

IMG-597a35050f98f6c84378746d7c6366e8-V.jpg
IMG-278ed12d576ab540d99ae6bc6fdca232-V.jpg
12 yrs male child presented with chest pain radiating to left arm.
Reading File
Searching the Web
chest pain left arm radiation child 12 years ECG ST changes pediatric differential diagnosis
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Now I have enough information to provide a thorough analysis. Let me compile everything from the ECG images and the textbook sources.
ECG Analysis - 12-Year-Old Male with Chest Pain Radiating to Left Arm
ECG Technical Details
- Settings: AUTO 10 mm/mV, 25 mm/s, 150 Hz filter
- Two ECGs provided (the second is dated 2026-05-26, 08:16)
- Leads: Full 12-lead
ECG Findings (Both Tracings)
| Parameter | Finding |
|---|---|
| Rate | ~100-110 bpm - sinus tachycardia |
| Rhythm | Sinus (P waves visible, regular) |
| Axis | Normal/leftward |
| P waves | Normal morphology |
| PR interval | Normal for age (~0.14-0.16s) |
| QRS duration | Normal (~0.08s) |
| ST segments | ST elevation in V4-V5-V6 with tall, slightly peaked T waves |
| ST in I, aVL | Appears elevated/upsloping |
| ST in V1-V2 | Reciprocal depression possible in V1-V2 |
| Q waves | Possible narrow Q waves in lateral leads (I, aVL, V5-V6) - need close inspection |
| QTc | Appears normal |
| Voltage | Prominent R waves in V4-V5 (high voltage) |
The machine printout (second ECG) states: "Sinus mode Tac... Cardiac electr... **Report need..." (truncated), suggesting the machine itself flagged an abnormality requiring interpretation.
Key Differential Diagnosis for This Presentation
This is a HIGH-ALERT case. A 12-year-old male with chest pain radiating to the left arm + ST changes on ECG is NOT a typical musculoskeletal presentation. The primary differentials are:
1. ALCAPA (Anomalous Left Coronary Artery from the Pulmonary Artery) - TOP CONCERN
- ECG shows ischemic changes (ST elevation, Q waves in lateral leads) in a child
- Per Rosen's Emergency Medicine: "A rare but potentially fatal congenital cardiac abnormality detected by ECG, anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA), will show ischemic changes. Older children and adolescents may have acute-on-chronic ischemic symptoms."
- The LCA drains retrograde into the pulmonary artery, causing chronic LV ischemia
- Presentation: chest pain, dyspnea on exertion, syncope
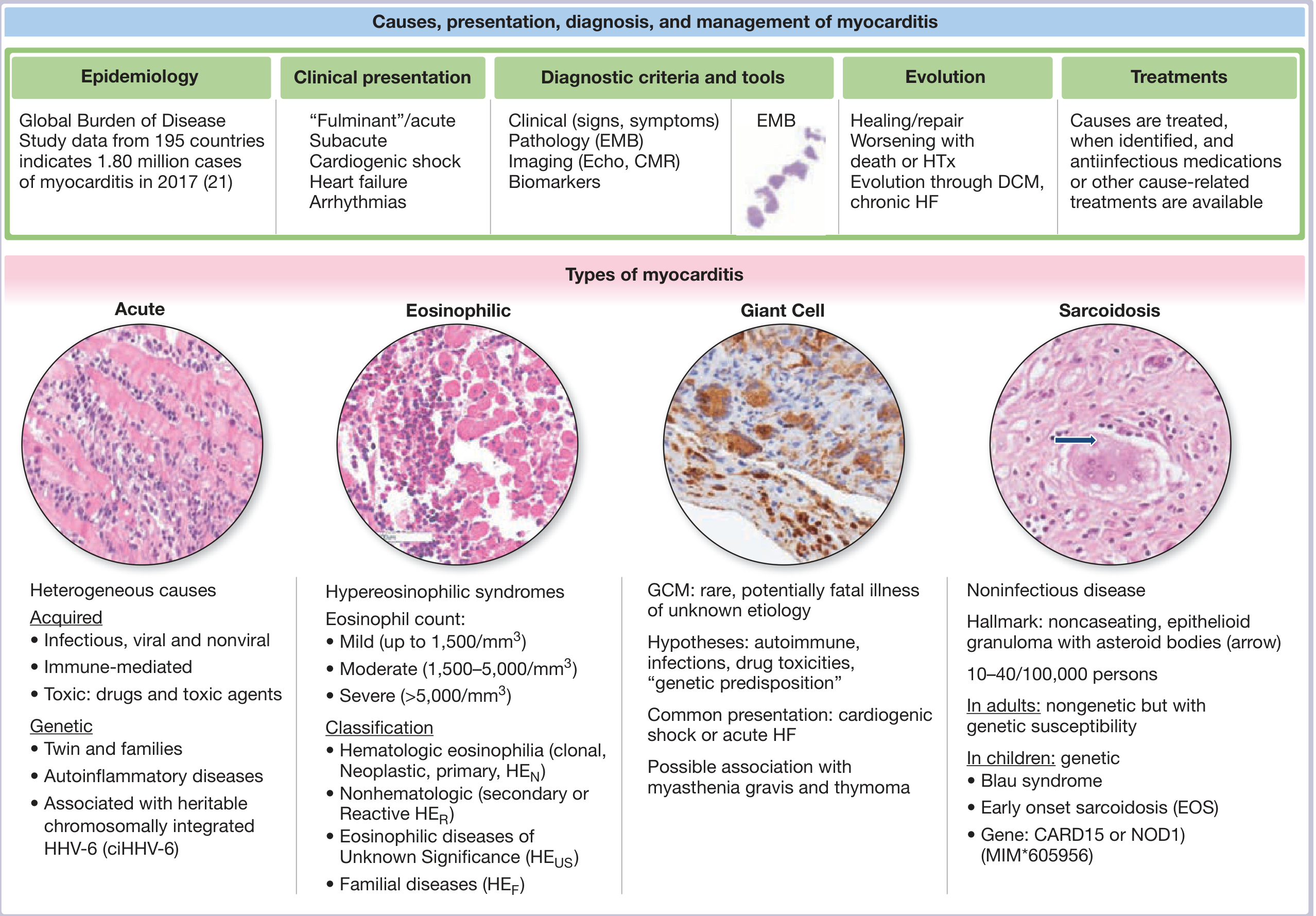
2. Myocarditis
- ST elevation (often diffuse but can be regional) in a child
