Teach Teach me thyroid surgery at the level of neat pg
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content from Schwartz's, Sabiston, and K.J. Lee's Otolaryngology textbooks, along with excellent surgical illustrations. Let me compile the complete PG-level teaching note.
Thyroid Surgery - Complete PG-Level Teaching Note
Sources: Schwartz's Principles of Surgery 11e, Sabiston Textbook of Surgery, K.J. Lee's Essential Otolaryngology, Cummings Otolaryngology
1. Historical Context (Exam Favourite)
- First thyroidectomy: Abu al-Qasim (952 AD) - for endemic goiter, nearly fatal from blood loss
- Term "thyroid" coined by Thomas Wharton (1646) - from Greek thyreos (shield)
- Theodor Kocher = "Father of modern thyroid surgery" - performed >5000 thyroidectomies, mortality 0.5%, won Nobel Prize in Medicine/Physiology 1909 (first Nobel to a surgeon)
- Thomas Dunhill pioneered the bilateral operation: unilateral total lobectomy + contralateral subtotal resection for thyrotoxicosis ("Dunhill's operation")
- Pre-Kocher era: French Academy of Medicine banned thyroid surgery due to 40%+ mortality
2. Indications for Thyroidectomy
| Category | Examples |
|---|---|
| Hyperthyroidism | Graves disease (failed medical/RAI), toxic multinodular goiter, toxic adenoma |
| Goiter | Compressive goiter (dysphagia, dyspnea, SVC syndrome), substernal goiter |
| Thyroid nodules | Bethesda IV-VI on FNA, large nodules with indeterminate cytology |
| Thyroid cancer | DTC (papillary, follicular), MTC, anaplastic, lymphoma failing chemo |
| Cosmetic/Patient preference | After informed discussion |
3. Extent of Thyroid Resection - Definitions
| Operation | Definition |
|---|---|
| Total thyroidectomy | All visible thyroid excised |
| Near-total thyroidectomy | <1 g remnant left at ligament of Berry (to protect RLN) |
| Subtotal thyroidectomy | 3-5 g remnant left (protects RLN + parathyroids + avoids T4 replacement); less common now |
| Thyroid lobectomy (hemithyroidectomy) | One lobe + isthmus + pyramidal lobe |
| Dunhill operation | Total on one side + subtotal on other - for bilateral disease (Graves) |
| Isthmusectomy | Isthmus + pyramidal lobe only (tracheal/midline pathology) |
Current practice: Vast majority = total thyroidectomy or lobectomy. Over 130,000 thyroidectomies/year in the USA.
4. Surgical Anatomy - The Critical Structures
The Recurrent Laryngeal Nerve (RLN) - THE most important structure
| Feature | Left RLN | Right RLN |
|---|---|---|
| Loop around | Aortic arch (ligamentum arteriosum) | Right subclavian artery |
| Course | Straight, in tracheoesophageal groove | More oblique (laterally angled) |
| Non-recurrent variant | Never | ~1% of cases (right-sided aortic arch/aberrant subclavian) - HIGH RISK |
Key landmarks to find the RLN:
- Most consistently found at the level of the cricoid cartilage
- Identified medial to the Tubercle of Zuckerkandl (posterior thyroid tubercle)
- Just below the ligament of Berry and its laryngeal entry point
- White, wave-like structure with characteristic vascular stripe
- Extralaryngeal branching occurs in ~1/3 of patients above the crossing point with inferior thyroid artery
Ligament of Berry (suspensory ligament): The RLN is most vulnerable HERE. Small crossing arteries and veins run through it. Electrocautery is contraindicated in this zone - use gentle pressure, careful ligation only.
