CVP monitoring for MD anaesthesia exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have a comprehensive data set. Let me compile the full, exam-focused answer.
CVP Monitoring - MD Anaesthesia Exam Guide
Sources: Miller's Anesthesia 10e, Barash's Clinical Anesthesia 9e, Fishman's Pulmonary Diseases, Tintinalli's Emergency Medicine, Pye's Surgical Handicraft
1. Definition and Physiology
Central venous pressure (CVP) is the blood pressure within the superior vena cava / right atrium. It represents right atrial pressure and is used as an approximation of right ventricular preload (end-diastolic pressure).
CVP is determined by the interplay of:
- Mean circulatory filling pressure (MCFP) - the driving pressure for venous return (~8-10 mmHg)
- Venous return - inversely related to CVP per Guyton's model
- Right ventricular function - compliance, inotropy
- Intrathoracic/pericardial pressure
Normal CVP: 2-8 mmHg (or approximately 3-10 cmH₂O). Healthy resting value is 2-3 mmHg.
The difference between MCFP and CVP is only 6-8 mmHg, so small changes in CVP can have profound haemodynamic consequences. - Miller's Anesthesia, p. 4802
2. The CVP Waveform
This is the single most important topic for the exam. The CVP waveform reflects mechanical events of the cardiac cycle.
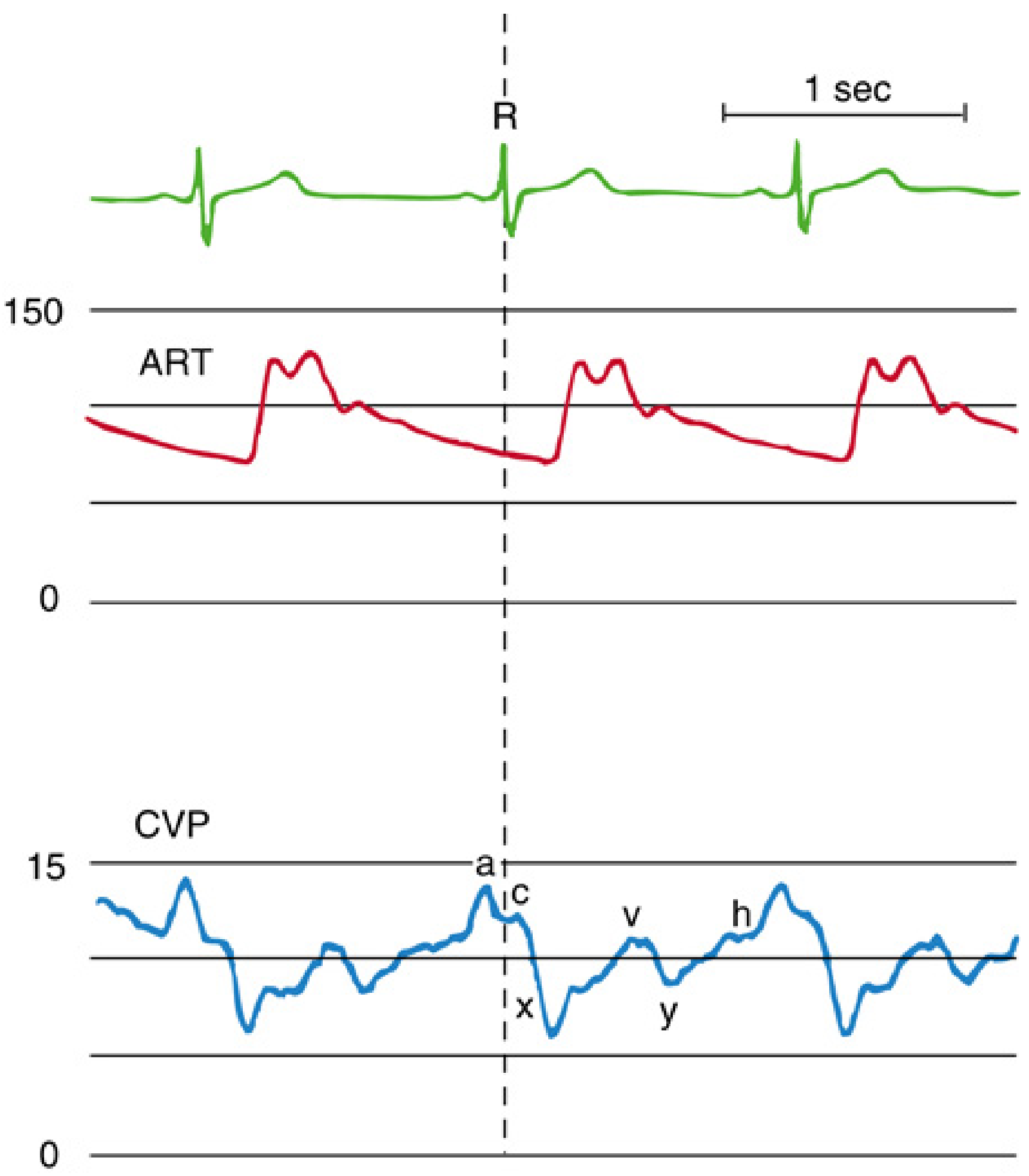
Normal CVP waveform (blue) with ECG (green) and arterial trace (red). The R wave marks end-diastole/onset of systole.
