Anti epileptics from padmaja Uday Kumar
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have sufficient comprehensive content to compile a thorough antiepileptics notes in the style of Padmaja Udaykumar. Let me now compose the full answer.
Antiepileptic Drugs (AEDs)
Based on Lippincott Illustrated Reviews: Pharmacology & Katzung's Basic & Clinical Pharmacology - covering the standard Padmaja Udaykumar syllabus
Classification of Seizures (ILAE)
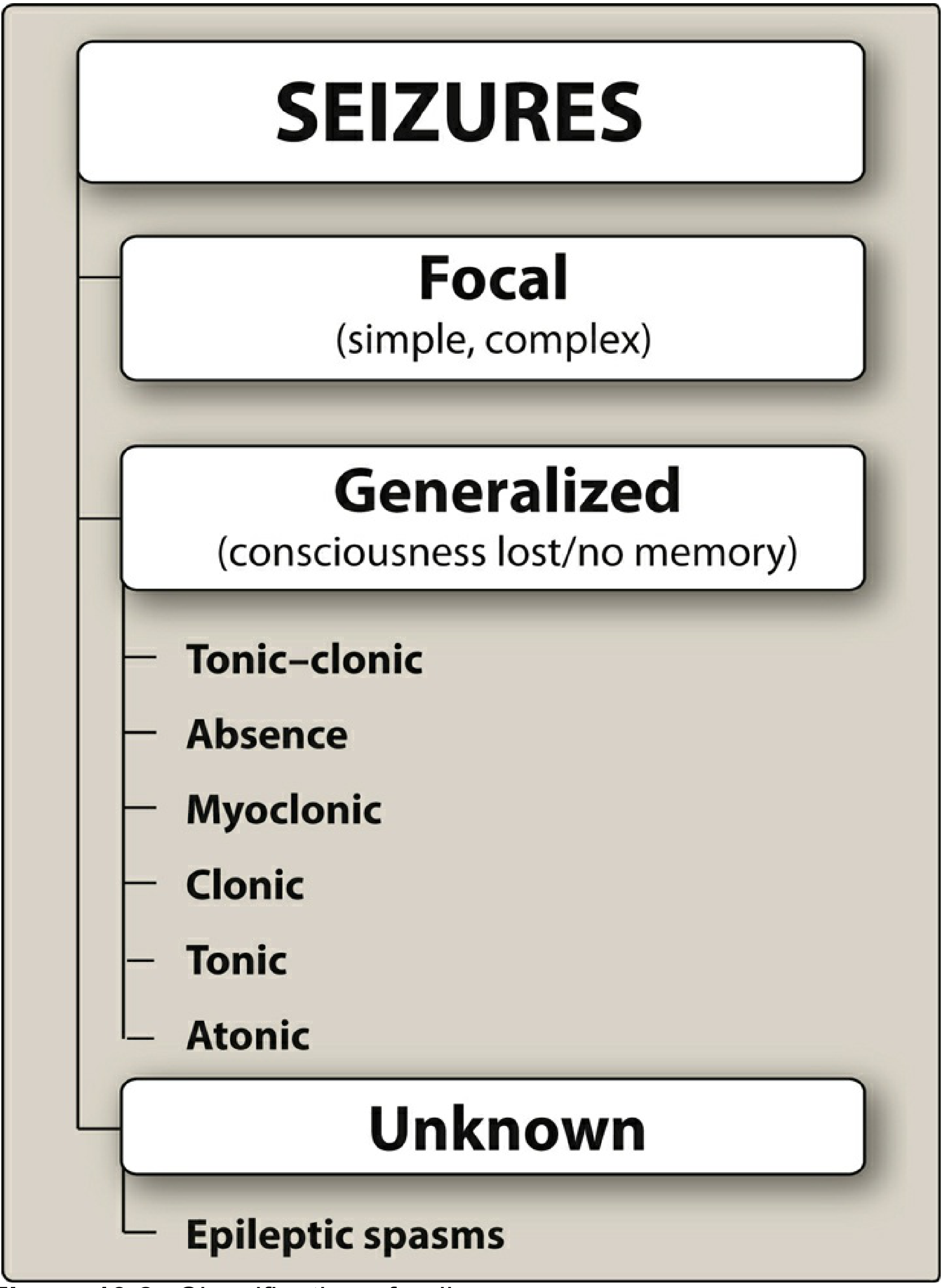
| Type | Subtypes | Key Features |
|---|---|---|
| Focal (Partial) | Aware (simple partial) / Impaired awareness (complex partial) / Focal-to-bilateral tonic-clonic | Originates in one hemisphere; consciousness may/may not be lost |
| Generalized | Tonic-clonic, Absence, Myoclonic, Clonic, Tonic, Atonic | Both hemispheres from onset; consciousness always lost |
| Unknown | Epileptic spasms (West syndrome) | Cannot be classified as focal or generalized |
Seizure Type Details
- Tonic-clonic (Grand mal): Loss of consciousness → sustained muscle contraction (tonic) → rhythmic jerking (clonic). Post-ictal confusion and exhaustion.
