Malaria
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent — both diagrams are clear and highly informative. I now have everything needed for a comprehensive overview. Here is the full synthesis:
Malaria
Overview
Malaria is a potentially life-threatening parasitic disease caused by protozoa of the genus Plasmodium, transmitted exclusively by the bite of female Anopheles mosquitoes. The WHO estimated >200 million cases and >600,000 deaths in 2020, with the greatest burden in sub-Saharan Africa and parts of Asia. With widespread jet travel, cases now appear worldwide.
Five species infect humans:
| Species | Disease | Notes |
|---|---|---|
| P. falciparum | Falciparum (tertian) malaria | Most dangerous; high fatality; no hypnozoite |
| P. vivax | Benign tertian malaria | Dormant hypnozoite → relapse |
| P. ovale | Ovale malaria | Dormant hypnozoite → relapse |
| P. malariae | Quartan malaria | Mild; long latency |
| P. knowlesi | Knowlesi malaria | Zoonosis (primates); can be severe; SE Asia |
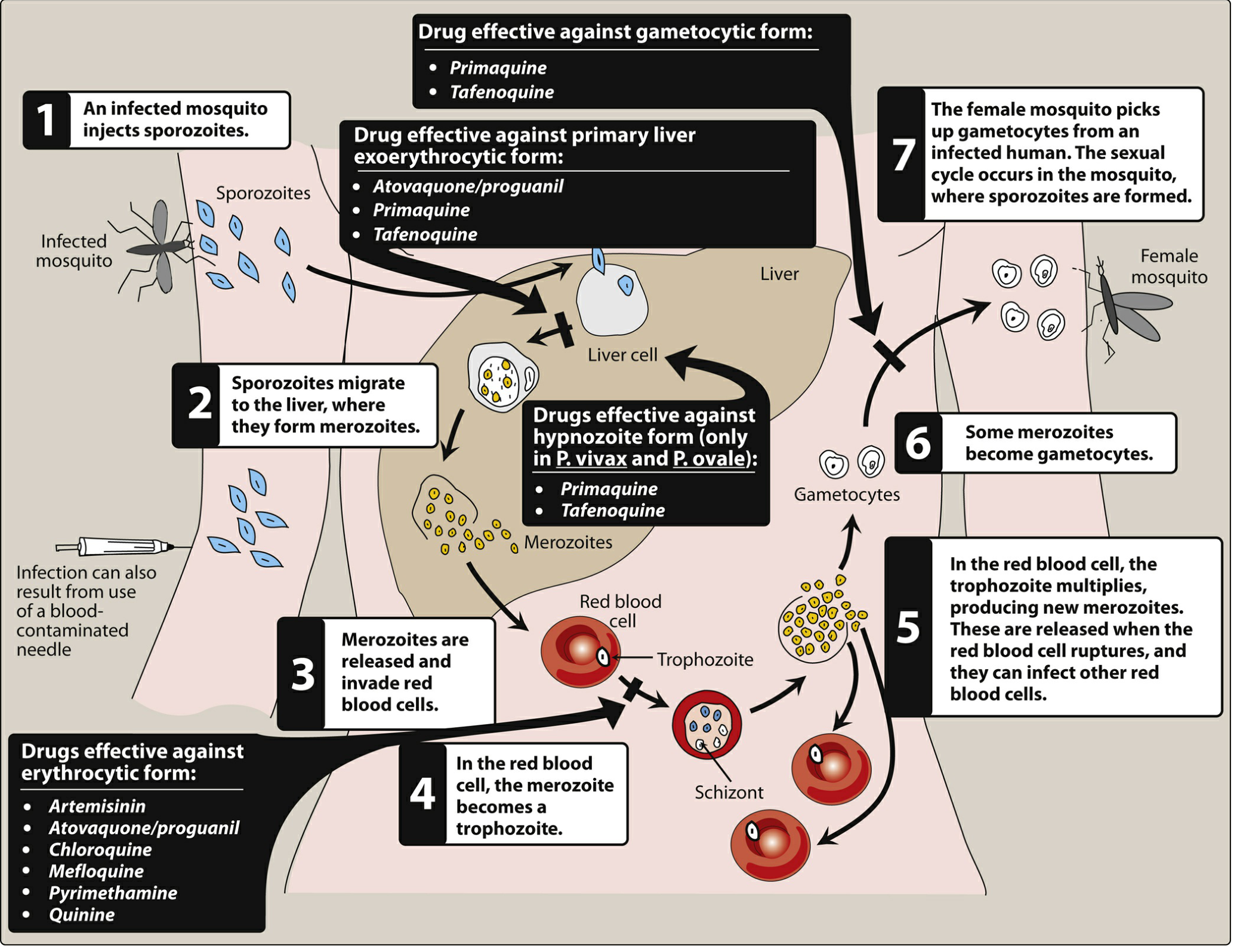
Life Cycle

Hepatic (pre-erythrocytic) stage:
- An infected Anopheles mosquito injects sporozoites into the bloodstream.