- Frequently follows a viral illness (check for recent fever, URI, GI illness)
- Elevated troponin would support this
- ST changes in multiple leads without clear "culprit vessel" territory
3. Hypertrophic Cardiomyopathy (HCM)
- Chest pain + left arm radiation on exertion in a child
- LV hypertrophy changes on ECG
- ST changes from subendocardial ischemia
- Check for family history of sudden death
4. Acute Pericarditis
- Diffuse ST elevation with saddle-shaped morphology
- PR depression (look carefully in II and V5)
- Usually positional pain, but can radiate
5. Coronary Artery Anomaly (Other - e.g., anomalous origin from wrong sinus)
- Sudden exertional chest pain in young athletes
- Exercise-triggered ischemia
6. Kawasaki Disease Sequelae
- Coronary aneurysm with thrombosis or stenosis
- Prior history of prolonged fever/rash in early childhood
7. Drug-related / Toxicology
- Cocaine, stimulants, synthetic cannabinoids can cause coronary spasm and MI even in adolescents
Immediate Management Protocol
This child needs urgent evaluation - do not dismiss as musculoskeletal.
Emergency investigations (do NOW in parallel):
- Troponin I/T + serial troponin at 3-6 hours - myocardial injury marker
- CK-MB - additional myocardial damage marker
- BNP/NT-proBNP - ventricular stress marker
- CBC, CRP, ESR - inflammation (myocarditis, pericarditis)
- 2D Echocardiogram with Doppler - MOST IMPORTANT NEXT STEP - assess:
- LV systolic function (global and regional wall motion abnormalities)
- Coronary artery origins (ALCAPA)
- Pericardial effusion
- Septal thickness (HCM)
- Mitral regurgitation (ALCAPA marker)
- Chest X-ray - cardiomegaly, pulmonary edema
- Electrolytes, renal function, magnesium
- Drug screen if relevant history
Monitoring:
- Continuous cardiac monitoring (telemetry)
- IV access
- O2 saturation monitoring
- Keep NPO until echo result available
Specialist referral:
- Urgent pediatric cardiology consultation
- If troponin elevated or echo shows wall motion abnormality: consider transfer to tertiary pediatric cardiac center
What the ECG Specifically Suggests
The ST elevation pattern in V4-V5-V6 with high voltage and the lateral lead changes in this 12-year-old most closely fits:
- Anterolateral ischemia - territory of the LAD/LCx
- In pediatric context: ALCAPA causes exactly this - chronic anterolateral LV ischemia
- Myocarditis is also very possible given the diffuse nature
The machine's note "Report needed" confirms this ECG is flagged as abnormal.
