how to assess in detail in pediatrics in detailed step by step
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a detailed, step-by-step guide to pediatric assessment — structured specifically for physiotherapy students who need a thorough clinical picture.
Pediatric Assessment: Complete Step-by-Step Guide
STEP 1 — First Impression: The Pediatric Assessment Triangle (PAT)
Before touching the child, assess from the doorway in seconds. The PAT gives you a rapid "sick vs. not sick" determination.
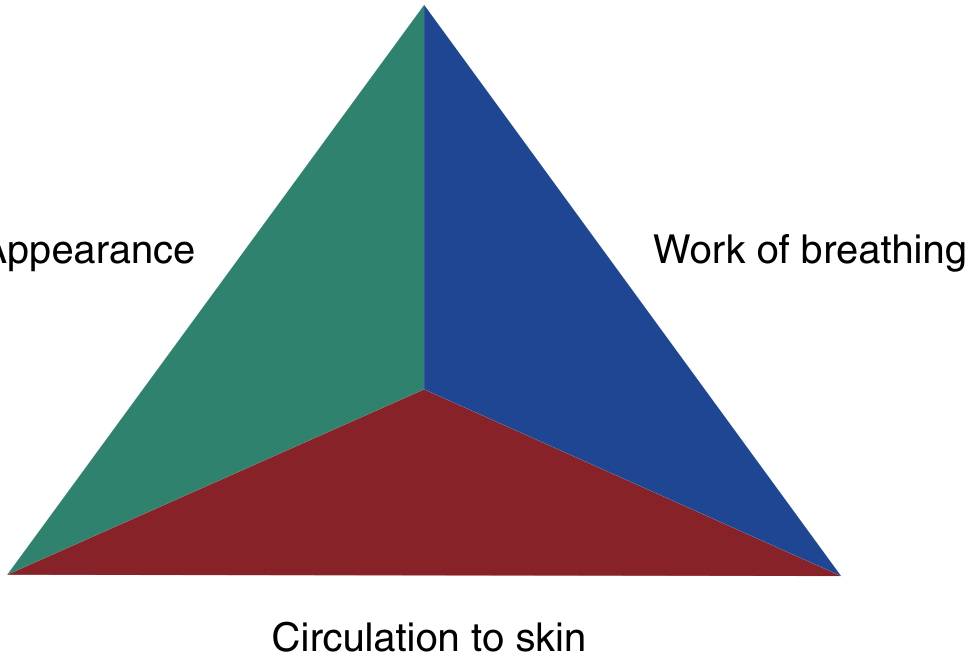
The three sides of the triangle:
1. Appearance (TICLS)
| Component | What to observe |
|---|---|
| Tone | Is the infant floppy? Poor muscle tone? |
| Interactivity | Is the child alert, aware of surroundings? Or irritable/unresponsive? |
| Consolability | Can a parent console the child, or is distress inconsolable? |
| Look/Gaze | Normal tracking of faces/objects? Or vacant stare? |
| Speech/Cry | Strong cry? Or weak/absent cry to stimuli? |
2. Work of Breathing
- Abnormal sounds: stridor, grunting, snoring, wheezing
- Abnormal positioning: sniffing position, tripod posture, refusal to lie flat
- Retractions (subcostal, intercostal, supraclavicular)
- Head bobbing (especially in infants)
- Nasal flaring
3. Circulation to the Skin
- Pallor
- Mottling
- Cyanosis (central or peripheral)
- Capillary refill time >2 seconds
- Petechiae
A normal PAT = stable child. Any abnormality guides your urgency and focus. — Rosen's Emergency Medicine, p. 3069
STEP 2 — Vital Signs (Age-Adjusted)
Pediatric vital signs are age-dependent. Applying adult norms to children leads to missed triage and errors.
| Age | Heart Rate (bpm) | RR (breaths/min) | Systolic BP (mmHg) |
|---|---|---|---|
| Neonate (0–1 mo) | 100–160 | 30–60 | 60–90 |
| Infant (1–12 mo) | 90–150 | 25–40 | 70–100 |
| Toddler (1–3 yr) | 80–130 | 20–30 | 80–110 |
| Preschool (3–6 yr) | 70–120 | 20–25 | 80–110 |
| School age (6–12 yr) | 65–110 | 15–20 | 85–120 |
| Adolescent (>12 yr) | 60–100 | 12–20 | 90–130 |
Key points:
- Tachycardia is the earliest sign of cardiovascular compromise — but may also reflect fever, pain, or anxiety. Assess at rest.
- Hypotension is a late sign of shock in children. Do not wait for hypotension to act.
- Bradycardia in an ill child = ominous sign of impending cardiopulmonary failure.
- Weight-based dosing is mandatory — always record weight in kilograms.