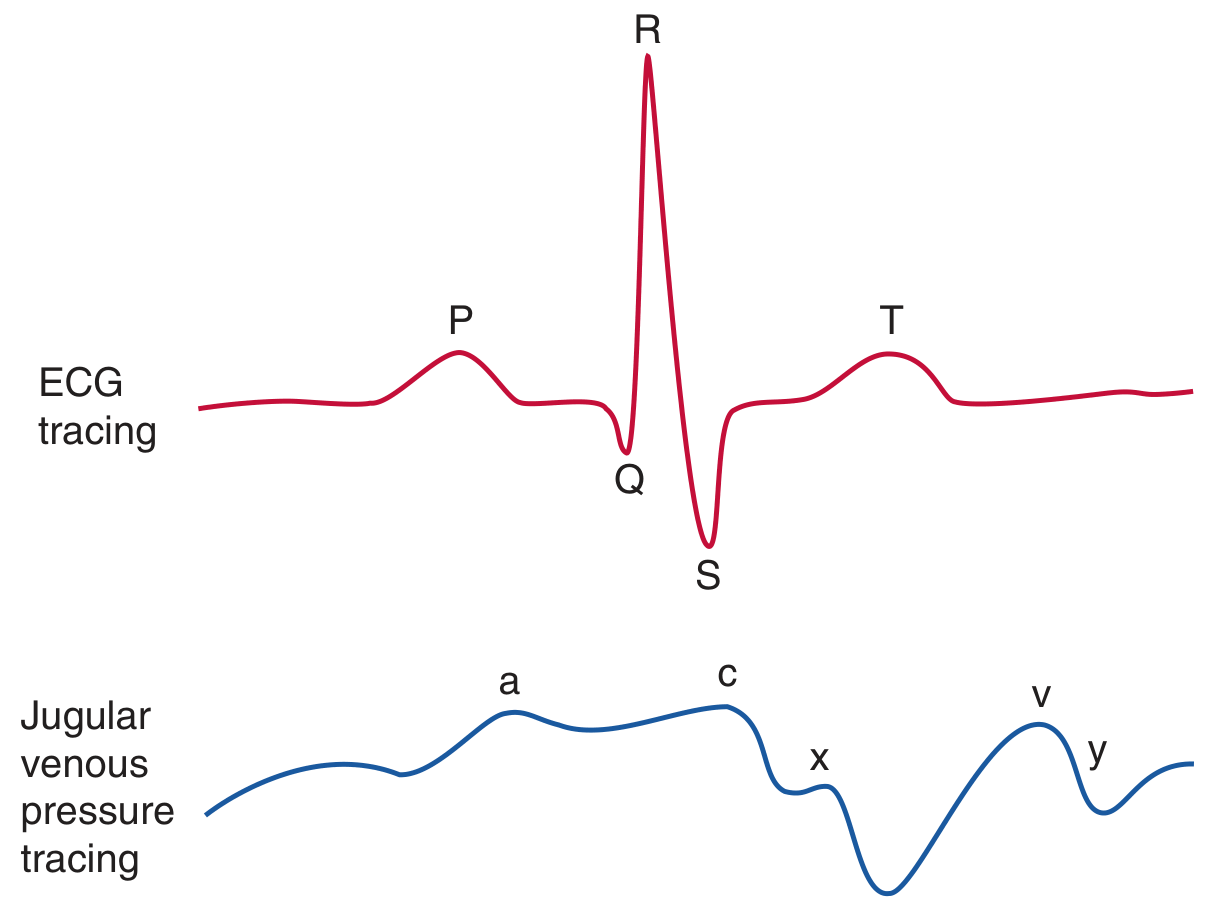
CVP (jugular venous pressure) tracing correlated with ECG
Waveform Components
| Component | Phase | Mechanical Event | ECG Timing |
|---|---|---|---|
| a wave | End-diastole | Atrial contraction | After P wave |
| c wave | Early systole | Isovolumic ventricular contraction; tricuspid valve bulges into RA | End of QRS |
| x descent | Mid-systole | Atrial relaxation + descent of the base ("systolic collapse") | Before T wave |
| v wave | Late systole/isovolumic relaxation | Passive atrial filling while tricuspid is closed | End of T wave |
| y descent | Early diastole | Tricuspid opens; blood flows into RV ("diastolic collapse") | Before next P wave |
| h wave | Mid-late diastole | Diastolic plateau (seen only at slow heart rates) | - |
Key exam point: The waveform has 3 systolic components (c wave, x descent, v wave) and 2 diastolic components (y descent, a wave). - Miller's Anesthesia, p. 4809
How to time the waveform: Always use the ECG R wave (not the arterial trace) to mark onset of systole. The arterial pressure upstroke is delayed ~200 ms after the ECG R wave (due to conduction, isovolumic contraction, aortic pressure transmission). - Miller's Anesthesia, p. 4809
Where to measure CVP: At the base of the c wave at end-expiration. - Fishman's, p. 2592
3. Abnormal CVP Waveforms
This is a high-yield exam topic.
| Condition | Waveform Change | Explanation |
|---|---|---|
| Atrial fibrillation | Loss of a wave; prominent c wave | No organised atrial contraction; greater atrial volume at end-diastole |
| AV dissociation (nodal rhythm, VT, VP pacing) | Cannon a waves | Atrium contracts against closed tricuspid valve |
| Tricuspid regurgitation | Tall systolic c-v wave; loss of x descent | Systolic RA filling through incompetent valve; CVP "ventricularised" |
| Tricuspid stenosis | Tall a wave; attenuated y descent | Increased resistance to atrial emptying |
| Cardiac tamponade | Dominant x descent; attenuated y descent | Pericardial fluid prevents diastolic filling |
| Pericardial constriction / RV ischaemia | Tall a and v waves; steep x AND y descents; M or W configuration | Rapid early filling then abrupt halt |
- Miller's Anesthesia, Table 32.4, p. 4811-4813
