First generation anti allergic drugs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Lippincott Pharmacology and Fitzpatrick's Dermatology. Here is a thorough overview:
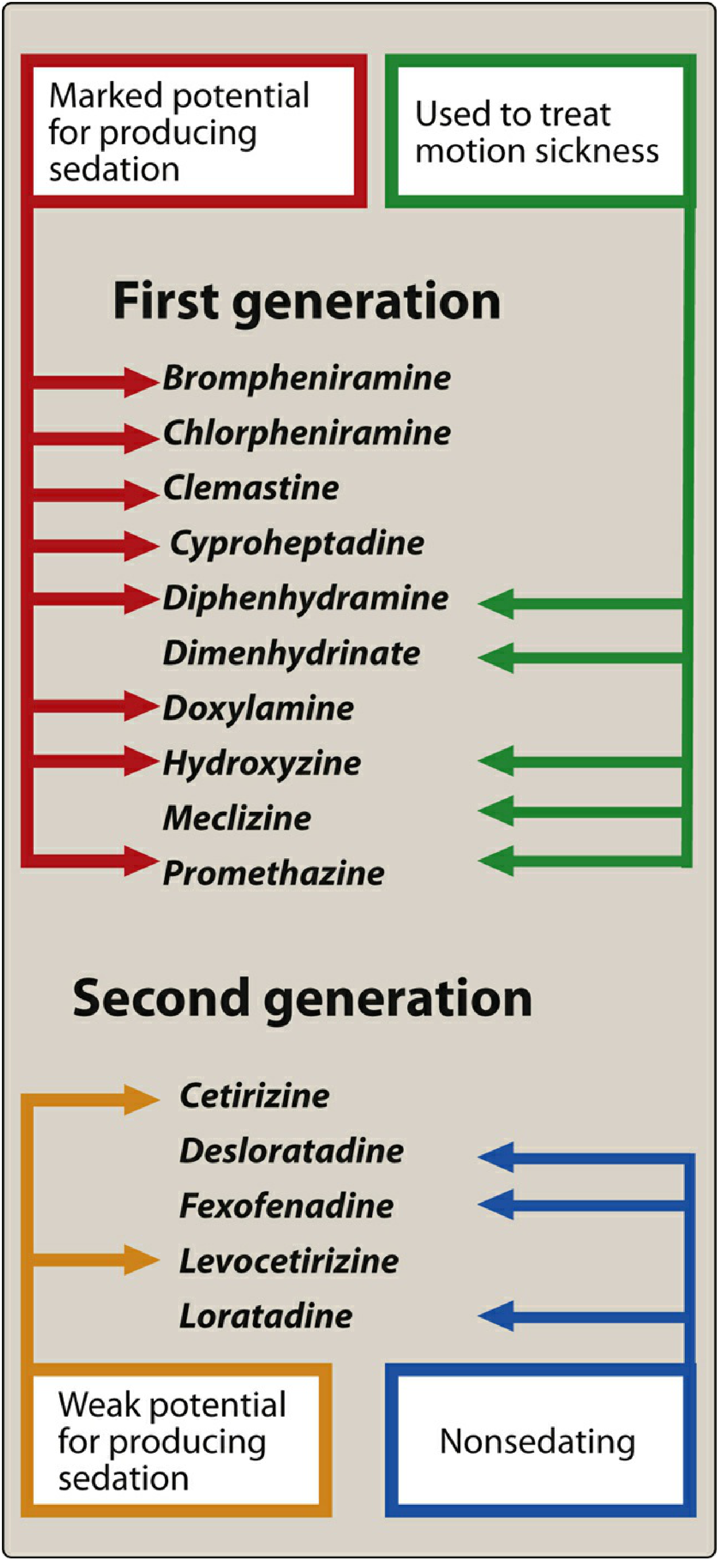
First-Generation (Sedating) Antihistamines — H1-Receptor Blockers
Overview
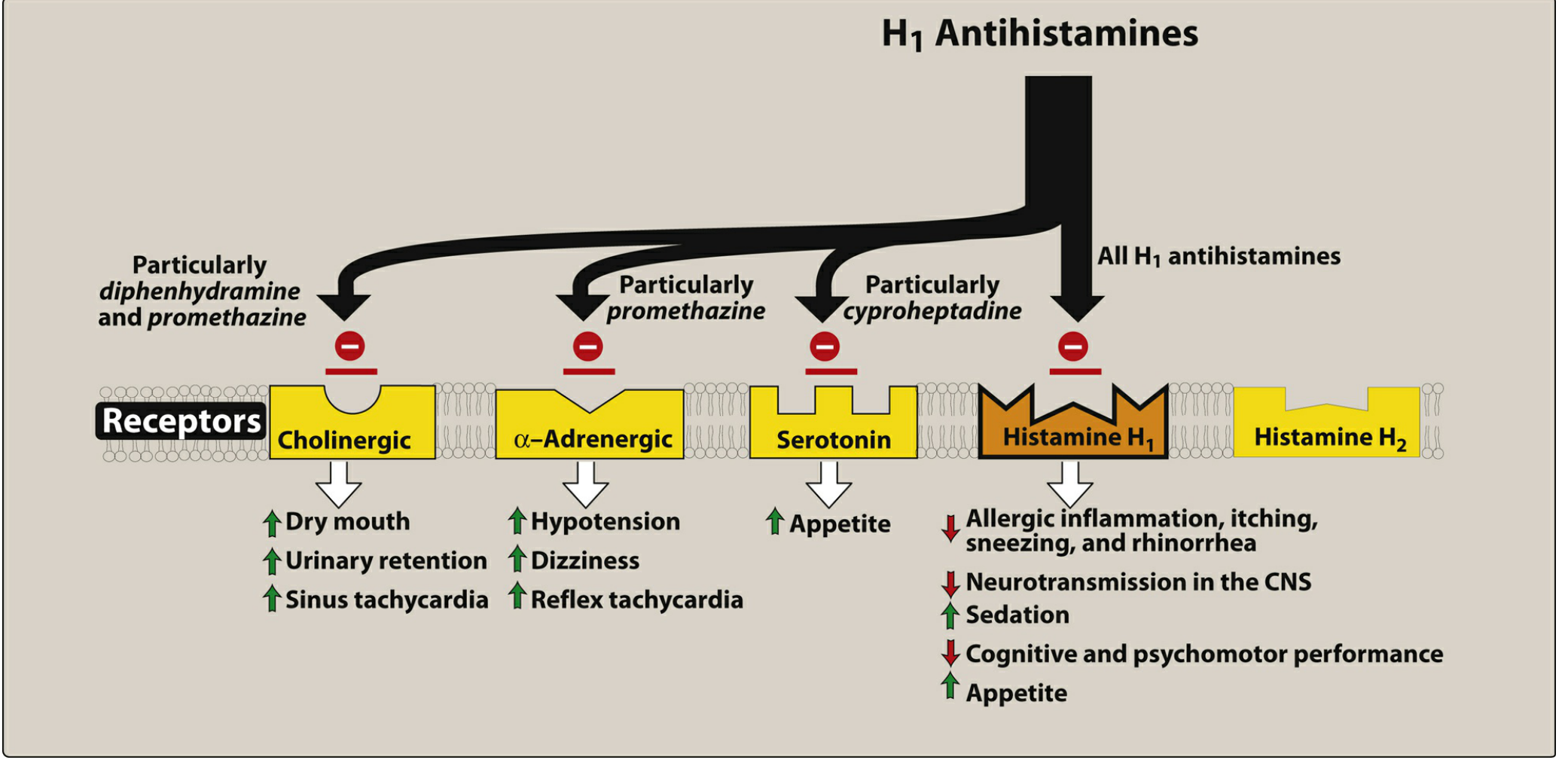
First-generation antihistamines are classic H1-receptor blockers that competitively block histamine at the H1 receptor. Unlike second-generation agents, they are lipophilic, readily cross the blood-brain barrier, and interact with multiple receptor types (cholinergic, adrenergic, serotonin) — the source of both their broader utility and their side effects.
Drugs (with chemical classes)
| Drug | Chemical Class | Notable Feature |
|---|---|---|
| Diphenhydramine | Ethanolamine | Prototype; strong sedation, antiemetic, motion sickness |
| Dimenhydrinate | Ethanolamine | Diphenhydramine + chlorinated theophylline; motion sickness |
| Doxylamine | Ethanolamine | OTC sleep aid; used in pregnancy nausea (with pyridoxine) |
| Chlorpheniramine | Alkylamine | Less sedating among 1st-gen; common in cold preparations |
| Brompheniramine | Alkylamine | Similar to chlorpheniramine |
| Hydroxyzine | Piperazine | Anxiolytic, antipruritic; half-life >20 hours |
| Meclizine | Piperazine | Motion sickness, vertigo |
| Promethazine | Phenothiazine | Antiemetic, sedation; also D2 antagonist |
| Clemastine | Ethanolamine | Used in allergic rhinitis |
| Cyproheptadine | Piperidine | Also a serotonin antagonist; used for appetite stimulation and serotonin syndrome |
| Azelastine | — | Topical (intranasal/ophthalmic); also has mast cell–stabilizing properties |
| Ketotifen | — | Mast cell–stabilizing + H1 blockade; ophthalmic use |
Mechanism of Action
- Competitive blockade at H1 receptors — do not prevent histamine release; they block the response at target tissue.
