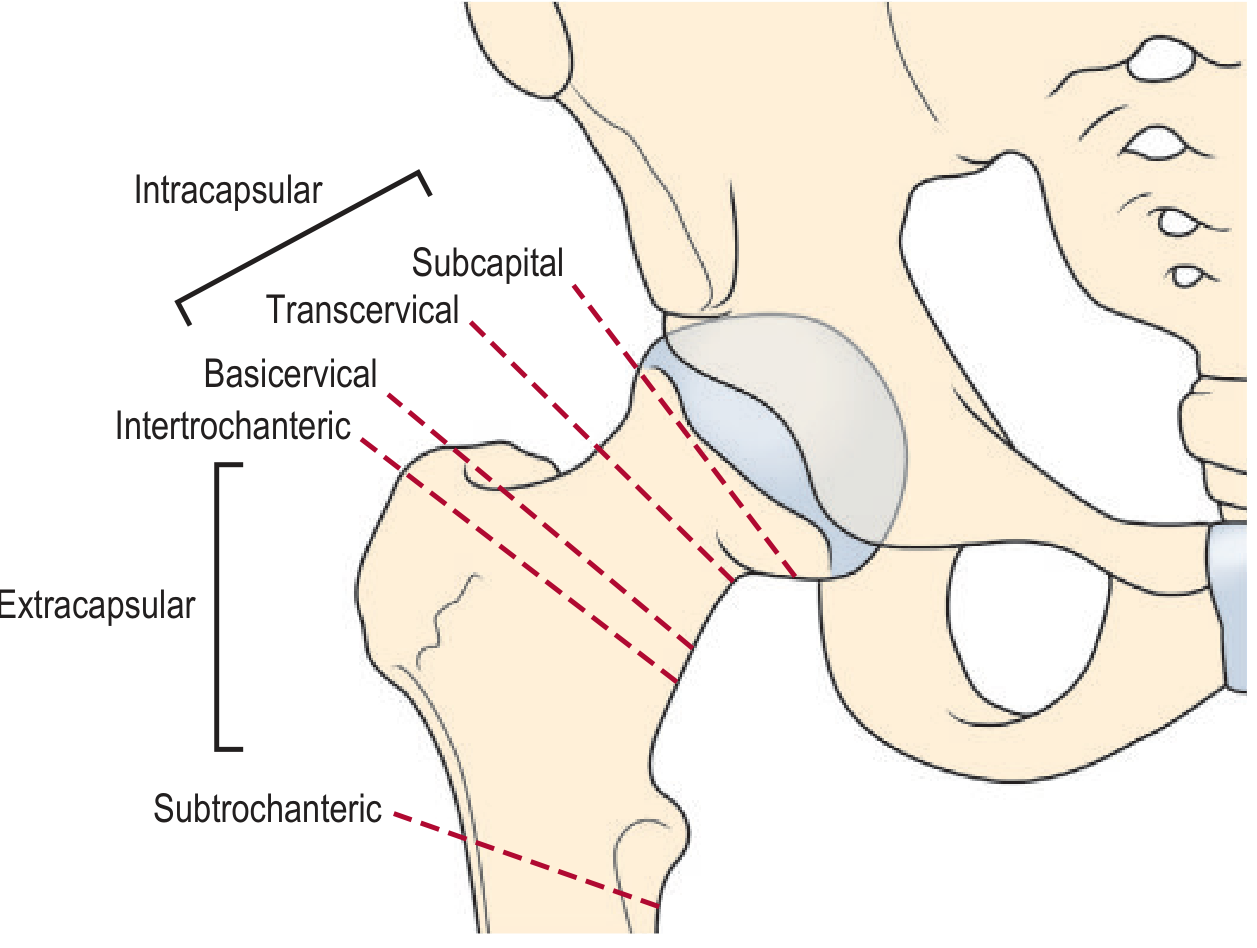
An intertrochanteric fracture is an extracapsular fracture of the proximal femur occurring between the greater and lesser trochanters, along the intertrochanteric line. Because it is extracapsular, the blood supply to the femoral head is at much less risk than with intracapsular (femoral neck) fractures - a key distinction. It is the most common type of hip fracture.