Red Flags Demanding Immediate Action
- Age 12 + chest pain radiating to left arm = never dismiss without cardiac workup
- ST changes on ECG in a child = cardiac emergency until proven otherwise
- Sinus tachycardia at rest may indicate pain, anxiety, or compensated low cardiac output
Bottom line: Admit this child, get urgent echo and troponin, involve pediatric cardiology immediately. ALCAPA and myocarditis are the leading diagnoses and both require urgent intervention. Do not discharge without a definitive explanation for the ECG changes.
- Rosen's Emergency Medicine, 9th ed. (Pediatric ECG and ALCAPA section)
- Braunwald's Heart Disease (ALCAPA - Anomalous Coronary Artery from Pulmonary Artery, p. 3467-3477)
How to rule out myocarditis
Finding Sources
Finding Sources
Searching PubMed
myocarditis diagnosis children cardiac MRI troponin
Reading File
Finding Sources
Searching PubMed
myocarditis diagnosis cardiac MRI children
Reading File
Reading Article
PMID: 38661130
Reading Article
PMID: 40837541
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is the complete, structured approach to ruling out myocarditis in this 12-year-old:
Ruling Out Myocarditis - Systematic Approach
Step 1 - Clinical History (Features that SUPPORT myocarditis)
Ask specifically for:
- Preceding viral illness - fever >38°C in the last 30 days, malaise, chills
- Respiratory symptoms - recent cough, sore throat, URI in past 2-4 weeks
- GI symptoms - vomiting, diarrhea (enteric viral prodrome)
- Autoimmune history - SLE, JIA, inflammatory bowel disease
- Drug/toxin exposure - medications, supplements, substance use
- Prior episode of similar chest pain
If none of these are present, myocarditis is less likely - but cannot be excluded on history alone.
Step 2 - ECG Clues to Distinguish Myocarditis vs. Ischemia
| Feature | Favors Myocarditis | Favors Ischemia (ALCAPA/ACS) |
|---|---|---|
| ST elevation shape | Concave (saddle-shaped) | Convex (tombstone/domed) |
| Distribution | Non-coronary territory (diffuse) | Follows coronary artery territory |
| Reciprocal ST depression | Absent | Present |
| PR depression | Present (especially in lead II) | Absent |
| Q waves | Late finding only | Pathological Q waves earlier |
| AV block | Possible (GCM/sarcoid) | Uncommon |
On this child's ECG, the ST elevation is most prominent in V4-V5-V6 - this is a coronary territory (LAD/LCx), which makes ALCAPA or ischemia at least as likely as myocarditis.
Step 3 - Laboratory Investigations
Order all of the following:
| Test | Significance in Myocarditis |
|---|---|
| hs-Troponin I/T (serial x3) | Elevated but often persistently elevated (not the ACS-pattern rise-fall). Normal troponin does NOT exclude myocarditis |
| CK-MB | Elevated with myocyte injury |
| BNP / NT-proBNP | Elevated if LV dysfunction present; may be normal |
| ESR + CRP | Elevated in myocarditis; only mildly elevated in ACS - helps differentiate |
| Full blood count with differential | Eosinophilia suggests eosinophilic/hypersensitivity myocarditis |
| LFTs, metabolic panel | Baseline; hepatomegaly from RV failure |
| Lactate | Raised if low cardiac output/fulminant course |
| Blood cultures | If febrile - rule out bacterial myocarditis |
| Viral serology | Coxsackievirus B, adenovirus, Parvovirus B19, HHV-6, EBV, CMV, COVID-19 - Parvovirus B19 and HHV-6 are the most common in pediatric myocarditis (Hutchinson & Law, 2025, PMID 40837541) |
| ANA, anti-dsDNA | Screen for autoimmune etiology |
| Anticardiac autoantibodies | If available |
| Throat/NP swab PCR | Enterovirus, respiratory viruses |
Key point: Troponin persistently elevated over weeks = myocarditis. ACS-pattern rapid rise and fall = more likely ischemic event.
