What is neoplasia ..how to differentiate between benign and malignant tumours
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
I now have comprehensive content from Robbins & Kumar Basic Pathology. Let me compile a thorough, well-structured answer.
Neoplasia: Definition and Benign vs. Malignant Tumours
Source: Robbins & Kumar Basic Pathology, 10th ed.
What is Neoplasia?
Neoplasia literally means "new growth" (Greek: neos = new, plasia = formation). Neoplastic cells are described as "transformed" because they replicate incessantly, having escaped the regulatory mechanisms that govern normal cell proliferation. Neoplasms therefore enjoy a degree of autonomy, though they still depend on the host for nutrition and blood supply.
In everyday clinical usage, a neoplasm is called a tumor, and the study of tumors is oncology (from Greek oncos, "tumor").
Cancer is fundamentally a genetic disorder caused by:
- DNA mutations from mutagens or spontaneous replication errors
- Inherited mutations
- Epigenetic alterations (aberrant DNA methylation, histone modification)
These changes accumulate through clonal evolution - cells with growth/survival advantages outcompete their neighbors via Darwinian selection, progressively acquiring more aggressive characteristics (tumor progression).
Components of All Tumors
Every tumor, benign or malignant, has two basic components:
| Component | Description |
|---|---|
| Parenchyma | The transformed (neoplastic) cells - determines biologic behavior and gives the tumor its name |
| Stroma | Host-derived supporting tissue: connective tissue, blood vessels, and inflammatory cells - provides the blood supply essential for growth |
Nomenclature (Naming Tumors)
Benign Tumors
Named by attaching the suffix -oma to the cell of origin:
| Origin | Benign Tumor Name |
|---|---|
| Fibrous tissue | Fibroma |
| Cartilage | Chondroma |
| Glandular epithelium | Adenoma |
| Epithelium (papillary projection) | Papilloma |
| Cystic epithelium | Cystadenoma |
| Fat cells | Lipoma |
| Smooth muscle | Leiomyoma |
| Blood vessels | Hemangioma |
Malignant Tumors
| Origin | Malignant Tumor Name |
|---|---|
| Epithelium (any germ layer) | Carcinoma |
| Glandular epithelium | Adenocarcinoma |
| Squamous epithelium | Squamous cell carcinoma |
| Mesenchymal/solid tissue | Sarcoma |
| Fat cells (malignant) | Liposarcoma |
| Cartilage (malignant) | Chondrosarcoma |