Epidemiology and Etiology
- Predominantly affects the elderly (especially post-menopausal women with osteoporosis)
- Usually follows a low-energy fall from standing height - often sideways onto the hip
- Reduced bone density (osteopenia/osteoporosis), sarcopenia, impaired balance, visual problems, and multiple medications all contribute
- In ~4% of cases, an associated fracture is present (most commonly ipsilateral distal radius 2%, or proximal humerus 1%)
- After one hip fracture, a second contralateral hip fracture occurs in up to 1 in 3 patients within 1.5 years
Risk factors for falling (Table 54-1, Rockwood & Green 2025):
- Increased age, concurrent illness, mental impairment, gait/balance disorders
- Physical disability, visual abnormalities, prior stroke
- Medications: tranquilizers, antihypertensives, multiple drug polypharmacy, alcohol
Classification (OTA/AO - 31.A)
The most widely used classification is the OTA/AO system, which divides trochanteric fractures into 3 main types:
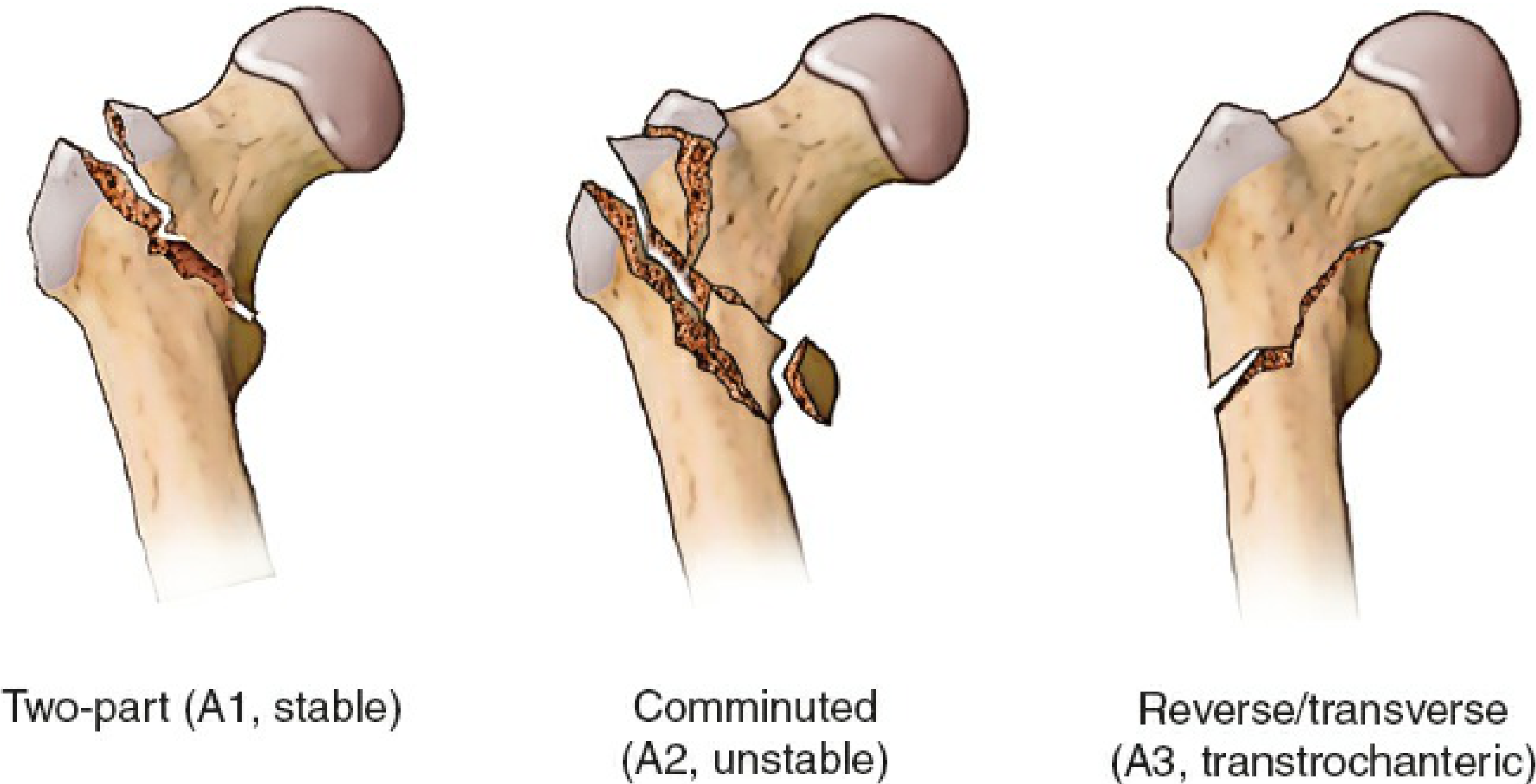
| Type | Pattern | Stability | Key Feature |
|---|---|---|---|
| A1 | Two-part fracture through the trochanters | Stable | Intact lateral wall; medial cortex interrupted in one place; lesser trochanter may be attached to either fragment |
| A2 | Comminuted - main fracture line through trochanters | Unstable | Lateral wall intact but 3-4 fragments; lesser trochanter detached; coronal fragments possible |
| A3 | Reverse oblique or transverse | Unstable/Challenging | Fracture from lesser trochanter extends to lateral cortex; lateral wall is unstable; may extend into subtrochanteric region |
The lateral wall integrity is the single most important factor in planning surgery - an intact lateral wall defines A1 vs A2, while an unstable lateral wall defines A3.
Clinical Features (Diagnosis)
Symptoms:
- Acute pain around the hip and thigh; inability to stand or walk
- Pain may radiate to the ipsilateral knee
- Affected leg is shortened and externally rotated (due to deforming muscle forces)
- In a nondisplaced fracture, axial compression pain may be the only finding
Examination:
- Contusion or hematoma around the hip
- Passive range of motion painful
- Unlike femoral neck fractures, the patient typically gives a history of tripping over a carpet, pet, or step (direct sideways fall)
Imaging
Plain X-rays (first-line):
- AP pelvis (both hips included) + lateral hip
- The non-involved hip helps assess normal anatomy for comparison
- Comminuted fractures are easily identified; minimally displaced fractures can be occult (~1%)
MRI (gold standard for occult fractures):
- Most sensitive and specific; indicated when fracture is suspected but radiographs are normal