STEP 3 — History Taking
3a. SAMPLE History (Emergency/Quick Focused)
Use when time is limited:
| Letter | Meaning |
|---|---|
| S | Signs and Symptoms |
| A | Allergies |
| M | Medications |
| P | Past medical history |
| L | Last meal/fluid intake |
| E | Events leading to illness or injury |
3b. Full Pediatric History (Comprehensive)
1. Presenting Complaint
- Chief complaint in the caregiver's own words
- In preverbal children, symptoms are inferred from behavior — parents are highly perceptive of subtle behavioral changes
2. History of Presenting Complaint
- Onset, duration, progression
- Aggravating and relieving factors
- Associated symptoms (fever, vomiting, decreased feeding, rash, etc.)
3. Birth & Neonatal History (critical for neonates and infants)
- Gestational age, mode of delivery
- Complications during labor/delivery
- Maternal fever during labor, prolonged rupture of membranes, maternal Group B Streptococcus (GBS) status
- APGAR scores
- NICU admission, oxygen/ventilator use
- Newborn screening results (metabolic disorders, hypothyroidism, hearing)
4. Feeding History
- Breastfed or formula-fed
- Introduction of solids, current diet
- In infants: number of wet diapers/day — key indicator of hydration status (especially in breastfed newborns where intake is hard to quantify)
5. Growth and Development
- Growth milestones: weight gain trajectory, height
- Developmental milestones: gross motor, fine motor, speech/language, social
- Screen for regression — loss of previously attained milestones is significant
6. Immunization History
- Up to date? Which vaccines received?
- Critical in febrile infants (bacteremia risk) and children with rash (measles, varicella)
7. Past Medical History
- Previous illnesses, hospitalizations, surgeries
- Chronic conditions (asthma, cardiac disease, epilepsy, etc.)
8. Medications and Allergies
- Current medications (note: all doses are weight-based in children)
- Drug allergies and nature of reaction
9. Family History
- Relevant genetic conditions, cardiac disease, sudden death in young relatives
10. Social History (age-specific)
- Living situation, primary caregivers
- School/daycare attendance
- For adolescents (asked privately, without parent): sexual history, drug/alcohol/e-cigarette use, mental health, risk-taking behaviors
- Safeguarding concerns (child maltreatment)
STEP 4 — Physical Examination (Head-to-Toe)
Approach by Age — This is critical
| Age Group | Strategy |
|---|---|
| Neonate/Infant | Examine on parent's lap, warm hands, keep warm, examine most disturbing parts last (mouth, ears) |
| Toddler (1–3 yr) | Most difficult — stranger anxiety is peak; approach slowly, use distraction, examine with child on parent's lap; leave uncomfortable procedures last |
| Preschool (3–6 yr) | Use play, let them handle equipment first; explain simply what you're doing |
| School age (6–12 yr) | Explain findings, involve child in examination |
| Adolescent | Examine like adults, offer privacy, confirm preference for parent presence or absence, respect modesty |
General Inspection
- State of alertness, interaction with environment
- Nutritional status, hygiene, signs of neglect
- Dysmorphic features (unusual facial features, limb anomalies)
- Obvious distress, posture, spontaneous movement
Airway Assessment
- Patency: any stridor, drooling, inability to swallow?
- In infants: the head is proportionally large — neutral or slight extension (not hyperextension) maintains airway; use a shoulder roll under infants to align
- The tongue is proportionally large; obligate nose-breathers up to ~3–6 months
- Any hoarseness or muffled voice?
Respiratory Assessment
- Inspection: rate (count for full 60 seconds in infants), depth, symmetry, use of accessory muscles
- Retractions: subcostal, intercostal, suprasternal, supraclavicular
- Palpation: chest wall movement, tracheal position
- Percussion: dullness (consolidation/effusion), hyperresonance (pneumothorax/hyperinflation)
- Auscultation: air entry bilaterally, added sounds (wheeze, crackles, diminished)
- Note: Breath sounds transmit easily through a child's thin chest wall — auscultate carefully and systematically
Cardiovascular Assessment
- Heart rate: note if at rest (a crying child's HR is unreliable — leave pulse oximeter on until calm)
- Pulse quality: central (femoral, brachial in infants) vs. peripheral — thready peripheral pulse + tachycardia = shock
- Capillary refill time (CRT): press for 5 seconds, release — normal <2 seconds
- Auscultation: heart sounds, murmurs
- Blood pressure: age-appropriate cuff size is mandatory
- Children compensate by vasoconstriction before losing BP — look for cold extremities + tachycardia as early shock signs
Abdominal Assessment
- Inspection: distension, visible peristalsis, umbilicus
- Auscultation first (before palpation): bowel sounds
- Palpation: start away from the area of pain; use the child's hand under yours to reduce guarding in toddlers; assess for organomegaly (liver, spleen), masses, tenderness
- Percussion: tympany, dullness over organomegaly/ascites