- Absence (Petit mal): Brief (3-5 sec) abrupt loss of consciousness with eye blinking. Onset at 3-5 years. Classic 3/sec spike-and-wave on EEG.
- Myoclonic: Brief jerks, usually after waking. Occur in Juvenile Myoclonic Epilepsy (JME), Dravet syndrome.
- Atonic (Drop attacks): Sudden loss of muscle tone - seen in Lennox-Gastaut syndrome.
- Tonic: Extension muscle rigidity, <60 seconds.
Mechanisms of Action of AEDs
AEDs act by three major mechanisms:
- Blocking voltage-gated Na⁺ channels - reduce repetitive high-frequency neuronal firing
- Blocking voltage-gated Ca²⁺ channels (T-type) - specifically for absence seizures
- Enhancing GABAergic inhibition - increase Cl⁻ influx or reduce GABA breakdown
- Blocking glutamate (excitatory) transmission - AMPA or NMDA receptor antagonism
Individual Drugs
1. Phenytoin (Dilantin)
- Mechanism: Blocks voltage-gated Na⁺ channels (use-dependent/frequency-dependent block). Prolongs inactivation state.
- Uses: Focal seizures, tonic-clonic seizures, status epilepticus (IV fosphenytoin), not for absence
- Pharmacokinetics:
- Zero-order (saturation) kinetics at therapeutic doses - small dose increase → large rise in plasma levels
- Highly protein-bound (~90%)
- Enzyme inducer (CYP2C9, CYP2C19, CYP3A4)
- Adverse effects:
- Dose-related: Nystagmus (earliest), ataxia, diplopia, sedation, cognitive impairment
- Chronic: Gingival hyperplasia, hirsutism, coarsening of facial features, peripheral neuropathy, megaloblastic anemia (folate deficiency), osteomalacia
- Idiosyncratic: Stevens-Johnson syndrome (SJS), hypersensitivity, lupus-like syndrome
- IV: Cardiovascular depression, hypotension - use fosphenytoin (water-soluble prodrug) to avoid this
- Teratogenicity: Fetal hydantoin syndrome (cleft palate, cardiac defects, digit abnormalities)
2. Carbamazepine (Tegretol)
- Mechanism: Blocks voltage-gated Na⁺ channels (use-dependent)
- Uses:
- Drug of choice for focal (partial) seizures and tonic-clonic
- Also: Trigeminal neuralgia (drug of choice), bipolar disorder
- NOT used in absence or myoclonic (may worsen)
- Pharmacokinetics:
- Auto-induction of its own metabolism (CYP3A4) - levels fall after 3-4 weeks
- Active metabolite: carbamazepine-10,11-epoxide
- Enzyme inducer - reduces levels of OCP, warfarin, other AEDs
- Adverse effects:
- CNS: diplopia, dizziness, ataxia
- GI: nausea
- SIADH (hyponatremia) - common
- Leukopenia, agranulocytosis (monitor CBC)
- SJS/TEN - especially in HLA-B*1502 positive patients (Southeast Asian genetic screen recommended before use)
- Aplastic anemia (rare)
- Drug of choice: Focal seizures
3. Valproic Acid / Sodium Valproate (Depakote, Epilim)
- Mechanism: Multiple - blocks Na⁺ channels, blocks T-type Ca²⁺ channels, increases GABA (inhibits GABA transaminase)
- Uses:
- Broadest spectrum AED - effective for ALL seizure types (tonic-clonic, absence, myoclonic, focal)
- Drug of choice: Juvenile Myoclonic Epilepsy (JME)
- Also: Migraine prophylaxis, bipolar disorder
- Pharmacokinetics:
- Enzyme inhibitor (opposite of carbamazepine and phenytoin) - raises levels of other AEDs (e.g., lamotrigine levels can double)
- Highly protein-bound
- Metabolized by glucuronidation and mitochondrial beta-oxidation