Step 4 - Echocardiography (MOST ACCESSIBLE - Do First)
2D echo with Doppler looking for:
| Finding | Interpretation |
|---|---|
| Global LV dysfunction (reduced EF) | Myocarditis (diffuse inflammation) |
| Regional wall motion abnormality (RWMA) | Can occur in both; check if it follows coronary territory |
| Non-coronary territory RWMA | Favors myocarditis |
| Coronary territory RWMA | Favors ALCAPA or ischemia |
| Pericardial effusion | Myopericarditis |
| LV/RV dilation | Dilated myocarditis |
| Septal thickening | HCM (alternative diagnosis) |
| Coronary origins visible | Rules out ALCAPA if both coronaries seen arising from aorta |
| Mitral regurgitation | Can occur in myocarditis (annular dilation) or ALCAPA (papillary muscle ischemia) |
Step 5 - Cardiac MRI (CMR) - GOLD STANDARD NON-INVASIVE TEST
This is the single most important test to confirm or exclude myocarditis.
CMR sequences for myocarditis (Lake Louise Criteria, updated 2018):
| Sequence | What it shows | Myocarditis finding |
|---|---|---|
| T2-weighted / T2 mapping | Myocardial edema (acute inflammation) | Increased T2 signal / elevated T2 values |
| T1 mapping / ECV | Diffuse fibrosis and edema | Elevated native T1 and ECV |
| Early gadolinium enhancement (EGE) | Myocardial hyperemia/capillary leak | Increased global signal ratio |
| Late gadolinium enhancement (LGE) | Myocyte necrosis/fibrosis | Mid-wall or epicardial pattern (NOT subendocardial) |
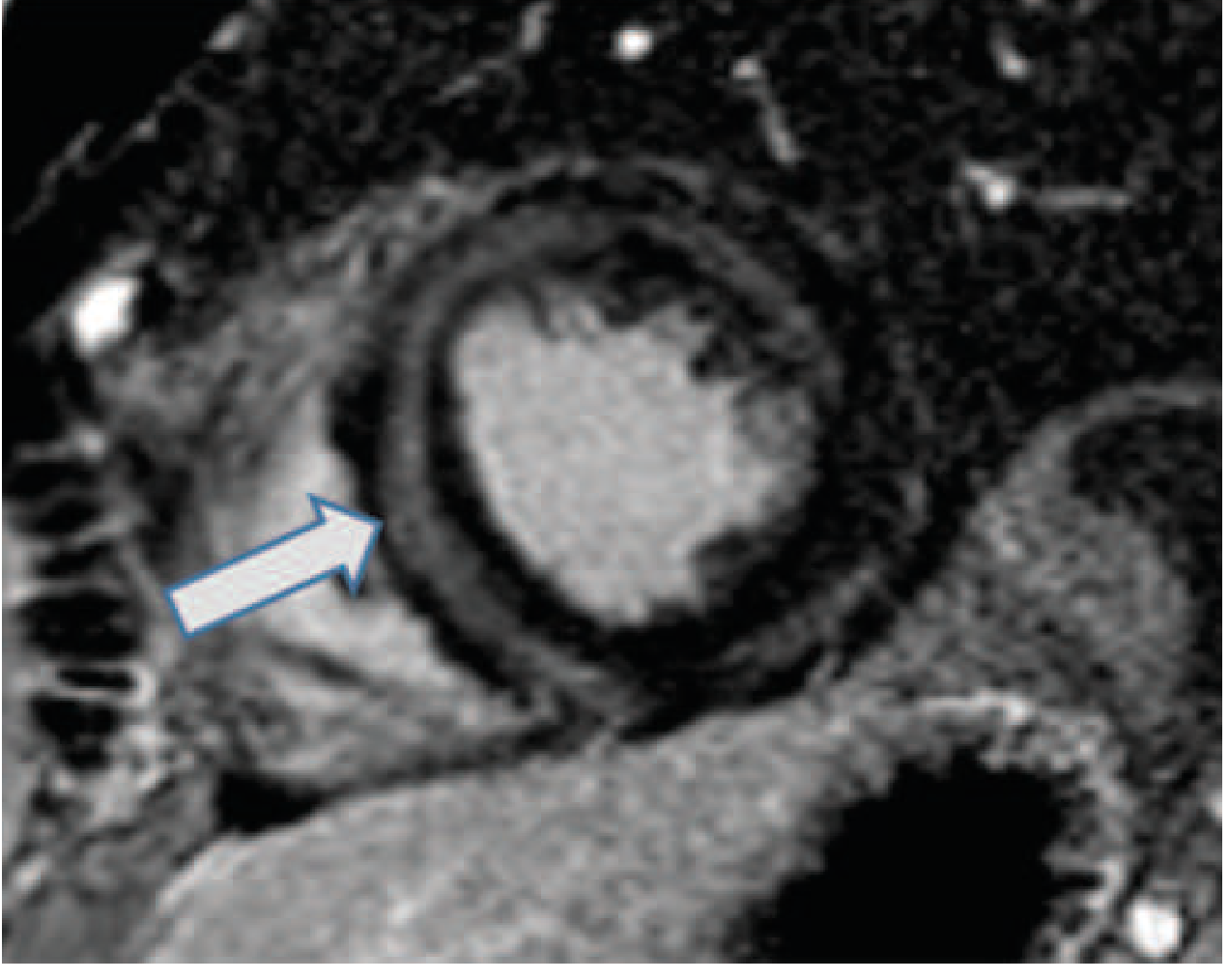
The LGE distribution is the critical differentiator:
- Myocarditis: Mid-wall or epicardial LGE, non-coronary territory
- Ischemia/ALCAPA: Subendocardial or transmural LGE in a coronary artery distribution
- HCM: LGE at RV insertion points or within hypertrophied segments
Per Harrison's (22nd ed.): "Cardiac magnetic resonance image of myocarditis showing the typical mid-wall location for late gadolinium enhancement from cardiac inflammation and scarring."
