Cau explain the the avf care cannulatio and their sign of infection and evaluation
Arteriovenous Fistula (AVF): Care, Cannulation, Signs of Infection & Evaluation
What is an AVF?
1. AVF Care (Pre- and Post-Cannulation)
Pre-Maturation (After Surgical Creation)
- Avoid blood pressure measurements, IV lines, and blood draws in the AVF arm — preserving the vein is paramount
- Avoid PICC lines in the fistula arm; these cause venous stenosis and can eliminate the site for future access
- Exercise the fistula arm (e.g., squeezing a rubber ball) to promote maturation
- Assess maturation using the "Rule of 6s": vein diameter ≥ 6 mm, flow ≥ 600 mL/min, depth ≤ 6 mm from skin surface, and mature segment ≥ 6 cm — typically achieved by 6 weeks post-surgery
Daily Patient Care
- Inspect the fistula site daily for erythema, swelling, warmth, discharge
- Keep skin clean and dry; avoid trauma, tight clothing, or jewelry over the site
- Never sleep on the fistula arm
- Report any loss of thrill or bruit to the care team immediately
2. Cannulation Techniques
A. Rope Ladder Technique (Standard)
- Needle insertion sites are rotated systematically along the entire length of the fistula
- Distributes trauma evenly, reducing aneurysm formation at individual sites
- Requires a well-developed segment of at least 6–10 cm
B. Buttonhole (Constant-Site) Technique
- The same needle track is used at every session, creating a fibrous tunnel
- A blunt needle follows the established track after the first few sessions with sharp needles
- Advantages: less pain, less aneurysm formation at individual sites
- Disadvantage: higher infection risk (Staphylococcus aureus bacteremia risk increases with buttonhole method); scab removal must be meticulous and sterile
C. Area Cannulation (Avoided)
- Repeated cannulation in the same small area
- Leads to aneurysm formation and stenosis — this technique is discouraged
Needle Insertion Tips
- Typically two needles (arterial + venous, 14–17 gauge) are inserted in the direction of blood flow
- The arterial needle is placed toward the arteriovenous anastomosis; the venous needle is placed further upstream to return blood
- Minimum separation of ~5 cm between needles to reduce recirculation
- Apply firm pressure for 10–15 minutes post-needle removal to achieve hemostasis
3. Signs of AVF Infection
Local Signs
| Sign | Description |
|---|---|
| Erythema | Redness around the cannulation site or anastomosis |
| Warmth | Local increase in temperature beyond the expected warmth of the fistula |
| Swelling/Induration | Edema or firmness at the site |
| Tenderness | Pain on palpation of the site |
| Purulent discharge | Pus or cloudy exudate from needle sites |
| Bleeding | Prolonged or unusual bleeding from cannulation sites |
Systemic Signs (indicate bacteremia)
- Fever (may be the only manifestation)
- Tachycardia
- Hypotension
- Rigors/chills — especially during dialysis
⚠️ Bacteremia from vascular access infection in HD patients is 10–20× more frequent than in patients with AV fistulas vs. central venous catheters. AVF infection is less common than graft or catheter infection, but when present carries risk of metastatic complications: endocarditis, osteomyelitis, septic arthritis.