- Adverse effects:
- GI: nausea, vomiting (give enteric-coated)
- Weight gain
- Hair loss (alopecia) - may regrow curly
- Tremor
- Hepatotoxicity - rare but fatal; highest risk in children <2 years on polytherapy
- Pancreatitis - rare
- Neural tube defects (spina bifida) - 1-2% risk; AVOID in pregnancy (most teratogenic AED)
- Polycystic ovarian syndrome with long-term use
- Hyperammonemic encephalopathy (especially with topiramate co-use)
- Contraindicated: Pregnancy, hepatic disease, urea cycle disorders
4. Phenobarbital
- Mechanism: Enhances GABA_A receptor activity - prolongs Cl⁻ channel opening duration (vs. benzodiazepines which increase frequency)
- Uses:
- Tonic-clonic, focal seizures
- Status epilepticus (IV/IM)
- Neonatal seizures
- Febrile convulsions (prophylaxis - though no longer recommended routinely)
- Pharmacokinetics:
- Long half-life (~80-100 hours) - once daily dosing
- Major enzyme inducer (CYP1A2, CYP2C9, CYP3A4)
- Adverse effects:
- Sedation, cognitive impairment (limits use)
- Dependence and tolerance
- Hyperactivity in children (paradoxical)
- Megaloblastic anemia (folate deficiency)
- Osteomalacia (Vitamin D deficiency via enzyme induction)
- Respiratory depression in overdose
5. Ethosuximide (Zarontin)
- Mechanism: Blocks T-type Ca²⁺ channels in thalamic neurons - interrupts the oscillatory firing underlying absence seizures
- Uses:
- Drug of choice for absence seizures (petit mal) in children
- Effective ONLY for absence - no effect on tonic-clonic
- Adverse effects:
- GI: nausea, vomiting, anorexia (most common - take with food)
- CNS: headache, dizziness, hiccups
- Lupus-like syndrome
- Blood dyscrasias (leukopenia, aplastic anemia - rare)
- Note: If a patient has BOTH absence + tonic-clonic seizures, use valproate (not ethosuximide) - Lippincott, Ch. 19
6. Benzodiazepines (Diazepam, Lorazepam, Clonazepam, Clobazam)
- Mechanism: Enhance GABA_A receptor activity - increase frequency of Cl⁻ channel opening (vs. barbiturates which increase duration)
- Uses:
| Drug | Main Use |
|---|---|
| Diazepam (IV/rectal) | Acute status epilepticus (first-line), febrile seizures (acute) |
| Lorazepam (IV) | Preferred in status epilepticus (longer CNS duration than diazepam) |
| Clonazepam | Myoclonic seizures, absence, Lennox-Gastaut; also panic disorder |
| Clobazam | Adjunctive for Lennox-Gastaut syndrome |
- Adverse effects: Sedation, tolerance, dependence, respiratory depression
- Tolerance develops rapidly to antiepileptic effect of clonazepam - limits long-term use
7. Lamotrigine (Lamictal)
- Mechanism: Blocks voltage-gated Na⁺ channels; also blocks Ca²⁺ channels; reduces glutamate release
- Uses: Broad spectrum - focal seizures, generalized tonic-clonic, absence, Lennox-Gastaut, bipolar disorder
- Pharmacokinetics:
- Metabolized by glucuronidation
- Half-life affected greatly by co-medications: Valproate doubles lamotrigine levels (inhibits glucuronidation) → start very low; Enzyme inducers (carbamazepine, phenytoin) halve levels
- Adverse effects:
- Steven-Johnson Syndrome (SJS) - serious risk especially if dose escalated too fast or used with valproate (titrate slowly!)
