Role of lung ultrasound in diagnosis of critical clinical conditions
Reading File
search_medical_text
lung ultrasound diagnosis critical conditions ICU emergency
search_medical_image
lung ultrasound findings pleural effusion pneumothorax B-lines consolidation
GradeResponse
GradeResponse
search_medical_text
lung ultrasound A-lines B-lines pneumothorax pleural effusion signs
search_medical_text
BLUE protocol lung ultrasound acute respiratory failure differential diagnosis
GradeResponse
Here is a comprehensive synthesis of the role of lung ultrasound (LUS) in diagnosing critical clinical conditions.
Lung Ultrasound in Critical Clinical Conditions
Lung ultrasound has emerged as one of the most powerful point-of-care tools in critical care and emergency medicine. Its portability, repeatability, absence of radiation, and bedside availability make it ideal for rapid assessment of the acutely deteriorating patient.
Why Lung Ultrasound Works
The lung is largely inaccessible to ultrasound under normal aeration because air reflects sound. However, pathological conditions alter the air-fluid ratio of lung tissue, generating characteristic ultrasound artifacts or real tissue images that are diagnostically specific. Understanding these artifacts is the foundation of LUS interpretation.
Core Ultrasound Signs
| Sign | Appearance | Significance |
|---|---|---|
| A-lines | Horizontal, equally spaced hyperechoic lines below the pleural line | Normal aeration or pneumothorax |
| B-lines (lung rockets) | Vertical hyperechoic lines arising from pleura, erasing A-lines, reaching the edge of screen | Interstitial syndrome (pulmonary edema, pneumonitis) |
| Lung sliding | Shimmering movement of visceral on parietal pleura with respiration | Normal; absence suggests pneumothorax |
| Seashore sign (M-mode) | Granular pattern deep to pleural line | Normal lung sliding present |
| Stratosphere/Barcode sign (M-mode) | Parallel horizontal lines throughout | Absent lung sliding — pneumothorax |
| Consolidation | Hypoechoic, tissue-like (hepatization); may contain air bronchograms | Pneumonia, atelectasis, contusion |
| Shred sign | Irregular, shredded deep border of consolidation | Subpleural pneumonia |
| Quad sign | Anechoic quadrilateral space bounded by pleura, lung, and ribs | Pleural effusion |
| Sinusoid sign | Oscillating movement of lung in effusion on M-mode | Confirms free-flowing effusion |
Diagnostic Applications in Critical Conditions
1. Pneumothorax
LUS is superior to supine chest X-ray for pneumothorax detection (sensitivity ~90% vs. ~50% for CXR in supine trauma patients — Chest, 2011; meta-analysis by Ding et al.).
Key findings:
- Absent lung sliding at the affected zone
- Absent B-lines
- A-lines present (air reverberation)
- Stratosphere/barcode sign on M-mode
- Lung point (transition between absent and present sliding) — pathognomonic for pneumothorax; 100% specific
If lung sliding is present, pneumothorax is effectively excluded at that probe location.
2. Pleural Effusion
LUS detects effusions with >90% sensitivity and specificity, far exceeding supine CXR. It can quantify volume and guide thoracentesis.
Key findings:
- Quad sign: anechoic (transudates) or echogenic/complex (exudates, hemothorax, empyema) collection above the diaphragm
- Sinusoid sign: lung oscillates within the effusion on M-mode
- Compressed/consolidated lung floating in effusion ("jellyfish sign")
Quantification: Several validated formulas use interpleural distance to estimate volume (Vignon et al., Crit Care Med 2005; Balik et al., Intensive Care Med 2006). LUS can reliably predict effusions >500 mL in mechanically ventilated patients (Roch et al., Chest 2005).
Procedure guidance: Ultrasound-guided thoracentesis significantly reduces pneumothorax risk compared to blind technique (Barnes et al., J Clin Ultrasound 2005).
3. Pulmonary Edema (Cardiogenic)
B-lines are the signature of alveolar-interstitial syndrome. In cardiogenic pulmonary edema:
- Bilateral, diffuse B-lines (≥3 B-lines per zone in ≥2 bilateral zones) = interstitial syndrome
- B-lines correlate with extravascular lung water (EVLW) and PCWP
- Lichtenstein et al. (Chest 2009) showed A-lines predict low PAOP (<18 mmHg) and B-lines predict elevated PAOP — making LUS a non-invasive surrogate for pulmonary artery catheter data
- Serial monitoring of B-line count tracks response to diuresis in real time
4. Pneumonia / Alveolar Consolidation
LUS sensitivity and specificity for alveolar consolidation exceed 90% (Lichtenstein et al., Intensive Care Med 2004; cited in Bedside General and Cardiac Ultrasonography in the Evaluation of Critically Ill Patients, p. 13).
Key findings:
- Hepatization: lung appears liver-like (loss of aeration)
- Air bronchograms: hyperechoic punctate or linear branching structures within consolidation
- Dynamic air bronchograms (moving with respiration) = patent airway — distinguishes pneumonia from obstructive atelectasis
- Static air bronchograms = reabsorptive atelectasis
- Shred sign: irregular, shredded deep border
- Subpleural consolidations as small as 1 cm can be visualized
5. Acute Respiratory Distress Syndrome (ARDS)
ARDS produces a heterogeneous LUS pattern:
- Bilateral B-lines (non-homogeneous distribution, unlike cardiogenic edema)
- Spared areas with normal A-lines
- Anterior consolidations with air bronchograms
- Irregular, thickened, fragmented pleural line (vs. smooth in pulmonary edema)
- Small pleural effusions
This heterogeneity on LUS helps differentiate ARDS from cardiogenic pulmonary edema, which shows homogeneous bilateral B-lines with a smooth pleural line.