| Blood cell lineages | Leukemia / Lymphoma |
Special cases: Teratomas (from totipotent germ cells, contain tissue from >1 germ layer); Mixed tumors like pleomorphic adenoma of salivary gland (epithelial + myxoid stroma).
Differentiating Benign from Malignant Tumours
This is the central task in tumor pathology. Four key features are assessed:
1. Differentiation and Anaplasia
Differentiation refers to how closely the tumor cells resemble their normal counterpart morphologically and functionally.
| Feature | Benign | Malignant |
|---|---|---|
| Differentiation | Well differentiated - closely resembles normal tissue | Ranges from well to poorly differentiated; anaplastic = undifferentiated |
| Nuclear morphology | Normal size, shape, chromatin | Hyperchromatic nuclei, prominent nucleoli, pleomorphism |
| Mitoses | Rare, normal | Frequent, often atypical (tripolar/quadripolar spindles) |
| Cell uniformity | Uniform cells | Pleomorphism (variation in size and shape) |
| Growth pattern | Organized, retains normal architecture | Disordered - loss of polarity, sheets of cells, absent gland/squamous architecture |
| Functional activity | Retains functions of parent cell | Often loses specialized functions; may express ectopic/fetal proteins |
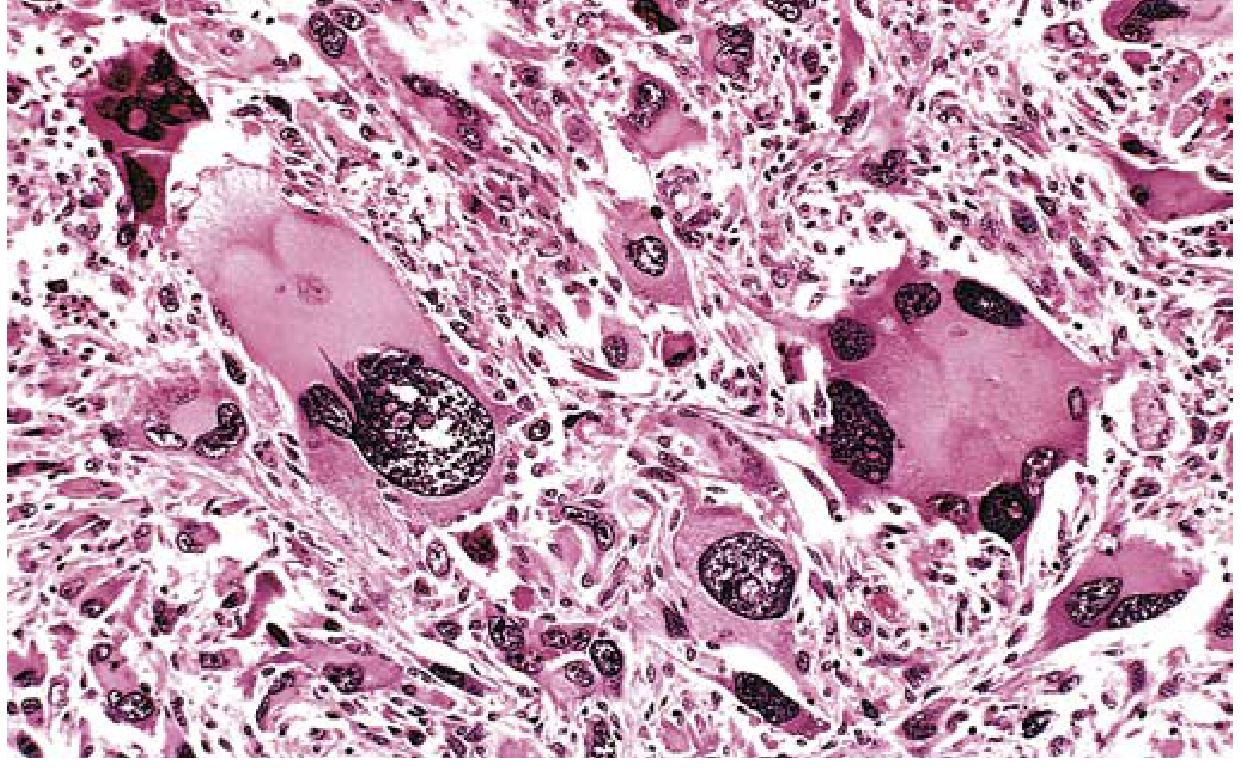
Anaplasia is the hallmark of malignancy - cells that fail to differentiate, showing:
- Marked pleomorphism (variation in cell and nuclear size/shape)
- Hyperchromatism (dark-staining nuclei with coarse chromatin)
- Large, prominent nucleoli
- Abundant, often abnormal mitoses
- Loss of polarity and architecture
Below is a histological image of a pleomorphic malignant tumor (rhabdomyosarcoma) showing the marked nuclear variation and tumor giant cells characteristic of anaplasia:
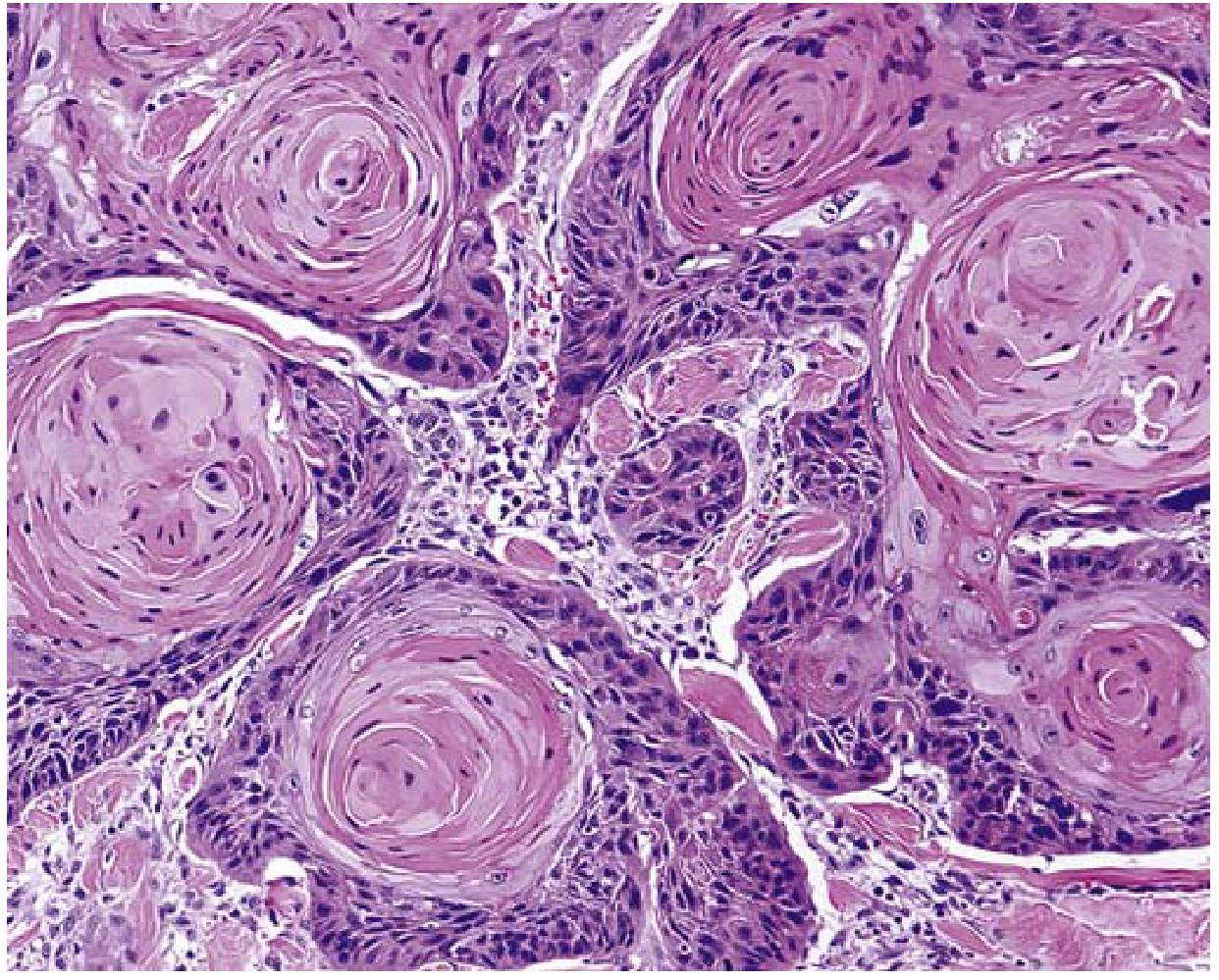
And here is a well-differentiated squamous cell carcinoma of the skin, showing keratin pearl formation - an example of retained differentiation even in malignancy:
2. Rate of Growth
| Feature | Benign | Malignant |
|---|---|---|
| Growth rate | Slow, often remains stable | Generally rapid; the more anaplastic, the faster |
| Mitotic index | Low | High |
| Necrosis | Uncommon | Common (outgrows blood supply) |
3. Local Invasion
This is one of the most reliable distinguishing features:
| Feature | Benign | Malignant |
|---|---|---|