- Dizziness, diplopia, headache, ataxia
- Generally well-tolerated; weight-neutral
- Relatively safer in pregnancy compared to valproate
8. Gabapentin (Neurontin) & Pregabalin (Lyrica)
- Mechanism: Bind to α2-δ subunit of voltage-gated Ca²⁺ channels → reduce Ca²⁺ influx → reduce neurotransmitter release (NOT related to GABA despite the name)
- Uses:
- Gabapentin: Adjunctive for focal seizures; neuropathic pain, postherpetic neuralgia, restless legs syndrome
- Pregabalin: Same as gabapentin + generalized anxiety disorder, fibromyalgia
- Pharmacokinetics: Not metabolized, excreted unchanged by kidney - dose adjust in renal failure; no drug interactions (no enzyme effects)
- Adverse effects: Sedation, dizziness, ataxia, weight gain, peripheral edema
9. Topiramate (Topamax)
- Mechanism: Multiple - blocks Na⁺ channels, enhances GABA_A, blocks AMPA/kainate glutamate receptors, inhibits carbonic anhydrase
- Uses: Focal seizures, tonic-clonic, Lennox-Gastaut, migraine prophylaxis (second-line)
- Adverse effects:
- Cognitive impairment/word-finding difficulty ("Dope-a-max") - most troublesome
- Weight loss (unlike most AEDs)
- Kidney stones (carbonic anhydrase inhibition → metabolic acidosis → hypocitraturia)
- Glaucoma (acute angle-closure)
- Teratogenic (oral cleft risk)
10. Levetiracetam (Keppra)
- Mechanism: Binds SV2A (synaptic vesicle protein 2A) → modulates neurotransmitter release
- Uses: Focal seizures, myoclonic seizures (JME), generalized tonic-clonic; increasingly used as first-line due to favorable profile
- Pharmacokinetics: Minimal protein binding, mostly renally excreted, minimal drug interactions
- Adverse effects: Sedation, dizziness; behavioral/psychiatric effects - irritability, aggression, depression (most notable)
11. Oxcarbazepine (Trileptal) & Eslicarbazepine
- Mechanism: Blocks voltage-gated Na⁺ channels (similar to carbamazepine but no auto-induction)
- Uses: Focal seizures (preferred over carbamazepine in many centers due to better tolerability)
- Advantages over carbamazepine: Less enzyme induction, no auto-induction, no active epoxide metabolite
- Adverse effects: Dizziness, diplopia; hyponatremia (SIADH) - more prominent than carbamazepine; rash
12. Lacosamide (Vimpat)
- Mechanism: Enhances slow inactivation of voltage-gated Na⁺ channels (unique mechanism among Na⁺ channel blockers)
- Uses: Focal seizures (adjunctive and monotherapy)
- Adverse effects: Dizziness, diplopia, nausea, PR interval prolongation (cardiac monitoring needed)
13. Vigabatrin (Sabril)
- Mechanism: Irreversible inhibitor of GABA transaminase → increases GABA levels
- Uses: Infantile spasms (West syndrome) - drug of choice; adjunctive for refractory focal seizures
- Major ADR: Permanent visual field defects (concentric peripheral vision loss due to retinal toxicity) - mandatory visual field monitoring
14. Zonisamide (Zonegran)
- Mechanism: Blocks Na⁺ and T-type Ca²⁺ channels; also carbonic anhydrase inhibitor
- Uses: Focal seizures (adjunctive); Dravet syndrome, myoclonic
- Adverse effects: Kidney stones, cognitive effects, weight loss, anhydrosis (no sweating - especially in children)
