Approach to hematuria history wise
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Campbell-Walsh Urology, Tintinalli's, NKF Primer, and Rosen's. Here is a thorough, well-structured answer.
Approach to Hematuria: History
Hematuria (blood in the urine) may signal pathology anywhere from the glomerulus to the urethra. A structured history is the cornerstone of evaluation - it often localizes the source and stratifies malignancy risk before any test is ordered.
1. First - Confirm It Is True Hematuria
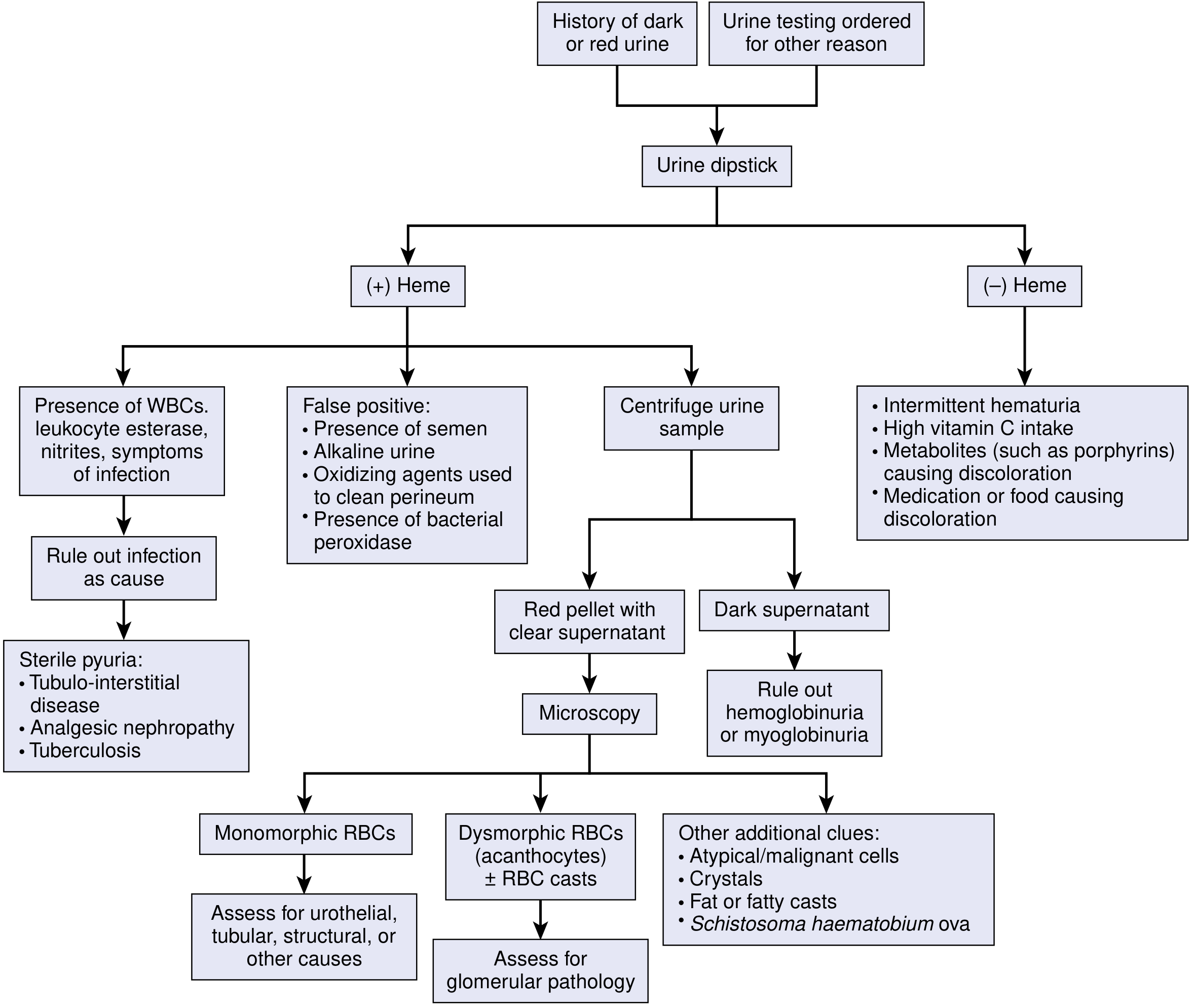
Before taking a detailed history, establish that the patient has true hematuria. Several conditions mimic it (pseudohematuria):
- Foods: beets, rhubarb, blackberries
- Drugs: rifampicin, nitrofurantoin, metronidazole, chloroquine, isoniazid, chlorpromazine
- Other: myoglobinuria (rhabdomyolysis), hemoglobinuria (intravascular hemolysis), porphyrins, high vitamin C intake
A urine dipstick positive for blood must always be followed by microscopy - dipstick alone is insufficient to confirm true hematuria. - Campbell-Walsh Urology
2. Characterize the Hematuria
Gross vs. Microscopic
- Gross hematuria is visible to the patient and is alarming; in patients >50 years, the most common cause is bladder cancer.