| Capsule | Usually encapsulated with a fibrous capsule | Usually non-encapsulated; lack well-defined borders |
| Borders | Well-defined, sharp margins | Irregular, infiltrative margins |
| Local behavior | Remains localized; pushes adjacent tissue (cohesive, expansile mass) | Infiltrates and destroys adjacent tissue |
| Surgical removal | Usually complete and curative | Often leaves microscopic residual disease |
Note: Some benign tumors (e.g., hemangiomas) are not encapsulated but are still non-invasive.
4. Metastasis
Metastasis is the definitive marker of malignancy. Benign tumors never metastasize.
| Feature | Benign | Malignant |
|---|---|---|
| Distant spread | Never | Yes - hallmark of malignancy |
| Routes of spread | - | Lymphatic, hematogenous, seeding of body cavities |
| Common sites | - | Lymph nodes, liver, lung, bone, brain (varies by tumor type) |
Malignant spread requires tumor cells to:
- Invade the extracellular matrix (ECM)
- Enter lymphatics or blood vessels (intravasation)
- Survive in circulation
- Exit at a distant site (extravasation)
- Form a new colony (colonization)
Summary Comparison Table
| Feature | Benign | Malignant |
|---|---|---|
| Differentiation | Well differentiated | Variable - may be anaplastic |
| Growth rate | Slow | Usually rapid |
| Nuclear features | Normal | Pleomorphism, hyperchromatism, abnormal mitoses |
| Capsule | Usually present | Usually absent |
| Borders | Well-defined | Irregular, infiltrative |
| Local invasion | Absent | Present |
| Metastasis | Absent | May be present |
| Necrosis | Uncommon | Common |
| Recurrence after removal | Uncommon | Relatively common |
| Patient outcome | Generally curable | Variable; may be lethal |
A Note on Dysplasia
Dysplasia ("disordered growth") sits between normal epithelium and frank malignancy. Dysplastic cells show:
- Pleomorphism and nuclear enlargement
- Hyperchromatic nuclei
- Abnormally positioned mitoses (superficial layers instead of basal)
- Loss of architectural organization
When severe dysplasia involves the full epithelial thickness, it is called carcinoma in situ - a preinvasive stage. Mild-to-moderate dysplasia can regress if the inciting cause is removed. Dysplasia itself is not cancer but marks tissue at elevated cancer risk.
Robbins & Kumar Basic Pathology, 10th ed., Chapter 6 (Neoplasia), pp. 187-220
This is a shared conversation. Sign in to Orris to start your own chat.