Drug of Choice Summary
| Seizure Type | Drug of Choice |
|---|---|
| Absence (petit mal) | Ethosuximide (children), Valproate (if also has GTC) |
| Juvenile Myoclonic Epilepsy | Valproate |
| Focal (partial) seizures | Carbamazepine, Lamotrigine, Levetiracetam |
| Generalized tonic-clonic | Valproate, Phenytoin, Carbamazepine |
| Status epilepticus (acute) | Lorazepam or Diazepam IV → Fosphenytoin/Phenobarbital |
| Infantile spasms (West syndrome) | Vigabatrin (+ ACTH/prednisolone) |
| Lennox-Gastaut syndrome | Valproate, Felbamate, Clobazam, Rufinamide |
| Neonatal seizures | Phenobarbital |
| Trigeminal neuralgia | Carbamazepine |
| Febrile convulsions (acute) | Rectal/IV Diazepam |
Teratogenicity of AEDs
| Risk | Drug |
|---|---|
| Highest | Valproate (neural tube defects - spina bifida; cognitive impairment in child) |
| High | Phenytoin (fetal hydantoin syndrome), Carbamazepine (spina bifida) |
| Moderate | Topiramate (oral clefts), Phenobarbital |
| Relatively safer | Lamotrigine, Levetiracetam, Oxcarbazepine |
- All pregnant women on AEDs should receive folic acid 5 mg/day (high dose)
- Vitamin K supplementation for mother before delivery (enzyme inducers deplete Vit K → neonatal hemorrhage)
Drug Interactions (Key)
- Enzyme Inducers (increase metabolism of other drugs): Phenytoin, Carbamazepine, Phenobarbital, Primidone → reduce levels of OCP, warfarin, other AEDs
- Enzyme Inhibitors: Valproate → increases lamotrigine levels (double), inhibits phenobarbital metabolism
- Valproate + Lamotrigine = highest SJS risk; start lamotrigine at 25 mg alternate days and titrate slowly
Status Epilepticus Management (Stepwise)
- Immediate (0-5 min): IV Lorazepam 0.1 mg/kg (or Diazepam 0.1-0.2 mg/kg IV/rectal)
- 5-30 min (if seizure continues): IV Fosphenytoin 20 mg PE/kg OR IV Valproate OR IV Levetiracetam
- Refractory (>30 min): IV Phenobarbital; consider ICU with IV Midazolam/Propofol infusion
Special Notes from Padmaja Udaykumar's Approach
| Drug | Unique Point |
|---|---|
| Phenytoin | Zero-order kinetics; gingival hyperplasia; nystagmus is first sign of toxicity |
| Carbamazepine | Auto-induction; test HLA-B*1502 before starting in SE Asians |
| Valproate | Most teratogenic; enzyme inhibitor (opposite of rest); broadest spectrum |
| Ethosuximide | ONLY for absence; T-type Ca²⁺ channel block |
| Benzodiazepines | Increase Cl⁻ channel opening frequency (barbiturates increase duration) |
| Vigabatrin | Irreversible GABA-T inhibitor; retinal toxicity |
| Lamotrigine | Slow titration mandatory to avoid SJS; safe(r) in pregnancy |
| Levetiracetam | SV2A mechanism; minimal drug interactions; causes behavioral issues |
| Topiramate | Weight loss (unique); "Dopamax"; kidney stones |
Note: Padmaja Udaykumar's Clinical Pharmacology textbook is not available in the current library, but the content above is compiled from Lippincott Illustrated Reviews: Pharmacology (Ch. 19 - Drugs for Epilepsy) and Katzung's Basic & Clinical Pharmacology (16e), which cover identical content and are standard references for the same examinations.
This is a shared conversation. Sign in to Orris to start your own chat.