A case of 70Y/Male with no past commorbidities with gross hematuria, how to approach
Reading File
Finding Sources
Searching PubMed
gross hematuria evaluation diagnosis
Searching the Web
gross hematuria 70 year old male workup approach AUA guidelines 2024
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Now I have sufficient comprehensive information to compile a thorough, well-structured clinical answer. Let me now deliver the full response.
Approach to Gross Hematuria in a 70-Year-Old Male
This is a high-risk presentation that demands a structured, urgent urologic workup. In a male >50 years with gross hematuria, bladder cancer must be excluded first - it is the most common cause in this demographic. The cancer detection rate in gross hematuria is ~23-40%, far higher than in microscopic hematuria (3-5%).
Step 1 - Confirm True Hematuria
Before anything else, rule out pseudohematuria:
- Obtain a clean midstream urine sample
- Send for microscopic urinalysis (not just urine dipstick)
- Dipstick: sensitivity 91-100% but specificity only 65% - can be falsely positive with myoglobinuria, hemoglobinuria, beet ingestion, rifampicin, phenazopyridine
- Confirm RBCs on microscopy (>3 RBCs/HPF = confirmed hematuria)
Also examine RBC morphology:
- Dysmorphic/crenated RBCs + RBC casts = glomerular origin (nephrology referral)
- Normal/isomorphic RBCs = lower urinary tract / non-glomerular bleeding (urologic workup)
Step 2 - Focused History
Key questions to ask:
| Feature | Significance |
|---|---|
| Timing in stream (initial, total, terminal) | Initial = urethral/prostatic; Terminal = bladder neck/trigone; Total = kidney/ureter/bladder |
| Clots present? Shape? | Vermiform (worm-shaped) clots = upper tract; Cuboid clots = bladder |
| Pain? | Painless gross hematuria = bladder cancer until proven otherwise; Colicky flank pain = urolithiasis |
| Smoking history | Major risk factor for urothelial carcinoma |
| Occupational/chemical exposure | Aromatic amines, benzidine, aniline dyes - urothelial carcinogens |
| LUTS (frequency, urgency, dysuria) | Irritative symptoms can suggest CIS (carcinoma in situ) |
| Anticoagulant/antiplatelet use | Does NOT cause hematuria per se - full workup still required |
| Prior pelvic radiation | Risk for radiation cystitis + secondary malignancy |
| Cyclophosphamide use | Hemorrhagic cystitis / bladder cancer risk |
| Weight loss, anorexia | Systemic malignancy |
| Family history of GU cancers | Urothelial, RCC, Lynch syndrome |
Note: Anticoagulation use does NOT eliminate the need for full workup - hematuria on anticoagulation still requires complete urologic evaluation.
Step 3 - Physical Examination
- BP - hypertension may suggest glomerular disease
- Abdominal exam - palpable renal mass (RCC), pulsatile mass (AAA - life-threatening, must not be missed)
- Abdominal bruit - arteriovenous fistula
- CVA (costovertebral angle) tenderness - pyelonephritis, calculi
- Digital Rectal Exam (DRE) - prostate size, nodularity (10% of recurrent gross hematuria has prostate cancer)
- Genital exam - meatal/urethral lesion, perineal trauma
Step 4 - Initial Investigations
Urine
| Test | Purpose |
|---|---|
| Urine microscopy + culture | Confirm RBCs; exclude UTI (treat first if UTI, but if hematuria persists after treatment, full workup still needed) |
| Urine cytology | Recommended in gross hematuria (can detect high-grade urothelial carcinoma, CIS) |
| Spot urine protein:creatinine | If glomerular origin suspected |
Blood
| Test | Purpose |
|---|---|
| CBC | Anaemia, thrombocytopenia |
| RFTs (Creatinine, eGFR) | Renal function baseline |
| PT/INR, aPTT | Coagulopathy |
| PSA | In males - 10% of recurrent gross hematuria cases have prostate cancer |
| Serum electrolytes | Baseline |
Step 5 - Imaging (Upper Tract)
CT Urography (CTU) - Investigation of Choice
- Multi-phase CT: non-contrast + nephrographic + excretory (delayed) phase
- Best overall imaging for gross hematuria - detects:
- Urothelial tumors of renal pelvis and ureter
- Renal cell carcinoma
- Urolithiasis
- Hydronephrosis
- Renal cysts, trauma
- Detects ~90% of upper tract malignant lesions
- Standard of care per AUA guidelines for gross hematuria
If contrast contraindicated (allergy, poor renal function): MR Urography is an acceptable alternative
Renal-bladder ultrasound alone is not sufficient for gross hematuria (acceptable substitute only in low-risk microhematuria).