- Microscopic hematuria = >5 RBCs/high-power field on two or more samples - found incidentally.
Timing in the Urinary Stream
This is a highly localizing question:
| Timing | Source |
|---|---|
| Initial stream only | Urethra or prostate (anterior urethral bleed expressed at stream onset) |
| Throughout entire stream | Bladder or upper urinary tract (above bladder neck) |
| Terminal (end of stream) | Bladder neck, posterior urethra, prostate (expressed on bladder neck contraction) |
Clot Characteristics
- Vermiform (worm-shaped) clots - formed in the upper tract (ureter/renal pelvis)
- Cuboid/amorphous clots - formed within the bladder
- Clots obstructing the upper tract cause colicky renal pain; clots in the bladder can cause urinary retention.
Transient vs. Persistent vs. Recurrent
- Transient: trauma, exercise, menstruation, catheterization
- Persistent: more likely structural pathology, infection, or malignancy
- Recurrent: consider IgA nephropathy, thin basement membrane disease, urolithiasis
3. Associated Symptoms (Pain vs. Painless)
Painless hematuria is the classic presentation of urothelial malignancy (bladder, ureteral, renal pelvis cancer) - this is an oncologic emergency until proved otherwise.
Painful hematuria - ask about:
- Colicky flank/loin pain radiating to groin - nephrolithiasis/ureterolithiasis
- Dysuria + frequency + urgency + fever - UTI or cystitis; pyelonephritis if febrile with flank pain
- Dull loin ache - renal parenchymal pathology (glomerulonephritis, hydronephrosis)
- Joint pain and skin rash - HSP (IgA vasculitis), SLE, other systemic vasculitis
- Abdominal/pelvic pain - trauma, mass lesion
4. Temporal Relationship to Other Events
- Preceded by pharyngitis or skin infection (1-2 weeks prior): post-streptococcal glomerulonephritis
- Concurrent with upper respiratory infection / same day as illness: IgA nephropathy (synpharyngitic hematuria - onset within 24-48 hours of URTI, unlike PSGN's 1-2 week lag)
- Recent vigorous exercise (>10 km running): exercise-induced hematuria - typically resolves with rest, can be of renal or bladder origin
- Recent trauma or catheterization: urothelial injury
- Recent pelvic radiation: radiation cystitis
5. Risk Factors for Urothelial Malignancy
These are the most important cancer-screening questions:
| Risk Factor | Clinical note |
|---|---|
| Age >50 | Strongest demographic risk for bladder cancer |
| Smoking history | Single biggest modifiable risk factor for bladder cancer |
| Industrial/occupational chemical exposure | Aromatic amines (dye, rubber, leather, paint industries) |
| Alkylating chemotherapy (cyclophosphamide, ifosfamide) | Hemorrhagic cystitis; increases transitional cell carcinoma risk |
| Analgesic abuse (phenacetin, NSAIDs) | Papillary necrosis, analgesic nephropathy |
| Chronic foreign body in urinary tract (chronic indwelling catheter) | Squamous cell carcinoma risk |
| Pelvic radiation | Radiation cystitis, secondary malignancy |
| Schistosomiasis (travel to endemic areas) | Squamous cell carcinoma of bladder |
6. Past Medical History
- Prior episodes of hematuria - when, evaluated, any diagnosis?