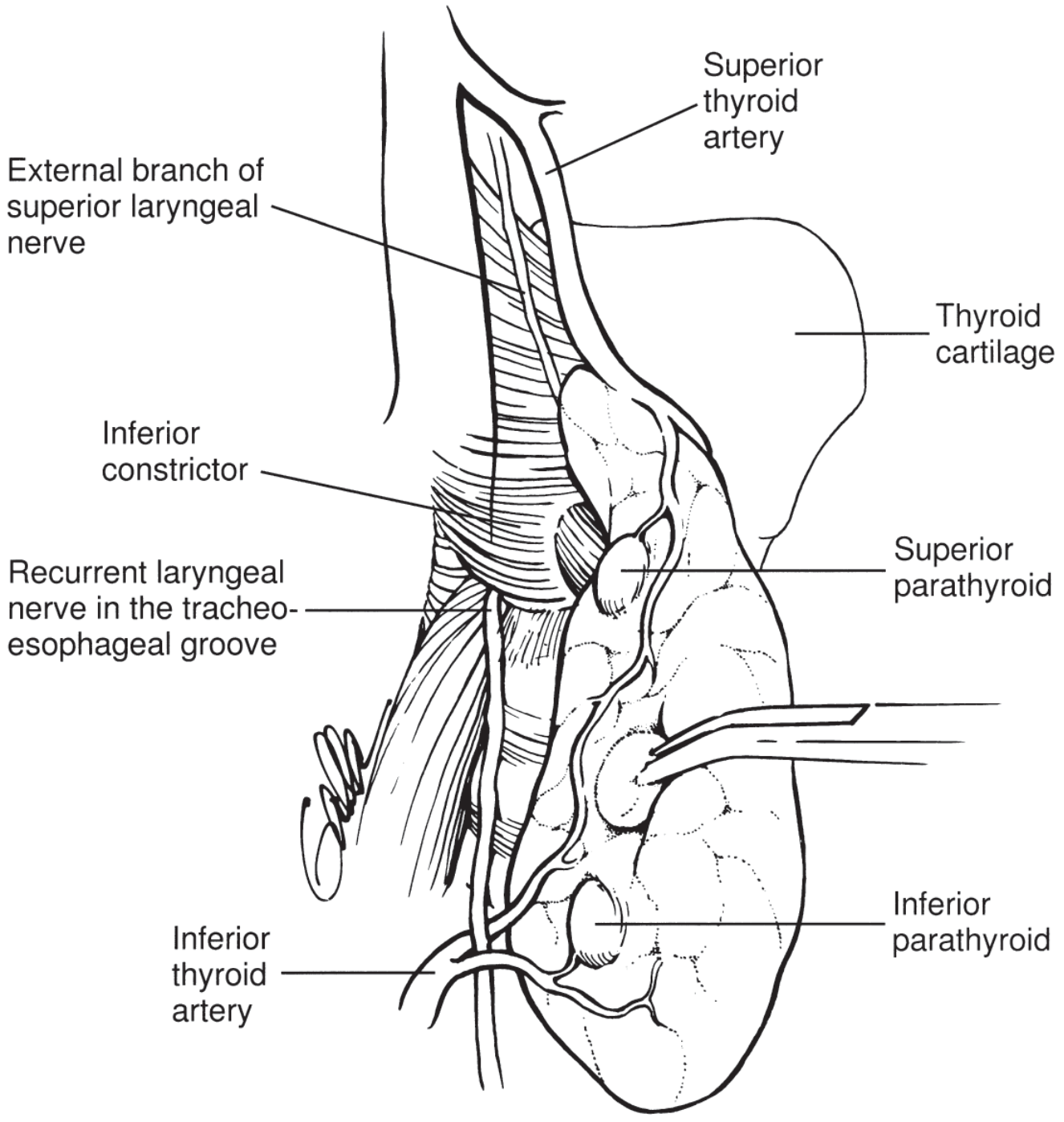
The External Branch of the Superior Laryngeal Nerve (EBSLN)
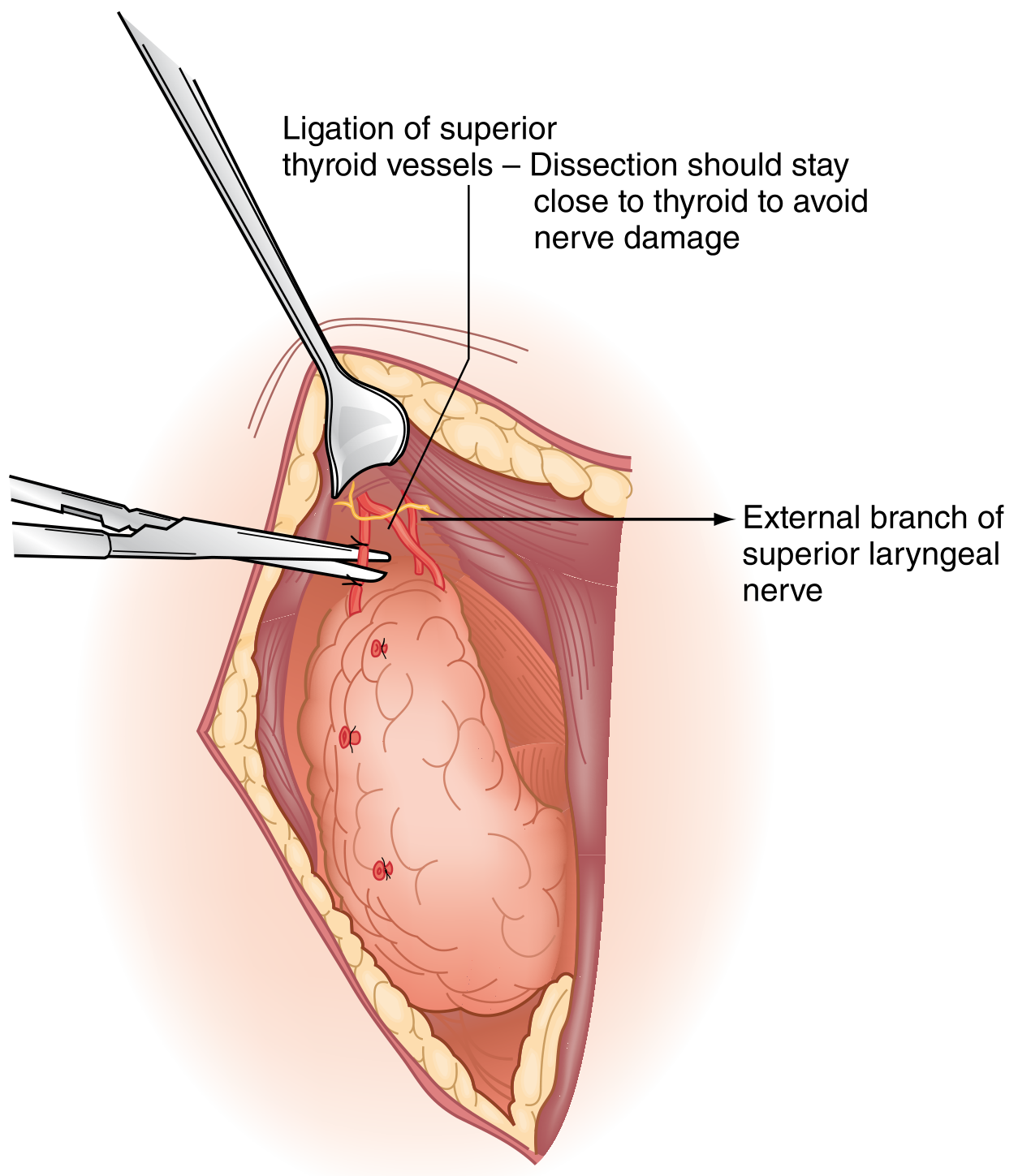
- Runs along cricothyroid muscle just medial to the superior pole vessels
- Vulnerable in ~20% of cases where it is at the level of the thyroid capsule
- Injury = loss of high-pitched phonation (cricothyroid muscle innervation) - career-ending for singers
- Avoidance: ligate superior pole vessels individually and as close to the thyroid capsule as possible
- The space of Reeves = avascular space between medial superior pole and cricothyroid muscle - use this for safe dissection
The Parathyroid Glands
| Gland | Location | Relationship to ITA/RLN |
|---|---|---|
| Superior | Posterior mid-thyroid, at level of cricoid cartilage | Posterior to RLN, above ITA crossing |
| Inferior | Less constant; near inferior pole, often adherent posterolaterally | Anterior to RLN, below ITA crossing |
- Located within 1 cm of the crossing of inferior thyroid artery and RLN
- Always ligate branches of inferior thyroid artery close to the thyroid capsule (not the main trunk) to preserve parathyroid blood supply
- If a parathyroid is devascularized (turns black): biopsy to confirm with frozen section → mince into 1mm fragments → autotransplant into multiple pockets in sternocleidomastoid muscle; mark pockets with silk + clip
5. Preoperative Preparation
- TFTs + TSH - ensure euthyroid (for hyperthyroidism: antithyroid drugs ± β-blockers; Graves: Lugol's iodine/SSKI 10 days before surgery for vascularity reduction)
- Neck ultrasound (all patients)
- FNA biopsy as indicated
- Vocal cord assessment (laryngoscopy): Mandatory in:
- Any voice changes or prior cervical/chest surgery
- Thyroid cancer with posterior extrathyroidal extension or bulky nodal metastases
- Up to 3.5% of benign disease and 8% of cancer patients have preop vocal cord dysfunction (can be silent in 20%!)