Common Organisms
- Staphylococcus aureus (most common; especially with buttonhole technique)
- Staphylococcus epidermidis
- Gram-negative organisms (less common)
4. Evaluation of the AVF
Bedside Physical Examination (Most Important Step)
- Thrill (palpable vibration): should be soft, continuous; a pulsatile or absent thrill suggests stenosis
- Bruit (audible turbulent flow): should be low-pitched and continuous; a high-pitched bruit suggests outflow stenosis
- Branham sign: bradycardia in response to manual compression of the AVF — indicates a high-output fistula
- Raise the fistula arm above the head — a normal fistula should collapse (flatten); failure to collapse indicates venous outflow or central venous stenosis
- A bounding pulsation with increasing aneurysm size also suggests outflow obstruction
- Aneurysms or pseudoaneurysms
- Hematoma, skin thinning over aneurysm (risk of rupture)
- Signs of ischemia in the hand ("steal syndrome"): pallor, coolness, pain
Surveillance Monitoring
| Method | Purpose |
|---|---|
| Static/Dynamic venous pressure | Serial trending for stenosis — change over time matters more than absolute value |
| Ultrasound dilution (Transonic device) | Measures fistula blood flow; most reliable objective method |
| Doppler ultrasound | Evaluates stenosis, thrombosis, aneurysm; assesses flow velocity |
| Fistulogram (angiography) | Definitive evaluation before any intervention; reveals exact site and degree of stenosis |
Laboratory Indicators of Access Dysfunction
- Declining HD adequacy (Kt/V or URR) without other explanation → suspect poor access flow
- Difficulty with cannulation by nursing staff
- Prolonged hemostasis time post-needling → suggests arterial inflow or venous outflow stenosis
When to Suspect Impending Failure
- Reduced blood flow rates on the dialysis machine
- Frequent access alarms
- Inadequate dialysis dose (Kt/V < 1.2)
- Arm/limb edema on the fistula side (central vein stenosis)
Summary Table
| Domain | Key Points |
|---|---|
| Care | Rotate sites (rope ladder), no BP/IV on fistula arm, daily inspection, preserve patency |
| Cannulation | Rope ladder (preferred), buttonhole (pain reduction but ↑ infection risk), avoid area technique |
| Infection signs | Erythema, warmth, swelling, tenderness, purulent discharge; systemic: fever, rigors, hypotension |
| Evaluation | Physical exam (thrill, bruit, Branham sign), Doppler US, flow monitoring, fistulogram if needed |
Can u give me in poster form
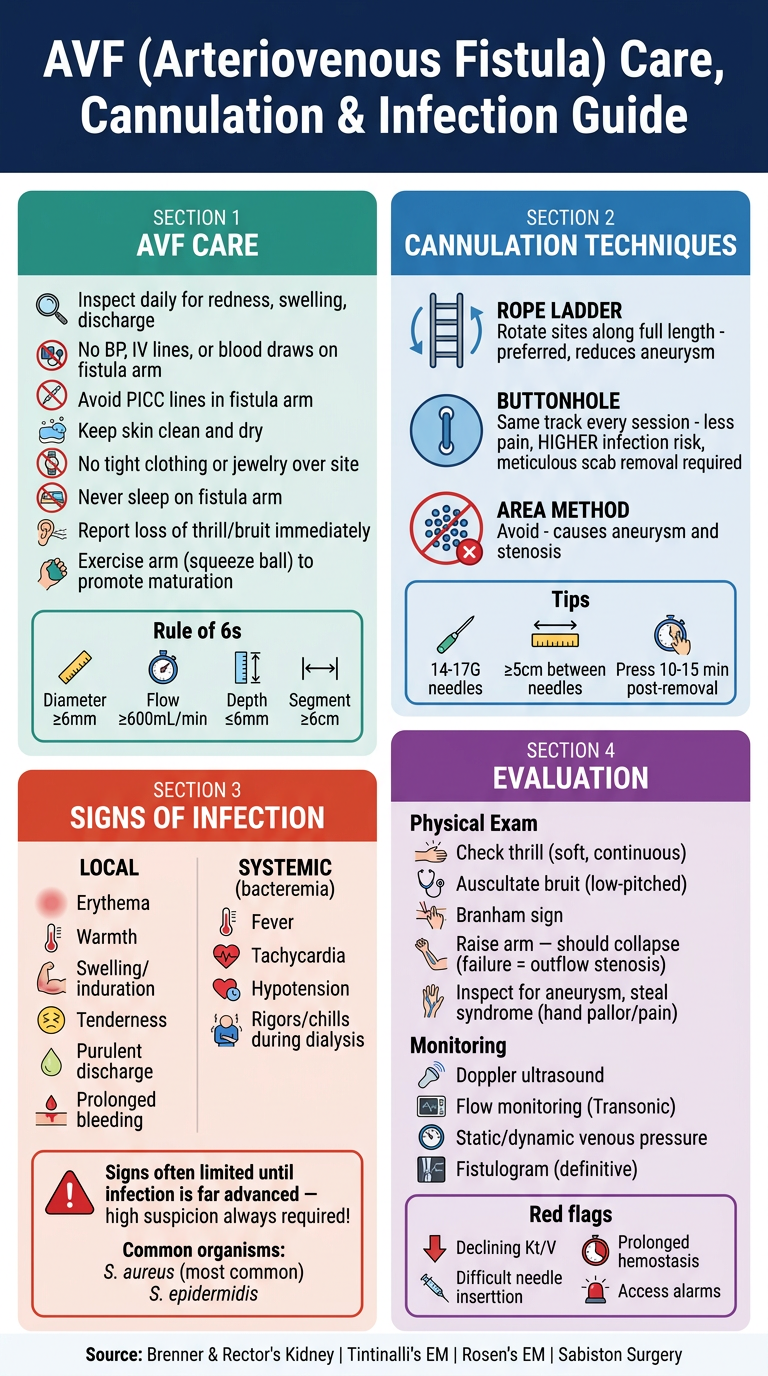