- More effective at preventing symptoms than reversing established reactions.
- Additional receptor interactions:
- Anticholinergic (muscarinic) blockade → dry mouth, urinary retention, blurred vision, constipation
- α-adrenergic blockade → postural hypotension
- Serotonin antagonism (cyproheptadine) → appetite stimulation, serotonin syndrome management
- Mast cell stabilization (azelastine, ketotifen) → additional anti-allergic benefit
Therapeutic Uses
- Allergic rhinitis & urticaria — drugs of choice for histamine-mediated symptoms (rhinorrhea, sneezing, pruritus, hives); do not relieve nasal congestion
- Motion sickness & nausea/vomiting — diphenhydramine, dimenhydrinate, meclizine, promethazine; block central H1 and M1 muscarinic receptors in the vestibular/chemoreceptor pathways; must be taken before exposure
- Insomnia — diphenhydramine and doxylamine are found in OTC sleep aids; tolerance to sedative effect develops quickly
- Vertigo — meclizine is preferred for vestibular disorders
- Pruritus — hydroxyzine is widely used; 1st-gen preferred over 2nd-gen for significant itching (e.g., eczema flares)
- Anaphylaxis (adjunct) — antihistamines are adjunctive only; epinephrine is the drug of choice
- Appetite stimulation — cyproheptadine (via serotonin antagonism)
- Serotonin syndrome — cyproheptadine as antidote
Antihistamines are NOT indicated for bronchial asthma because histamine is only one of several mediators responsible for bronchoconstriction.
Pharmacokinetics
- Oral absorption is rapid; onset of sedation within 30 minutes to 1 hour
- Sedation generally persists 4–6 hours, but may last 24 hours or longer for some agents
- Half-lives: brompheniramine, chlorpheniramine, and hydroxyzine >20 hours in adults
- Metabolized by hepatic CYP3A4 → glucuronide conjugates → excreted in urine
- Wheal-and-flare suppression can persist for up to 7 days after discontinuation despite short half-lives
- No tolerance to antihistamine effect over 3 months (only sedation tolerance develops)
Adverse Effects
| Category | Effects |
|---|---|
| CNS (sedation) | Drowsiness, dizziness, impaired cognition, fatigue |
| Other CNS | Tinnitus, blurred vision, irritability, insomnia (paradoxical excitation in children), tremor |
| Anticholinergic | Dry mucous membranes, urinary retention, constipation, postural hypotension, erectile dysfunction |
| Cardiac | QT prolongation, ventricular arrhythmias, torsades de pointes |
| GI | Nausea, vomiting, anorexia, diarrhea (uncommon; reduced by taking with food) |
Anticholinergic effects are especially common with ethanolamine, phenothiazine, and piperazine group agents.
Contraindications & Precautions
| Concern | Reason |
|---|---|
| Narrow-angle glaucoma | Anticholinergic effects raise intraocular pressure |
| Prostatic hypertrophy | Risk of urinary retention |
| MAO inhibitors (concurrent use) | Dangerous interaction |
| Cardiac arrhythmias | QT prolongation risk |
| First trimester of pregnancy | Embryotoxicity risk |
| Driving / hazardous work | Sedation impairs reaction time |
| Elderly patients | Increased anticholinergic burden; confusion, falls |
Why First-Generation Rather Than Second-Generation?
First-generation agents remain preferred in specific situations:
- When sedation is desired (sleep, anxiety, itch at night)
- Motion sickness (meclizine, promethazine, diphenhydramine)
- Severe acute pruritus (hydroxyzine)
- Cost considerations — effective and inexpensive
- Serotonin syndrome management (cyproheptadine)
Their main drawback is CNS penetration, which second-generation agents (cetirizine, fexofenadine, loratadine) avoid by being made polar and thus unable to cross the blood-brain barrier.
Sources: Lippincott Illustrated Reviews: Pharmacology, pp. 1309–1314 | Fitzpatrick's Dermatology, pp. 3482–3485
This is a shared conversation. Sign in to Orris to start your own chat.