Neurological Assessment
- Level of consciousness: use AVPU (Alert, Voice, Pain, Unresponsive) or GCS (age-modified)
- Fontanelle (infants): anterior fontanelle normally closes by 18 months
- Bulging = raised ICP; Sunken = dehydration
- Pupils: size, symmetry, reaction to light
- Tone: assess at rest — hypotonia vs. hypertonia
- Reflexes: deep tendon reflexes; primitive reflexes in neonates (Moro, rooting, grasp, stepping)
- Developmental reflexes: expected to disappear at specific ages — their persistence is abnormal
- Gait (ambulatory children): symmetry, posture, base width, heel-toe
Musculoskeletal Assessment (especially relevant for physio students)
- Inspect for deformity, swelling, asymmetry
- Palpate bones and joints for tenderness, warmth, swelling
- Range of motion (active and passive)
- Physeal injuries: children's ligaments are stronger than their growth plates — suspect growth plate fracture even with normal X-ray if physis is tender
- Limping: age-based differential (DDH, Perthes, slipped capital femoral epiphysis, septic arthritis)
- Scoliosis screen: Adams forward bend test
- Foot alignment: flat feet normal until ~3 years; tibial torsion; toe walking
- Note: Greater degrees of fracture angulation are acceptable in children due to bone remodeling capacity
Skin Assessment
- Color: cyanosis, jaundice, pallor, mottling, petechiae
- Rashes: distribution, morphology (macular, papular, vesicular, petechial)
- Bruising: location and pattern — accidental bruising typically on shins/forehead; unexplained or patterned bruising raises safeguarding concerns
- Turgor: pinch test for dehydration (though less reliable in obese children)
- Capillary refill at forehead, sternum, fingertips
ENT Assessment
- Ears: otoscopy — tympanic membrane appearance (erythema, effusion, perforation)
- Eyes: conjunctiva (pallor = anaemia, injection = infection), sclera (jaundice), red reflex
- Nose: flaring, secretions
- Throat: pharyngeal erythema, tonsillar enlargement/exudate — examine last in toddlers as most distressing
- Lymph nodes: cervical, axillary, inguinal — size, tenderness, mobility
Genitourinary
- Assess as indicated
- For neonates: check external genitalia, undescended testes, hypospadias
- Document Tanner staging in adolescents when relevant
STEP 5 — Developmental Assessment (Milestones)
As a physio student, this is especially important. Assess across 4 domains:
| Age | Gross Motor | Fine Motor | Language | Social |
|---|---|---|---|---|
| 2 months | Lifts head prone | Hands unfisted | Coos, social smile | Recognizes parents |
| 4 months | Rolls front to back | Grasps rattle | Laughs | Smiles spontaneously |
| 6 months | Sits with support | Transfers objects | Babbles | Stranger awareness |
| 9 months | Pulls to stand | Pincer grip emerging | "Mama/dada" nonspecific | Waves bye |
| 12 months | Walks with support | Pincer grip | 1–2 words with meaning | Separation anxiety |
| 18 months | Walks well | Stacks 2–3 blocks | 10–20 words | Parallel play |
| 2 years | Runs, kicks ball | Stacks 6 blocks | 2-word phrases | Symbolic play |
| 3 years | Climbs stairs alternating | Copies circle | Sentences | Group play |
| 5 years | Hops, skips | Copies square/triangle | Fluent speech | Cooperative play |
Red flags for gross motor delay (physio relevance):
- Not rolling by 6 months
- Not sitting independently by 9 months
- Not walking by 18 months
- Persistent toe walking after 2–3 years
- Asymmetric movement (hemiplegia)
- Loss of previously achieved milestones at any age
STEP 6 — Immunologic and Risk Stratification
- Young infants (<1 month) with fever have ≥10% risk of serious bacterial infection — treat as high risk regardless of appearance
- Vaccination status modifies risk (e.g., vaccinated children have lower bacteremia risk from H. influenzae, Streptococcus pneumoniae)
- Premature infants have adjusted developmental age for milestones (use corrected age up to 2 years)
STEP 7 — Documentation and Communication
- Record weight in kilograms always
- Document age in appropriate units: days (neonates), months (infants/toddlers), years (older children)
- For physiotherapy: clearly document:
- Functional mobility level
- Gross motor developmental stage
- Pain assessment using age-appropriate scale (FLACC for <3 yrs, Wong-Baker FACES for 3–7 yrs, NRS for ≥8 yrs)
- Caregiver/parent input on baseline function
Summary: Sequence at a Glance
- PAT → First impression from doorway (sick/not sick)
- Vital signs → Age-adjusted interpretation
- History → SAMPLE + detailed age-specific history
- Head-to-toe exam → Adapt approach to age/development
- Developmental screen → Milestones across 4 domains
- Risk stratification → Age, vaccination, prematurity
- Document → Kg weight, corrected age, functional baseline
Sources: Rosen's Emergency Medicine — Concepts and Clinical Practice, pp. 3066–3072; The Harriet Lane Handbook, 23rd ed.
as per this in deatil i want and demonstartions in detail everhing
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
This is a shared conversation. Sign in to Orris to start your own chat.