4. Indications for CVP Monitoring
From Miller's Anesthesia Box 32.5:
- CVP/haemodynamic monitoring in haemodynamically unstable patients
- Major surgery (cardiac, hepatic, vascular, trauma)
- Administration of concentrated vasoactive drugs or hyperalimentation
- Rapid fluid infusion (large cannulas)
- Transvenous cardiac pacing
- Temporary haemodialysis
- Aspiration of venous air emboli
- Pulmonary artery catheterisation (PAC)
- When peripheral IV access is unavailable
5. Cannulation Sites
| Site | Advantages | Disadvantages |
|---|---|---|
| Right internal jugular (IJV) | Most direct route to RA/RV; preferred for CVP monitoring and transvenous pacing; low pneumothorax risk | Carotid artery nearby; neck movement |
| Left IJV/external jugular | Alternative if right unavailable | Longer catheter length needed (3-5 cm more); tortuous path |
| Subclavian | Comfortable for patient; lower infection risk | Highest pneumothorax risk; non-compressible - avoid in coagulopathy |
| Femoral | Easy access; no pneumothorax risk; useful in trauma with cervical immobilisation | Highest thrombosis rate (~21.5%); infection risk; poor CVP reflection |
Key rules:
- Coagulopathy: prefer IJV or EJV (compressible)
- Severe emphysema: IJV over subclavian (pneumothorax risk)
- Emergency transvenous pacing: right IJV (most direct to RV)
- Trauma with hard collar: femoral or subclavian
- Catheter tip position: SVC/RA junction - confirm with CXR
Ultrasound guidance is now strongly recommended, especially for IJV cannulation. - Miller's Anesthesia, p. 4793
6. Setting Up and Zeroing
- Transducer zeroed to atmospheric pressure
- Referenced to the phlebostatic axis (4th intercostal space, mid-axillary line) - approximates right atrial level
- Read at end-expiration to eliminate respiratory pressure variation
- During spontaneous breathing: inspiration lowers CVP (negative pleural pressure transmitted)
- During positive pressure ventilation (IPPV): inspiration raises CVP (positive intrathoracic pressure transmitted)
- PEEP increases measured CVP but does not increase transmural pressure - can overestimate preload
7. CVP and Fluid Responsiveness - The Critical Concept
This is the most tested modern topic.