Step 6 - Cystoscopy (Mandatory)
- All patients with gross hematuria require cystoscopy - no imaging modality can adequately evaluate the bladder mucosa
- CT urography is not as sensitive as cystoscopy for bladder urothelial tumors
- Flexible cystoscopy preferred as an office procedure
- Allows direct visualization of:
- Bladder tumors (papillary, sessile, CIS)
- Bladder neck, trigone
- Ureteral orifices (looking for lateralizing hematuria - blood jetting from one orifice = upper tract lesion)
- Prostatic urethra
- Urethra
Step 7 - Special Considerations for This Patient (70M, No Comorbidities)
This patient is high risk by all stratification systems:
- Age >60 (strongest independent risk factor)
- Male sex
- Any episode of gross hematuria = automatic high-risk category regardless of other factors
Per the 2025 AUA/SUFU Guideline (updated from 2020):
- Any gross hematuria triggers complete urologic evaluation: CTU + cystoscopy + urine cytology
- Do NOT defer or watch - every episode must be investigated
- Even one negative urinalysis after gross hematuria does NOT eliminate need for workup
Differential Diagnosis (Most to Least Likely in This Context)
| Priority | Cause | Notes |
|---|---|---|
| 1st | Bladder urothelial carcinoma | Most common cause of gross hematuria in men >50; 85% present with painless hematuria |
| 2nd | Renal cell carcinoma | Hematuria + flank pain + mass = classic triad (rarely all 3 present) |
| 3rd | Urolithiasis | Usually with colicky pain; clots may be present |
| 4th | Upper tract urothelial carcinoma | Renal pelvis/ureter; vermiform clots |
| 5th | BPH with prostate bleeding | Increased prostate vascularity; but must exclude malignancy |
| 6th | Prostate cancer | DRE + PSA |
| 7th | Radiation/hemorrhagic cystitis | History usually clarifies |
| 8th | Glomerulonephritis / IgA nephropathy | Dysmorphic RBCs, casts, proteinuria, HTN |
| 9th | Renal infarction / AVM | Less common |
| 10th | AAA / vascular | Rare but life-threatening - pulsatile mass = urgent imaging |
Diagnostic Algorithm Summary
Gross Hematuria (70Y Male)
↓
Rule out pseudohematuria (urine microscopy)
↓
Confirm UTI? → Treat → Re-check → If persists → Full workup
↓
History + Physical + DRE + PSA
↓
Labs: CBC, RFTs, coagulation, urine cytology, urine culture
↓
CT Urography (upper tract imaging)
↓
Cystoscopy (mandatory, regardless of CTU findings)
↓
├─ Mass/filling defect on CTU → Urologic oncology referral
├─ Bladder tumor on cystoscopy → TURBT + staging
├─ Lateralizing hematuria from ureteral orifice → Retrograde pyelogram + ureteroscopy
└─ All negative → Consider nephrology referral (glomerular workup)
Key Clinical Pearls
- Painless gross hematuria in a male >50 = bladder cancer until proven otherwise
- Even a single episode must be fully investigated - hematuria is often intermittent
- Anticoagulation is not an excuse to skip workup - it does not cause hematuria, it unmasks it
- Risk of malignancy on gross hematuria evaluation: ~20-40% vs 3-5% for microscopic hematuria
- 85% of newly diagnosed bladder cancers present with painless gross hematuria
- PSA should be considered - 10% of recurrent gross hematuria cases have prostate cancer
- If negative workup: low risk of malignancy for next 3-5 years, but any new gross hematuria triggers repeat full evaluation
Sources: Campbell Walsh Wein Urology 3-Volume Set, p. 96-106 | ROSEN's Emergency Medicine, p. 1920-1980 | Campbell Walsh Wein Urology, p. 4571-4575 (Detection of Urothelial Carcinoma) | AUA/SUFU Microhematuria Guideline 2025 | AUA Medical Student Curriculum: Hematuria
52Y male, s/p partial gastrectomy in his 25th pod, presented with coffee ground vomitus, what will be the approach
Reading File
Finding Sources
Finding Sources
Searching the Web
post gastrectomy day 25 coffee ground vomiting upper GI bleed approach management anastomotic ulcer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive data to write a thorough, structured response. Let me compile it.