- AAES guidelines: noninvasive voice assessment for ALL; selective laryngoscopy based on risk
- Transcutaneous laryngeal ultrasound - emerging non-invasive alternative (sensitivity/specificity 93-100%)
- Serum calcium: check if concurrent primary hyperparathyroidism suspected (MEN2A)
6. Operative Technique - Step by Step
Positioning
- Supine, both arms tucked
- Back raised 20 degrees, neck extended by soft roll behind scapulae
- Head on foam/gel ring - brings thyroid gland to maximal exposure
Incision
- Kocher collar incision: horizontal, 3-5 cm (may need longer), placed 1 cm below the cricoid cartilage, in or parallel to a natural skin crease (Langer's lines) - ensures cosmetic scar
Step 1: Raising Flaps
- Subcutaneous tissue + platysma incised sharply
- Subplatysmal flaps raised superiorly to the level of thyroid cartilage, inferiorly to suprasternal notch
- Strap muscles divided in the midline (entire length)
Step 2: Strap Muscle Elevation
- Sternohyoid (medial) + sternothyroid (lateral) elevated off ventral thyroid surface as one layer
- Blunt dissection until internal jugular vein and ansa cervicalis identified
- Strap muscles rarely need to be divided - if needed, divide HIGH to preserve ansa cervicalis innervation
- If tumor invades strap muscles → en-bloc resection
Step 3: Middle Thyroid Vein Division
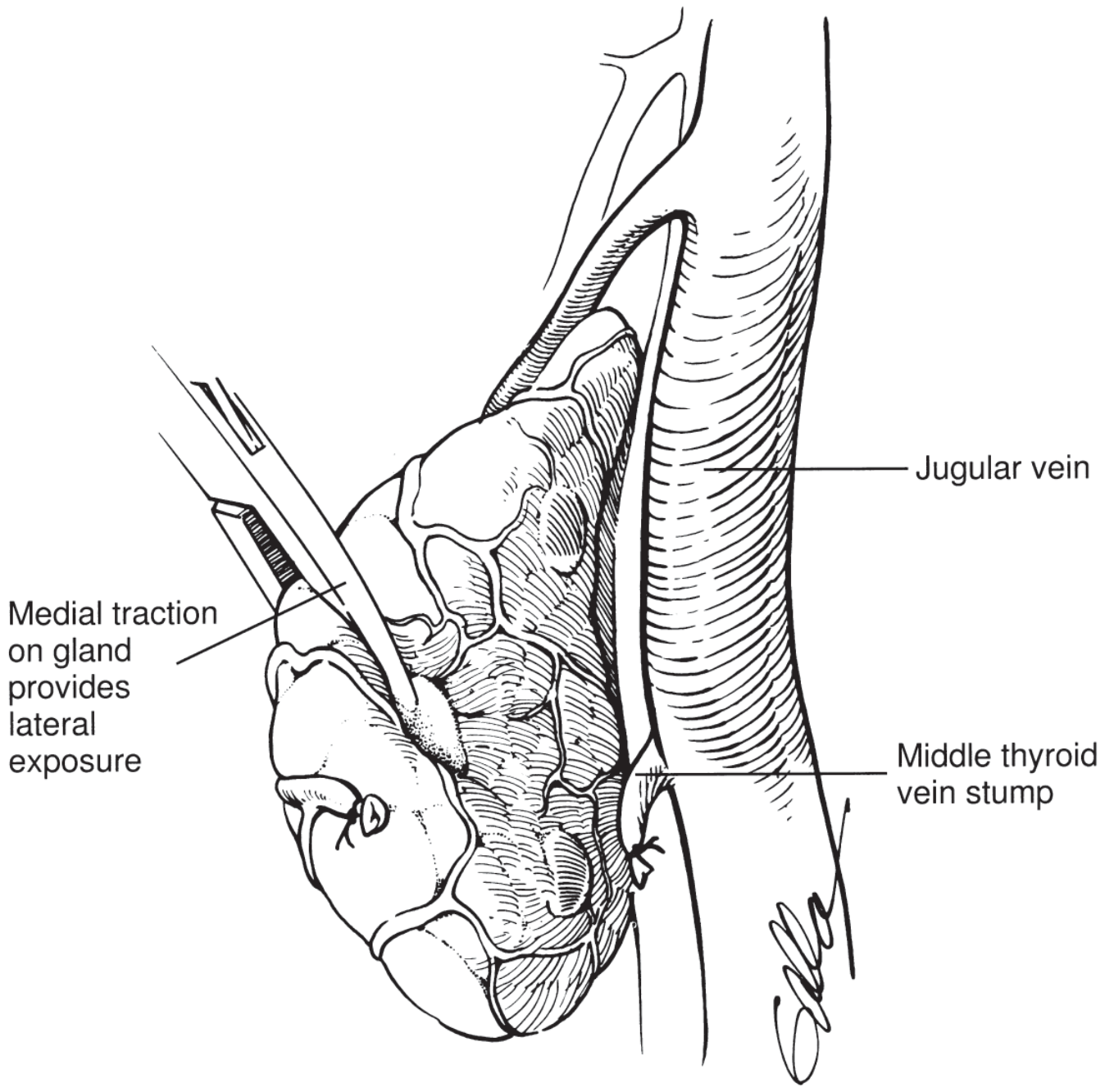
- Thyroid lobe retracted medially and anteriorly
- Lateral tissues swept posterolaterally with peanut sponge
- Middle thyroid vein ligated and divided → provides lateral exposure of mid lobe
Step 4: Superior Pole Dissection