- Detects incomplete fractures, bone bruise, and soft tissue damage
CT scan:
- Useful alternative when MRI is unavailable
- Helps identify comminution, lateral wall status, and fracture pattern
- A traction view can elucidate fracture location and lateral wall status

Anatomy of Relevance
- The trochanteric region contains cortical and cancellous bone
- The calcar femorale (Adam's arch) - a strong plate of posteromedial cortical bone - is the key structural element; it is most affected with posteromedial comminution
- Ward's triangle is a relatively weaker trabecular zone; peripheral to it, the structure transitions to the femoral medullary canal
- With aging, cortical bone thins and the calcar becomes weaker
Management
Preoperative Optimization
The following should be addressed rapidly:
- Correct anemia, dehydration, electrolyte imbalance, cardiac and respiratory issues
- Anticoagulation management: Surgery should NOT be postponed for aspirin. For warfarin, reversal is debated but urgent surgery with intraoperative bleeding measures is acceptable for some. For DOACs, delay 1-2 days depending on renal function
- VTE prophylaxis: LMWH is standard; continue for at least 28 days postoperatively; start 12 hours post-wound closure
- Preoperative traction is no longer routinely recommended (no benefit in pain reduction; complicates nursing care)
Timing of Surgery
- Surgery should be performed as soon as possible, ideally within 24 hours once the patient is medically optimized
- British Hip Fracture Database data: 30-day mortality increases 10% after a 24-hour delay
- The HIP ATTACK trial found no advantage of accelerated surgery (median 6 hours) over standard care (median 24 hours) on mortality
Anesthesia
- Both regional (spinal) and general anesthesia are acceptable with equal mortality profiles
- Regional anesthesia is preferred when possible due to fewer pulmonary complications
- Femoral nerve block or fascia iliaca compartment block (ultrasound-guided) is recommended to reduce opioid use and postoperative delirium
Surgical Treatment
Internal Fixation
1. Sliding Hip Screw (Dynamic Hip Screw - DHS):
- The standard for stable (A1, A2) fractures with an intact lateral wall
- A large lag screw in the femoral head slides within a barrel on the plate, allowing controlled fracture collapse
- Avoids stress risers, allows some impaction at the fracture site
2. Cephalomedullary (Intramedullary) Nail:
- Indicated for: A3 (reverse oblique) fractures, unstable fractures, subtrochanteric extension, and when DHS is contraindicated
- A nail inserted down the medullary canal with a proximal lag screw into the femoral head
- Superior mechanical advantage in A3 fractures; associated with better outcomes in unstable patterns