Approach to Coffee Ground Vomitus in a 52Y Male, 25 Days Post-Partial Gastrectomy
This is a post-operative upper GI bleed (UGIB) in a surgically altered patient. The context of POD 25 (day 25 post-op) places this firmly in the "delayed/late post-operative hemorrhage" category. Coffee ground vomitus indicates altered blood - oxidized hemoglobin from a bleeding source that has been in contact with gastric acid, pointing to the gastric remnant or anastomotic site as the likely origin.
Step 1 - Immediate Assessment: Is the Patient Stable or Unstable?
This is the most critical first branch point and determines everything that follows.
Signs of Hemodynamic Instability:
- HR >100 bpm (tachycardia)
- SBP <90 mmHg or postural drop >20 mmHg (orthostatic hypotension)
- Cold peripheries, poor capillary refill
- Altered consciousness, confusion
- Urine output <0.5 mL/kg/hr
Immediate Actions (ALL Patients):
- 2 large-bore IV cannulas (≥18G) or large-bore central cordis
- Oxygen - high flow via face mask
- Draw blood urgently: CBC, LFTs, RFTs, coagulation profile, blood group and crossmatch, serum electrolytes, ABG
- Urinary catheter - monitor urine output hourly
- ECG - rule out ischaemic event triggered by hemorrhage
- Nil by mouth
- If hematemesis ongoing + reduced consciousness = consider elective intubation (to protect airway before endoscopy)
Step 2 - Resuscitation
Fluid and Transfusion Strategy:
| Scenario | Action |
|---|---|
| Active bleeding + hemodynamic instability | Immediate resuscitation - do NOT wait for labs to start |
| Hb <7 g/dL | Transfuse packed RBCs |
| Active ongoing hemorrhage | Transfuse based on hemodynamics, not Hb level alone |
| Stable, not actively bleeding | Restrictive strategy - transfuse only if Hb <7 g/dL (shown to reduce rebleeding + mortality) |
| Coagulopathy / INR >1.5 | Fresh frozen plasma |
| Platelets <50,000 | Platelet transfusion |
ICU Admission Criteria:
- Active bleeding (hematemesis, bright red blood via NGT, or hematochezia)
- Hemodynamic instability not rapidly corrected by fluids
- Requires monitoring and close observation
Step 3 - Risk Stratification Scoring
Glasgow-Blatchford Score (pre-endoscopy, helps triage):
| Variable | Included |
|---|---|
| Systolic BP, BUN, Hb, pulse | Yes |
| Melena, syncope | Yes |
| Hepatic disease, cardiac failure | Yes |
- Score ≥1 = needs inpatient management and endoscopy
- Maximum 23; higher = greater risk of rebleeding/death
Rockall Score (complete = pre + post-endoscopy):
| Variable | Included |
|---|---|
| Age, shock, comorbidities | Pre-endoscopy (Clinical Rockall) |
| Endoscopic diagnosis + stigmata | Post-endoscopy (Complete Rockall) |
- Complete score ≤2 = low risk; score ≥8 = high risk of mortality
- Scores 5+ have ~40% rebleeding risk
Step 4 - Differential Diagnosis in This Context (POD 25 Post-Partial Gastrectomy)
This patient has altered anatomy - key considerations are specific to post-gastrectomy state:
| Priority | Cause | Mechanism | Notes |
|---|---|---|---|
| 1st | Anastomotic / Marginal Ulcer | Ischemia, suture tension, acid injury to jejunal mucosa | Most common cause of delayed post-gastrectomy bleeding (after POD 3-5); Roux-en-Y particularly susceptible |
| 2nd | Staple/suture line bleeding | Direct vessel disruption | More common in early period (<24h), but can recur; "herald bleed" possible |
| 3rd | Stress ulcer (gastric remnant) | Physiological stress of major surgery → mucosal ischemia | Day 25 = stress ulcer prophylaxis may have been discontinued |
| 4th | Anastomotic leak with secondary hemorrhage | Septic collection erodes adjacent vessels | Look for fever, peritonism, tachycardia, sepsis signs |
| 5th | Secondary vascular erosion | Septic collections near divided vessels (left gastric, splenic, hepatic artery) | Catastrophic, life-threatening - "sentinel bleed" before massive hemorrhage |
| 6th | Recurrent / residual peptic ulcer disease | Underlying reason for original gastrectomy | H. pylori, NSAID use |
| 7th | Mallory-Weiss tear | Repeated retching/vomiting post-op | Relatively benign, often self-limiting |
| 8th | Gastric remnant cancer | Anastomotic recurrence if original surgery was for cancer | Less likely at POD 25, but important long-term |
| 9th | Bile reflux gastritis | Especially Billroth II / Roux-en-Y | Chronic, not usually acute bleed |
| 10th | Coagulopathy (DIC, anticoagulant overuse) | Perioperative coagulation disorder | Check coagulation profile |
Special danger - Secondary Hemorrhage from vascular erosion: Bailey and Love specifically warns that "septic collections along with radical vascular dissection may lead to catastrophic secondary hemorrhage from exposed or divided blood vessels - very difficult to manage whether reoperation or interventional radiology is employed." This is the most feared complication.