- Retract thyroid inferiorly and medially first
- Then retract upper pole downward and laterally to expose cricothyroid space
- Superior pole vessels individually isolated, ligated, and divided individually, close to thyroid capsule (to protect EBSLN)
- Use space of Reeves for safe medial dissection of superior pole
- Filmy tissues swept away from posterior superior pole by blunt dissection
- Superior parathyroid often identified here at level of cricoid
Step 5: RLN Identification (MANDATORY)
- ATA 2015 guidelines: visual identification of RLN in ALL cases
- Identify at the level of the cricoid, where it is most consistent
- Confirm with intraoperative neuromonitoring (IONM) using endotracheal tube electrodes
- Right RLN: more oblique course - keep in mind non-recurrent variant on the right!
- Use IONM: stimulate vagus nerve AND RLN before, during, and after resection
Step 6: Inferior Pole Mobilization
- Inferior thyroid lobe grasped with Allis/large Kelly clamp, retracted anteromedially
- Inferior pole vessels ligated and divided
- Lymphoadipose tissues dissected off lateral thyroid
- Inferior parathyroid identified (anterior to RLN, inferior to ITA crossing)
- Ligate branches of inferior thyroid artery close to thyroid capsule
Step 7: Ligament of Berry and Tracheal Separation
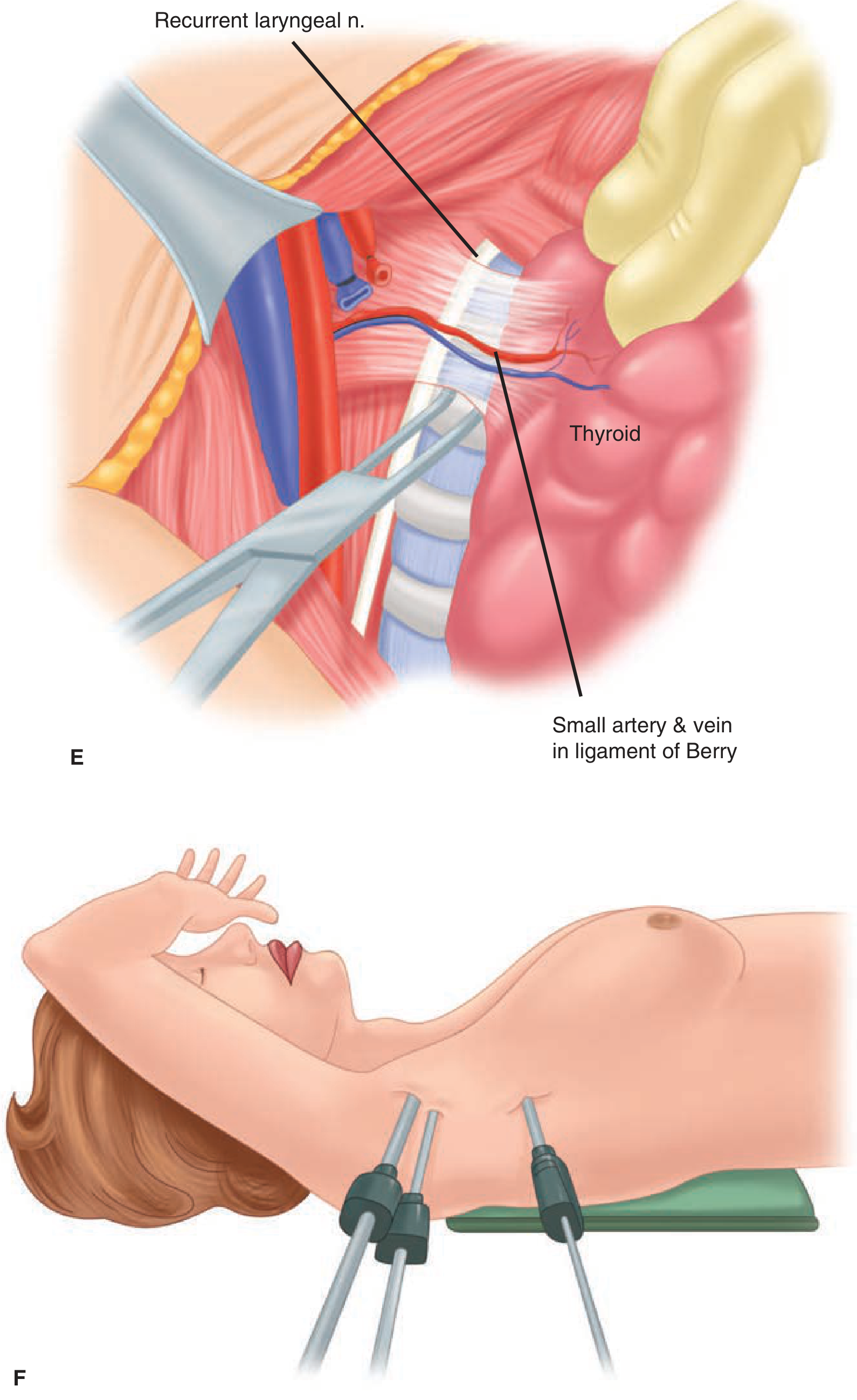
- RLN most vulnerable here
- Bleeding in this area: control with gentle pressure only, then carefully ligate the vessel
- No electrocautery near the RLN!
- Once ligament divided, thyroid separated from trachea by sharp dissection
- Pyramidal lobe: dissect cephalad to above the notch in thyroid cartilage (or above)