- Known nephrolithiasis or passage of gravel
- Renal disease (glomerulonephritis, polycystic kidney disease, chronic kidney disease)
- Diabetes - risk of papillary necrosis
- Sickle cell disease or trait - papillary necrosis (sickling in renal medulla)
- Coagulopathy or bleeding disorders - note: anticoagulation at therapeutic levels does NOT cause hematuria; finding hematuria in an anticoagulated patient still requires full workup
- Hypertension - renal parenchymal disease
- Autoimmune disease (SLE, vasculitis)
- Recurrent UTIs
7. Drug History
Drugs that can cause hematuria or mimic it:
- NSAIDs - papillary necrosis, interstitial nephritis
- Anticoagulants (warfarin, heparin, DOACs) - hematuria in these patients is NOT benign and still requires workup
- Penicillin, diuretics, anticonvulsants - interstitial nephritis
- Cyclophosphamide - hemorrhagic cystitis
- Chlorpromazine - urinary discoloration
- Rifampicin, nitrofurantoin, isoniazid - red-brown urine discoloration (pseudohematuria)
8. Family History
This is particularly important and often overlooked:
| Family history | Suggests |
|---|---|
| Hematuria | Thin basement membrane disease, Alport syndrome, IgA nephropathy |
| Sensorineural deafness + hematuria | Alport syndrome (X-linked COL4A5 mutation) |
| Ocular disorders | Alport syndrome |
| Progressive renal failure / dialysis / transplant | Hereditary nephropathy |
| Nephrolithiasis | Inherited stone disease (hypercalciuria, cystinuria, hyperuricosuria) |
| Hemoglobinopathy (sickle cell) | Papillary necrosis |
| Coagulopathy, bleeding tendency | Blood dyscrasia |
| Polycystic kidney disease | ADPKD |
| Hypertension and renal failure | Alport syndrome, ADPKD |
9. Social and Travel History
- Occupation: dye/rubber/paint/leather industries (aromatic amine exposure)
- Travel to Sub-Saharan Africa, Middle East, South America: Schistosoma haematobium - causes terminal painless hematuria
- Exercise habits: long-distance running - exercise hematuria
- Menstrual history (females): rule out contamination of urine specimen with menstrual blood
10. Review of Systems
Ask specifically about:
- Fever, weight loss, night sweats (malignancy, TB, endocarditis)
- Skin rash - purpuric in HSP, butterfly rash in SLE
- Joint pain/swelling - SLE, HSP, vasculitis
- Hearing loss, visual problems - Alport syndrome
- Edema (periorbital, lower limb) - nephrotic/nephritic syndrome
- Hypertension, headache - glomerulonephritis
- Symptoms of prostatism (older males) - BPH, prostate cancer
Summary: Key Diagnostic Clues from History
| History feature | Most likely cause |
|---|---|
| Painless gross hematuria, age >50, smoker | Bladder cancer (urothelial) |
| Colicky flank pain, prior stones | Nephrolithiasis |
| Post-URTI (same day), young male | IgA nephropathy |
| Post-strep infection (1-2 wk delay) | Post-streptococcal GN |
| Deafness + hematuria + family history | Alport syndrome |
| Travel to Africa, terminal hematuria | Schistosomiasis |
| Exercise, resolves with rest | Exercise-induced hematuria |
| Dysuria + frequency + fever | UTI/pyelonephritis |
| Rash + arthralgia | HSP, SLE, vasculitis |
| Sickle cell disease / analgesic abuse / diabetes | Papillary necrosis |
| Cyclophosphamide use | Hemorrhagic cystitis |
Sources:
- Campbell-Walsh-Wein Urology, 12e, Ch. 2 (Evaluation of the Urologic Patient)
- NKF Primer on Kidney Diseases, 8e, Ch. 5
- Tintinalli's Emergency Medicine, 9e, Ch. 89
- Rosen's Emergency Medicine, 9e, Ch. 168
This is a shared conversation. Sign in to Orris to start your own chat.