Step 5 - Pre-Endoscopy Optimization
Proton Pump Inhibitors (PPI):
- Start IV PPI immediately - do not wait for endoscopy
- Options:
- IV PPI bolus every 12 hours (stable patients)
- IV PPI continuous infusion (80 mg bolus then 8 mg/hr) - for high-risk / active bleeding; shown to significantly reduce rebleeding rate
- PPI neutralizes gastric acid → stabilizes blood clots → promotes hemostasis
Prokinetics (to improve endoscopic visualization):
- IV Erythromycin 250 mg over 20-30 min, given 20-90 minutes before endoscopy
- Mechanism: motilin receptor agonist → promotes gastric emptying → clears blood/clots from view
- Evidence: improves visualization (77% vs 51%), reduces need for repeat endoscopy (15% vs 26%)
- Monitor QTc - erythromycin can cause QT prolongation; check for drug interactions (CYP3A4 inhibitor)
- Alternative: Metoclopramide 10 mg IV
NGT Placement:
- Can be considered to aspirate gastric contents and confirm active bleeding, but NOT mandatory
- Bright red blood or "coffee grounds" in NGT confirms upper GI source
Step 6 - Upper GI Endoscopy (OGD)
Endoscopy is the cornerstone of diagnosis AND treatment.
Timing:
| Stability | Timing |
|---|---|
| Unstable | Resuscitate first → endoscopy when hemodynamically stable (do not rush to scope an actively crashing patient without airway protection) |
| Stable | Within 24 hours (urgent - within 12 hours if ongoing active bleed suspected) |
Challenges in Post-Gastrectomy Anatomy:
- Altered anatomy (Billroth I, Billroth II, Roux-en-Y) affects scope navigation
- Expert endoscopist essential - standard scopes may not access all areas
- In Roux-en-Y: the gastric pouch, Roux limb, anastomosis, and excluded duodenum are all accessible
- Side-viewing duodenoscope or enteroscope may be needed to evaluate Billroth II afferent limb
- Risk of anastomotic disruption and perforation with air insufflation - use CO2 insufflation if available, minimize insufflation
Endoscopic Findings and Their Management:
| Finding | Forrest Classification | Action |
|---|---|---|
| Active arterial spurting | Ia | Dual therapy - injection (1:10,000 adrenaline) + mechanical (clip) or thermal |
| Active oozing | Ib | Injection + clip or thermal coagulation |
| Visible non-bleeding vessel | IIa | Endoscopic therapy (high rebleeding risk ~43-55%) |
| Adherent clot | IIb | Attempt clot removal + treat underlying vessel |
| Flat pigmented spot | IIc | Conservative - no endoscopic therapy needed |
| Clean base ulcer | III | No endoscopic therapy - very low rebleeding risk (<5%) |
Endoscopic Hemostatic Options:
- Injection therapy - 1:10,000 adrenaline (epinephrine) - vasoconstriction + tamponade
- Thermal coagulation - heater probe, argon plasma coagulation (APC)
- Mechanical clips (hemostatic clips, over-the-scope clips - OTSC)
- Hemostatic powders (TC-325/Hemospray) - useful for anastomotic ulcer bleeding, but temporary only - not monotherapy
- Endoscopic suturing - for massive bleeding marginal ulcers
Note: Forrest Ia/Ib + IIa lesions require endoscopic therapy. Monotherapy with adrenaline alone is no longer recommended - use dual therapy (adrenaline + clip or thermal).