Step 8: Completion and Closure
- For lobectomy: isthmus clamped, divided, and suture-ligated on the tracheal side
- For subtotal thyroidectomy: Mayo clamp across lobe, leaving ~4 g of posterior thyroid; suture-ligate remnant
- Devascularized parathyroids: autotransplant to SCM pockets
- Routine drain placement rarely necessary
- Strap muscles reapproximated in midline
- Platysma approximated
- Skin: subcuticular sutures or clips
7. Intraoperative Neuromonitoring (IONM)
- Contact electrodes on endotracheal tube detect EMG signals from vocal cords
- Two methods: intermittent (periodic stimulation) vs continuous (cuff electrode on vagus)
- Stimulate vagus + RLN before and after resection (loss of signal = nerve at risk)
- Barczynski 2009: prospective RCT of 2000 nerves - IONM reduced transient RLN injury rates
- Does not eliminate nerve injury but assists identification, especially in reoperations
- Can also identify and confirm EBSLN integrity
8. Complications - The Core PG Topic
A. Recurrent Laryngeal Nerve Injury
| Type | Incidence | Features |
|---|---|---|
| Transient paralysis | Up to 6% | Resolves within 6 months |
| Permanent paralysis | 0.5-2% | Unilateral: hoarseness; Bilateral: life-threatening stridor/aphonia requiring tracheostomy |
Causes of RLN injury:
- Inadvertent division (cutting)
- Traction/stretching during retraction
- Thermal injury from electrocautery or energy devices
- Ligature inclusion in suture
- Hematoma compression (delayed)
Unilateral RLN injury: Hoarseness, breathy voice, aspiration. Treat with voice therapy or medialization.