- The tip-to-apex distance (TAD) should be <25 mm to minimize risk of lag screw cutout

3. Percutaneous Compression Plate (PCCP):
- A sliding hip screw variant with smaller incision; theoretical advantages for lateral wall insufficiency
- Outcomes similar to SHS/IMN but technique more demanding
4. Proximal Femoral Locking Plate:
- NOT recommended as primary treatment for standard trochanteric fractures
- High failure rates due to static (non-collapsing) fixation
- May have a role in younger patients with complex fractures and good bone stock
Implants NOT recommended:
- 95-degree condylar plate / blade plate - static fixation, high failure rate, replaced by cephalomedullary nails
Fracture Reduction (Key Principles)
- Patient placed supine on fracture table with injured leg in traction
- Reduction to anatomical or slight valgus position - associated with lowest implant cutout risk
- Varus position must be avoided - mechanically unstable, leads to progressive varus and implant cutout
- Lateral view reduction is equally important - translation or angulation must be corrected
Complications
| Complication | Notes |
|---|---|
| Implant cutout | Most common fixation failure; associated with varus reduction, high TAD, poor bone quality |
| Non-union | Less common than in femoral neck fractures |
| Malunion (shortening/external rotation) | More common with unstable patterns |
| DVT/PE | Requires prophylaxis |
| Pneumonia | Common postoperative complication in elderly |
| Delirium | Perioperative; reduced by regional anesthesia and fascia iliaca blocks |
| Pressure sores | Risk in immobile patients |
| Second hip fracture | Up to 1-in-3 within 1.5 years |
Nonoperative Treatment
Reserved for:
- Non-ambulatory patients (e.g., nursing home patients) where surgery risk is prohibitive
- Management: symptomatic analgesia; Buck's traction intermittently for pain control; mobilize to sitting within 2-3 days
- Even nondisplaced fractures are at high risk for displacement with minimal activity (rolling in bed)
Key Contrasts with Femoral Neck Fracture
| Feature | Intertrochanteric | Femoral Neck |
|---|---|---|
| Location | Between trochanters (extracapsular) | At femoral neck (intracapsular) |
| Blood supply risk | Low | High (AVN risk) |
| Typical history | Tripping/direct fall onto hip | Sudden giving-way without obvious trip |
| Surgical treatment | Internal fixation (DHS/nail) | Hemiarthroplasty or cannulated screws |
| Union rate | High | Lower (AVN/non-union risk) |
Sources: Rockwood and Green's Fractures in Adults, 10th ed. 2025; Grainger & Allison's Diagnostic Radiology; Pfenninger and Fowler's Procedures for Primary Care, 3rd ed.
This is a shared conversation. Sign in to Orris to start your own chat.