Step 7 - If Endoscopy Fails or Cannot Be Performed
Interventional Radiology (IR) - Angiographic Embolization:
- CT Angiography (CTA) first - identifies bleeding source if bleed rate ≥0.5 mL/min
- Transcatheter Arterial Embolization (TAE) - preferred over surgery when feasible
- Particularly useful for:
- Post-gastrectomy vascular erosion/secondary hemorrhage
- Bleeding marginal ulcer that failed endoscopy
- Bleeding from named vessels (left gastric, gastroduodenal, splenic artery)
- Success rate: ~70-90% in acute non-variceal UGIB
Surgery (Last Resort):
Indications for emergency surgical intervention:
- Endoscopy failed or not technically feasible
- Angioembolization failed or unavailable
- Massive bleeding - hemodynamically unstable despite resuscitation
- Anastomotic leak with secondary hemorrhage (peritonism + sepsis)
- Erosion into a named vessel (splenic, left gastric, middle colic)
Surgical options:
- Gastroenterotomy + transluminal oversewing of bleeding vessel
- Resection of anastomotic region (segmental jejunal resection + additional gastrectomy) - more definitive
- Reoperation carries significantly increased risk - closer to total gastrectomy; underscores importance of non-surgical management first
Step 8 - Specific Post-Op Considerations
| Issue | Action |
|---|---|
| Anastomotic leak? | Check drain output, fever, peritonism, CRP; CT abdomen with contrast if suspected |
| Stress ulcer prophylaxis | Ensure IV PPI or sucralfate was given post-operatively; may have been missed |
| H. pylori status | Check if eradicated; if untreated H. pylori - prescribe triple/quadruple therapy after acute bleeding settles |
| NSAIDs / anticoagulants | Withhold all NSAIDs - they impair mucosal defense and platelet function; review anticoagulation need |
| Nutritional status | Likely nutritionally depleted at POD 25 - early nasojejunal feeding or TPN while NBM |
| Sepsis screen | Blood cultures, CRP, PCT, WBC - if secondary hemorrhage from vascular erosion, may need urgent imaging + IR |
Management Algorithm Summary
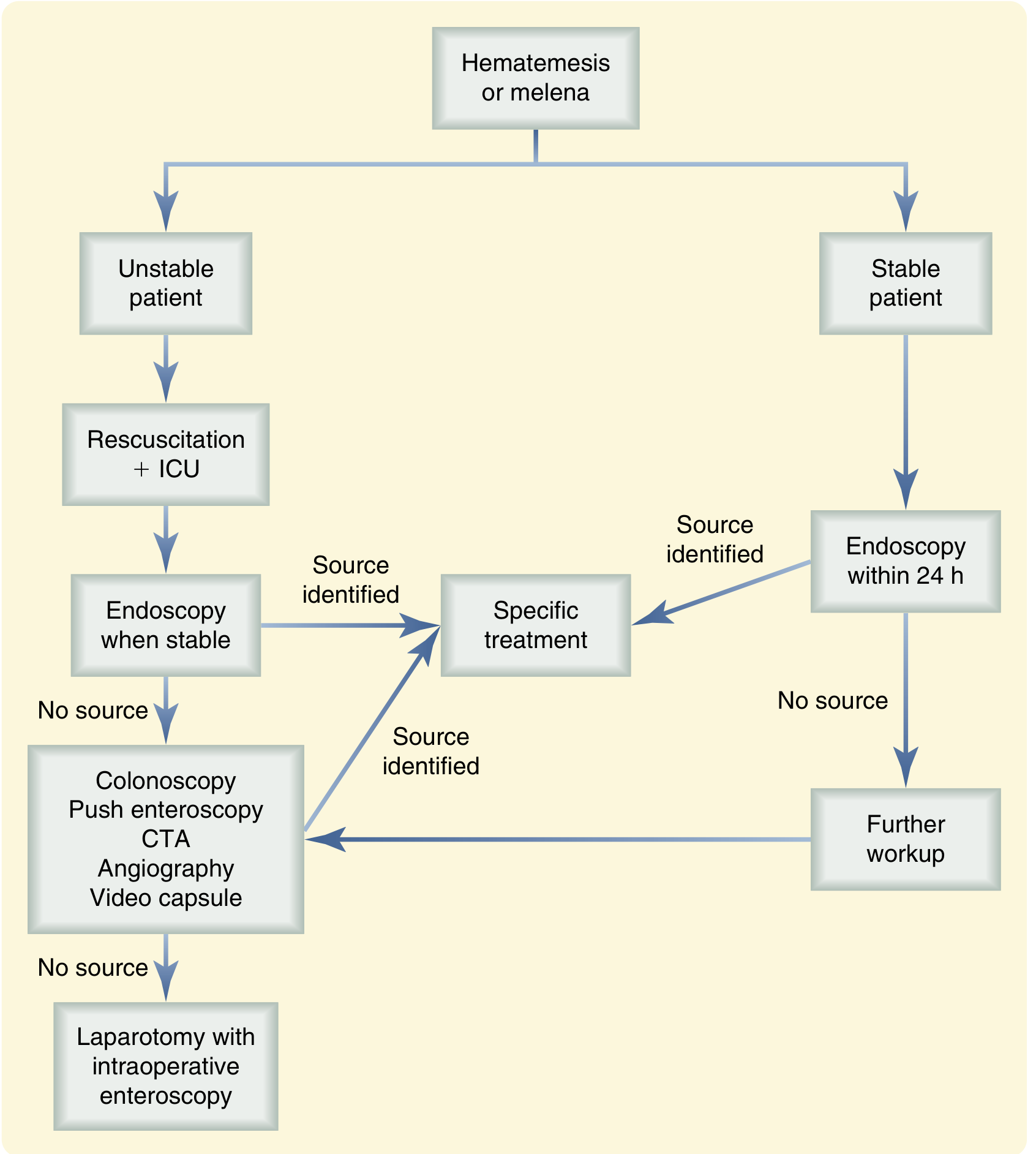
Algorithm for UGIB - Sabiston Textbook of Surgery
52Y Male, POD 25 Post-Partial Gastrectomy, Coffee Ground Vomitus
↓
Immediate Assessment: Stable or Unstable?
↓
┌───────────────────────────────────────────┐
│ UNSTABLE STABLE │