Bilateral RLN injury: Respiratory distress, stridor → emergent reintubation/tracheostomy
B. Hypoparathyroidism (Most Common Serious Complication)
| Type | Timing | Definition |
|---|---|---|
| Transient | Within 24-48 hrs | Serum Ca <8 mg/dL; resolves in 6 months |
| Permanent | >6 months | True deficiency requiring lifelong supplementation |
- Transient: up to 20-30% after total thyroidectomy
- Permanent: 1-2% after total thyroidectomy (higher in reoperations)
- Symptoms of hypocalcemia: perioral tingling, fingertip paresthesias, carpopedal spasm (Trousseau's sign), Chvostek's sign, seizures
- Management: IV calcium gluconate acutely; oral calcium + calcitriol (1,25-OH2-D3) long term
- PTH at 6-24 hours postop: near-undetectable PTH (<10 pg/mL) = high risk for permanent hypoparathyroidism
C. Postoperative Neck Hematoma (Surgical Emergency)
- Incidence: 0.1-1.1%
- Risk factors: male sex, advanced age, bilateral operation, Graves disease, anticoagulants
- Most (80%) occur within the first 6 hours postoperatively; 20% between 6-24 hours
- Danger: NOT blood loss per se, but tracheal compression → rapid airway compromise
- Presentation: pain, wound oozing, ecchymosis, firm neck swelling, stridor
- Management:
- Mild: OR under controlled anesthesia
- Impending airway collapse: open incision IMMEDIATELY at bedside (all 3 layers: skin + platysma + strap muscles)
- Always keep instruments at bedside postoperatively for this reason
D. EBSLN Injury
- Loss of high-pitched phonation, easy voice fatigue
- Particularly devastating for singers and public speakers
- Often underdiagnosed; reported as "voice changes" without formal laryngoscopy
E. Other Complications
| Complication | Notes |
|---|---|
| Thyroid storm | Especially in unprepared hyperthyroid patients |
| Tracheomalacia | In long-standing goiters; may need tracheostomy at operation |
| Chylous fistula | Left side; injury to thoracic duct |
| Keloid scar | Common concern in young women |
| Wound infection | Rare (<1%) |
9. Minimally Invasive / Alternative Approaches
| Approach | Details |
|---|---|
| Video-assisted thyroidectomy | Small collar incision + endoscope; cosmetically superior |
| Endoscopic via axillary | Remote access; avoids neck scar entirely |
| Robotic thyroidectomy | Transaxillary or retroauricular; growing in Asia; same oncologic outcomes |
| NOTES (Natural Orifice) | Transoral vestibular approach; scar-free; gaining traction |
10. Postoperative Management
- Serum calcium and PTH at 6-24 hours (especially after total thyroidectomy)
- Prophylactic oral calcium supplementation commonly given after total thyroidectomy
- Most cases can be done as day surgery (outpatient)
- Voice assessment at 2-4 weeks postop (compare with preop baseline)
- Thyroid hormone replacement after total thyroidectomy:
- Benign: T4 (levothyroxine) to maintain TSH in normal range
- DTC: suppressive T4 therapy (TSH <0.1 for high-risk; 0.1-0.5 for low-risk)
- Surgeon volume: outcomes improve up to 26 cases/year threshold (Nationwide Inpatient Sample study)
11. High-Yield PG Summary Points
| Point | Fact |
|---|---|
| Nobel Prize winner in thyroid surgery | Theodor Kocher (1909) |
| Most important step in thyroidectomy | Visual identification of RLN |
| Most vulnerable site for RLN injury | Ligament of Berry |
| Non-recurrent RLN | Right side (~1%), associated with aberrant right subclavian |
| Superior parathyroid relationship | Posterior to RLN |
| Inferior parathyroid relationship | Anterior to RLN |
| Most common serious complication | Hypoparathyroidism (transient) |
| Dreaded emergency post-thyroidectomy | Neck hematoma with airway compromise |
| To protect EBSLN | Ligate superior pole vessels close to capsule |
| Kocher incision placement | 1 cm below the cricoid cartilage |
| Subtotal thyroidectomy remnant | 3-5 g; near-total = <1 g |
| Autotransplant site for parathyroids | SCM (sternocleidomastoid) muscle pockets |
Sources: Schwartz's Principles of Surgery 11e (p.1686-1687), Sabiston Textbook of Surgery (pp.1521-1528), K.J. Lee's Essential Otolaryngology (pp.742-743)
This is a shared conversation. Sign in to Orris to start your own chat.