CVP is a poor predictor of fluid responsiveness and volume status. Multiple studies have failed to demonstrate a reliable relationship between CVP and intravascular blood volume or cardiac output response to fluids. Consensus guidelines recommend against using static CVP to guide fluid resuscitation. - Miller's Anesthesia p. 4803, Barash 9e, Fishman's
Why CVP is unreliable:
- The same CVP can result from very different ventricular preloads depending on compliance (flat vs. steep part of the diastolic pressure-volume curve)
- Myocardial ischaemia shifts the diastolic curve - CVP may rise while preload falls
- Changes in venomotor tone (catecholamines, vasoconstrictors) alter MCFP and thus CVP independently of volume
- Intrathoracic and pericardial pressure changes affect transmural (true distending) pressure, which is not measured
CVP still has a role:
- Extremes of CVP (very low = likely hypovolaemia; very high = likely RV failure or obstruction) remain clinically useful
- In differentiating shock types: distributive/hypovolaemic shock - low CVP; obstructive shock - high CVP
- Trending response to a fluid challenge - the direction of change matters more than the absolute value
Preferred alternatives for fluid responsiveness assessment:
- Pulse pressure variation (PPV) / systolic pressure variation (SPV)
- Stroke volume variation (SVV)
- IVC collapsibility index on ultrasound
- Passive leg raise + cardiac output response
- Transoesophageal echocardiography (TOE/TEE)
8. Complications of CVC Insertion
Categorised as Mechanical, Thromboembolic, Infectious - Miller's Anesthesia Box 32.6
Mechanical
- Arterial puncture (most common acute complication: 1.9-15%)
- Pneumothorax (subclavian > IJV; ~1.5% subclavian, ~0.5% IJV)
- Haemothorax, hydrothorax, hydromediastinum
- Air embolism
- Cardiac tamponade
- Arrhythmias
- Nerve injury (brachial plexus, phrenic, stellate ganglion, vocal cords)
Thromboembolic
- Catheter-related DVT: femoral ~21.5%, subclavian ~1.9%
- Pulmonary embolism
- SVC syndrome (if thrombus forms at catheter tip)
Infectious
- CLABSI (Central Line-Associated Bloodstream Infection) - most common late complication
- CLABSI rates fell ~50% from 2008-2016 with evidence-based bundle care
- Bundle: hand hygiene, maximal barrier precautions, chlorhexidine skin prep, optimal site selection, daily review of line necessity
9. CVP in Specific Clinical Contexts (Anaesthesia)
| Context | CVP Target / Role |
|---|---|
| Hepatic resection (liver surgery) | Low CVP (< 5 mmHg) maintained during parenchymal transection to reduce blood loss from hepatic veins |
| Cardiac surgery | Used alongside TOE, PA catheter; CVP reflects RV filling |
| Venous air embolism | CVP catheter allows aspiration of air; sudden rise in CVP may indicate venous air entry |
| Septic shock | CVP target of 8-12 mmHg was part of original Surviving Sepsis Campaign "bundles" but is no longer recommended as the primary target |
| Cardiac tamponade | High CVP + equalization of pressures; dominant x descent, attenuated y descent on waveform |
| Right heart failure | Elevated CVP; large v waves if tricuspid regurgitation |
10. Quick Summary Table for Exam
| Parameter | Value |
|---|---|
| Normal CVP | 2-8 mmHg (2-3 mmHg in healthy individuals) |
| Normal JVP equivalent | 3-10 cmH₂O |
| Phlebostatic axis | 4th ICS, mid-axillary line |
| Read at | End-expiration, base of c wave |
| Preferred cannulation site | Right IJV |
| Ultrasound guidance | Strongly recommended (IJV mandatory) |
| Fluid responsiveness predictor | Poor - do not use alone |
| Better dynamic predictors | PPV, SVV, PLR, IVC collapsibility, TOE |
Key exam pitfalls to avoid:
- Stating CVP reliably predicts fluid responsiveness - it does not
- Forgetting that IPPV and PEEP raise measured CVP but do not increase transmural distending pressure
- Confusing timing: a wave = after P; c wave = end of QRS; v wave = end of T wave
- Missing cannon a waves as a sign of AV dissociation (nodal rhythm, VT, pacing)
- Forgetting subclavian is non-compressible - avoid in coagulopathy
This is a shared conversation. Sign in to Orris to start your own chat.