│ → 2x large-bore IV → 2x IV access│
│ → Fluid resuscitation → Labs │
│ → ICU admission → Risk score │
│ → Consider intubation │ │
└──────────────┬──────────────┘ │
↓ ↓
IV PPI + IV Erythromycin 250mg (30 min before scope)
↓
URGENT UPPER GI ENDOSCOPY (within 12-24h)
↓
┌──────────────────────────────────────────────────────┐
│ Endoscopy reveals: │
│ • Anastomotic/Marginal ulcer → Forrest classification│
│ → Dual endoscopic therapy (clip + adrenaline) │
│ • Stress ulcer in remnant → Thermal/clip │
│ • Mallory-Weiss tear → Usually self-limiting │
│ • Anastomotic disruption → Surgical consult │
│ • No source found → CTA + Angiography │
└──────────────────────────────────────────────────────┘
↓
Post-endoscopy IV PPI infusion (8 mg/hr × 72h)
↓
Rebleed? → Repeat endoscopy × 1
↓ (fails)
IR Angioembolization
↓ (fails)
Surgery - oversew / anastomotic resection
Key Points to Remember
- POD 25 bleed = delayed hemorrhage - most likely cause is anastomotic/marginal ulcer (ischemia, suture material, acid injury to unprotected jejunal mucosa)
- Coffee grounds = altered blood in gastric acid - not massively brisk, but DO NOT be falsely reassured - it can precede a larger "herald bleed"
- Endoscopy is both diagnostic and therapeutic - but requires expertise in altered anatomy
- IV PPI and IV Erythromycin before scope - improves visualization and reduces rebleeding
- Restrictive transfusion (Hb <7) is preferred in stable patients - shown to reduce mortality
- Septic secondary hemorrhage must always be considered in the post-gastrectomy patient with signs of sepsis - this is catastrophic and requires IR/surgery
- Anticoagulants and NSAIDs should be withheld - they do not cause bleeding but can perpetuate it
- H. pylori - test and treat; long-term PPI after any ulcer complication post-gastrectomy
- Reoperation carries significant morbidity - always exhaust non-surgical options first
Sources: Sabiston Textbook of Surgery, p. 2185-2190 | Current Surgical Therapy 14e, p. 3041-3049 (Marginal and Recurrent Ulcer) | Bailey and Love's Short Practice of Surgery 28e, p. 1197 (Post-gastrectomy complications) | Maingot's Abdominal Operations, p. 242 | Endoscopic Management of Bleeding in Altered Anatomy - MDPI Medicine 2023
This is a shared conversation. Sign in to Orris to start your own chat.