A professional medical educational poster titled "AVF (Arteriovenous Fistula) Care, Cannulation & Infection Guide" for hemodialysis nurses and clinicians. The poster has a clean clinical design with a dark navy blue header and white/light sections below. It is divided into 4 color-coded sections: 1. SECTION 1 - "AVF CARE" (teal/green background): - Bullet points: Inspect daily for redness, swelling, discharge | No BP, IV lines, or blood draws on fistula arm | Avoid PICC lines in fistula arm | Keep skin clean and dry | No tight clothing or jewelry over site | Never sleep on fistula arm | Report loss of thrill/bruit immediately | Exercise arm (squeeze ball) to promote maturation | Rule of 6s: diameter ≥6mm, flow ≥600mL/min, depth ≤6mm, segment ≥6cm 2. SECTION 2 - "CANNULATION TECHNIQUES" (blue background): - Three techniques with icons: ROPE LADDER (rotate sites along full length - preferred, reduces aneurysm) | BUTTONHOLE (same track every session - less pain, HIGHER infection risk, meticulous scab removal required) | AREA METHOD (avoid - causes aneurysm and stenosis) - Tips: 14-17G needles | ≥5cm between needles | Press 10-15 min post-removal 3. SECTION 3 - "SIGNS OF INFECTION" (red/orange background): - LOCAL: Erythema | Warmth | Swelling/induration | Tenderness | Purulent discharge | Prolonged bleeding - SYSTEMIC (bacteremia): Fever | Tachycardia | Hypotension | Rigors/chills during dialysis - Warning box: "Signs often limited until infection is far advanced — high suspicion always required!" - Common organisms: S. aureus (most common), S. epidermidis 4. SECTION 4 - "EVALUATION" (purple background): - Physical Exam: Check thrill (soft, continuous) | Auscultate bruit (low-pitched) | Branham sign | Raise arm — should collapse (failure = outflow stenosis) | Inspect for aneurysm, steal syndrome (hand pallor/pain) - Monitoring: Doppler ultrasound | Flow monitoring (Transonic) | Static/dynamic venous pressure | Fistulogram (definitive) - Red flags: Declining Kt/V | Difficult cannulation | Prolonged hemostasis | Access alarms Footer: "Source: Brenner & Rector's Kidney | Tintinalli's EM | Rosen's EM | Sabiston Surgery" The poster is portrait orientation, highly readable, uses icons and bold headings, clinical and professional appearance.
- AVF Care — daily inspection, vein preservation, Rule of 6s
- Cannulation Techniques — rope ladder, buttonhole, and why to avoid area cannulation
- Signs of Infection — local (erythema, warmth, discharge) and systemic (fever, rigors, hypotension), with a high-suspicion warning
- Evaluation — physical exam (thrill, bruit, Branham sign), Doppler, flow monitoring, and red flags