6. Acute Cor Pulmonale / Pulmonary Embolism
LUS findings in PE are indirect:
- Subpleural consolidations (wedge-shaped, hypoechoic) due to pulmonary infarction — present in ~30–40% of cases
- Pleural effusion ipsilateral to infarction
- Combined with echocardiography (RV dilation, McConnell sign, D-sign) and DVT scan — this integrated ultrasound approach has high sensitivity for PE without radiation
7. Mechanical Ventilation Monitoring
LUS plays a growing role in ventilator management:
- PEEP-induced lung recruitment: B-line reduction and reappearance of A-lines indicates successful alveolar recruitment (Bouhemad et al., Am J Respir Crit Care Med 2011)
- Antibiotic-induced reaeration: LUS can monitor resolution of VAP consolidation (Bouhemad et al., Crit Care Med 2010)
- Weaning assessment: diaphragm and lung LUS together can predict extubation success
The BLUE Protocol
The Bedside Lung Ultrasound in Emergency (BLUE) protocol (Lichtenstein & Mezière, Chest 2008) is a structured diagnostic algorithm for acute respiratory failure in the ICU. It achieves a diagnostic accuracy >90% for the most common etiologies (pulmonary edema, pneumonia, COPD/asthma exacerbation, PE, pneumothorax) (Bedside General and Cardiac Ultrasonography, p. 13).
BLUE Protocol Algorithm (simplified):
Acute Respiratory Failure
|
Lung sliding?
/ \
NO YES
| |
A-lines? B-lines bilateral?
| / \
Pneumothorax YES NO
Pulmonary A-lines?
Edema |
YES NO
| |
Posterior Consolidation
consolidation? or effusion?
/ \
YES NO
Pneumonia COPD/Asthma/PE
Pediatric Lung Ultrasound
The same principles apply in children. The image below illustrates the key LUS patterns across pediatric respiratory conditions:
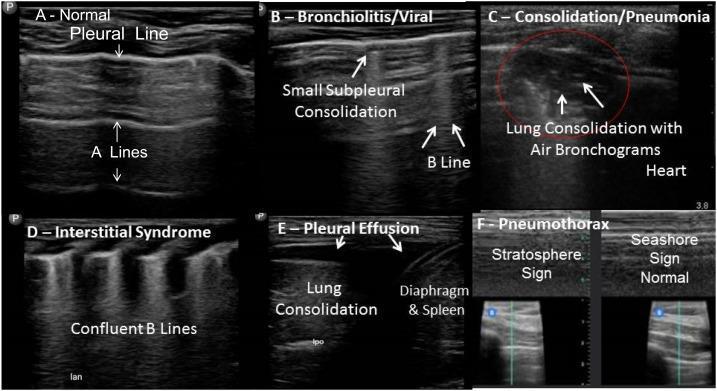
Panel A: Normal (A-lines) | Panel B: Bronchiolitis (B-lines, subpleural consolidation) | Panel C: Pneumonia (hepatization + air bronchograms) | Panel D: Interstitial syndrome (confluent B-lines) | Panel E: Pleural effusion (anechoic collection) | Panel F: M-mode — seashore sign (normal) vs. stratosphere sign (pneumothorax)
Advantages Over Conventional Imaging
| Feature | Chest X-ray | CT Scan | Lung Ultrasound |
|---|---|---|---|
| Bedside availability | Limited (portable) | No | Yes |
| Radiation | Yes | Yes (high) | No |
| Real-time dynamic | No | No | Yes |
| Sensitivity for PTX (supine) | ~50% | ~100% | ~90% |
| Sensitivity for effusion | ~70% | ~100% | >90% |
| Interstitial syndrome | Poor | Excellent | Excellent |
| Guidance for procedures | No | No | Yes |
| Repeatability | Limited | Very limited | Unlimited |
| Cost/accessibility | Low | High | Low |
Limitations
- Operator-dependent: accuracy is closely tied to sonographer competence and experience (Bedside General and Cardiac Ultrasonography, p. 13)
- Subcutaneous emphysema: air under skin obliterates the acoustic window
- Obesity and chest wall dressings: degrade image quality
- Central/deep lesions: not accessible (requires pleural contact)
- Bilateral pneumothorax: can be missed without systematic scanning
- Cannot replace CT for complex structural assessment or mediastinal evaluation
Summary
Lung ultrasound is a first-line diagnostic tool in critical care for pneumothorax, pleural effusion, pulmonary edema, pneumonia/consolidation, ARDS, and pulmonary embolism. Used as part of structured protocols like BLUE, it enables rapid, accurate, radiation-free diagnosis at the bedside with >90% accuracy for acute respiratory failure etiologies. Its integration with cardiac and vascular ultrasound (whole-body POCUS) further enhances diagnostic yield in the critically ill.
This is a shared conversation. Sign in to Orris to start your own chat.