Limitation in pediatrics: CMR may require sedation in young children, and availability can be limited - but at age 12, this is generally feasible. (Goldberg et al., 2024, PMID 38661130)
Step 6 - Coronary Angiography / CT Coronary Angiography
Per Fuster's Heart (15th ed.): "In patients with an acute coronary syndrome-like presentation, coronary angiography is still necessary to exclude obstructive coronary artery disease."
For this 12-year-old specifically:
- CT coronary angiography can confirm or exclude ALCAPA/coronary anomalies non-invasively
- Normal coronary anatomy on imaging shifts the diagnosis strongly toward myocarditis
- If echo shows coronary origins clearly from the aorta = ALCAPA excluded
Step 7 - Endomyocardial Biopsy (EMB) - The True Gold Standard
Histological gold standard but now uncommon in pediatric practice for routine myocarditis.
Dallas Criteria (classic): Inflammatory infiltrate + myocyte necrosis/degeneration on biopsy.
Modern approach: Dallas criteria + immunohistochemistry (anti-CD3, anti-CD68) + viral PCR from biopsy tissue.
When to do EMB in this child:
- Diagnosis remains unclear after echo + CMR
- Suspected fulminant myocarditis needing specific treatment
- Suspected giant cell myocarditis (GCM), cardiac sarcoidosis, or necrotizing eosinophilic myocarditis - these have specific treatments and require tissue diagnosis
- Hemodynamic compromise requiring circulatory support
Summary: Step-by-Step Ruling Out Algorithm for This Child
1. History → viral prodrome? autoimmune? drugs?
↓
2. ECG → ST shape? PR depression? Non-coronary distribution?
↓
3. Labs → Troponin (serial), CRP/ESR, CBC differential, viral serology
↓
4. Echo → LV function, wall motion, coronary origins, pericardial effusion
↓
5. CMR → T2/T1 mapping + LGE pattern (mid-wall = myocarditis; subendocardial = ischemia)
↓
6. If coronary disease not excluded → CTA coronaries or angiography (rule out ALCAPA)
↓
7. If diagnosis still uncertain + fulminant/specific type suspected → EMB
Myocarditis is effectively ruled OUT when:
- CMR shows no myocardial edema (T2), no elevated T1/ECV, and no LGE
- Echo shows normal LV function, no pericardial effusion, no RWMA
- Troponin normal or rapidly normalizing
- Inflammatory markers (CRP, ESR) are normal
- Viral serology negative
Myocarditis cannot be excluded on clinical/biochemical grounds alone - normal troponin and normal CRP do not rule it out. CMR is required for definitive exclusion.
- Fuster and Hurst's The Heart, 15th ed. (Table 20-4, Diagnostic Approach to Myocarditis)
- Harrison's Principles of Internal Medicine, 22nd ed. (Myocarditis, CMR LGE pattern)
- Hutchinson Z & Law Y. Myocarditis in children: diagnosis and management. JHLT Open. 2025 [PMID 40837541]
- Goldberg JF et al. Myocarditis in children 2024. Curr Opin Cardiol. 2024 [PMID 38661130]
Treatment
Finding Sources
Finding Sources
Searching PubMed
myocarditis treatment children IVIG immunosuppression
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.