- Sporozoites travel to the liver within minutes, using thrombospondin-related adhesive protein and circumsporozoite protein to bind hepatocyte heparan sulfate proteoglycans.
- Inside hepatocytes, sporozoites differentiate into merozoites (incubation 1–4 weeks), then hepatocytes rupture and merozoites are released.
- In P. vivax and P. ovale, some parasites enter a dormant hypnozoite stage in the liver — the basis for relapses months to years later.
Erythrocytic stage:
- A lectin-like molecule on merozoites binds sialylated glycophorin on red blood cells (RBCs), allowing invasion into a "digestive" vacuole.
- Merozoites differentiate into ring trophozoites, then mature trophozoites.
- Trophozoites either become gametocytes (sexual forms; restart cycle in mosquito) or differentiate into schizonts.
- P. falciparum schizonts express PfEMP1 on knob-like extensions on the RBC surface, which binds endothelial adhesion molecules (ICAM-1, VCAM-1, CD36), causing sequestration in capillary beds — the key pathogenic mechanism of severe disease.
- Schizonts lyse the RBC, releasing new merozoites → repeat cycle every 48–72 hours.
— Robbins & Kumar Basic Pathology, p. 392
Pathogenesis of Severe Disease (P. falciparum)
The capillary sequestration caused by PfEMP1 drives most severe complications, which typically appear at parasitemia >100,000 organisms/mm³:
- Cerebral malaria: delirium, seizures, coma, paralysis; ~80% mortality when combined with pulmonary insufficiency
- Acute respiratory distress (pulmonary malaria)
- Splanchnic involvement: vomiting, abdominal pain, bloody diarrhea
- Acute kidney injury
- Jaundice (haemolysis + hepatic involvement)
- Severe anaemia (haemolysis from repeated RBC lysis)
Most deaths in falciparum malaria occur within 3 days.
— Sherris & Ryan's Medical Microbiology, p. 1701–1705
Clinical Features
Classic presentation: headache and fatigue → fever, chills, sweats in paroxysms. The periodicity reflects synchronised RBC lysis:
- Every 48 hours — P. falciparum, P. vivax, P. ovale
- Every 72 hours — P. malariae
P. falciparum typically causes persistent high fever without clear paroxysms, hyperparasitemia, and rapid multiorgan dysfunction.
Diagnosis
- Peripheral blood smear (gold standard): thick and thin smears stained with Giemsa or Wright stain. Thick smear concentrates parasites; thin smear allows species identification. Multiple specimens may be needed.
- Acridine orange / QBC tubes: faster, requires fluorescence microscope; poor speciation.
- Rapid antigen tests:
- ParaSight F: detects HRP2 protein of P. falciparum; >95% sensitivity
- OptiMAL: detects parasite lactate dehydrogenase; distinguishes P. falciparum from P. vivax
- PCR assays: high sensitivity and speciation; used in reference labs
- Serology: epidemiological use; occasionally helpful for speciation
— Sherris & Ryan's Medical Microbiology, p. 1705
Treatment
Complete treatment requires eliminating parasites at three levels:
- Erythrocytic schizonts → ends the clinical attack
- Hepatic schizonts / hypnozoites → prevents relapse
- Gametocytes → prevents transmission
No single drug does all three. The diagram below maps drugs to life cycle stages:
Key Antimalarial Drugs
| Drug | Stage targeted | Notes |
|---|---|---|
| Chloroquine | Erythrocytic | Drug of choice for P. vivax, P. malariae, P. ovale (where sensitive); widespread P. falciparum resistance |
| Artemisinin / artemisinins | Erythrocytic | Rapidly acting; backbone of artemisinin-based combination therapy (ACT) for P. falciparum |
| Atovaquone/proguanil (Malarone) | Erythrocytic + primary liver stage | Used for treatment and prophylaxis |
| Mefloquine | Erythrocytic | Used where chloroquine-resistant P. falciparum |
| Quinine | Erythrocytic | IV for severe P. falciparum |
| Pyrimethamine | Erythrocytic | Antifolate; used in combination |
| Primaquine | Hypnozoites (liver) + gametocytes | Mandatory to prevent relapse in P. vivax and P. ovale; contraindicated in G6PD deficiency (causes haemolytic anaemia) |
| Tafenoquine | Hypnozoites + gametocytes + primary liver stage | Single-dose alternative to primaquine for P. vivax radical cure; also contraindicated in G6PD deficiency |
Resistance is the major challenge, particularly multi-drug-resistant P. falciparum. Artemisinin partial resistance has emerged in Southeast Asia and Africa.
— Lippincott Illustrated Reviews: Pharmacology, p. 1167–1170
Prevention
- Vector control: insecticide-treated bed nets, indoor residual spraying
- Chemoprophylaxis (for travellers):
- Atovaquone/proguanil, mefloquine, or doxycycline — choice depends on destination resistance patterns
- Chloroquine for travel to chloroquine-sensitive areas
- Vaccine: RTS,S/AS01 (Mosquirix) — first approved malaria vaccine, targets P. falciparum sporozoites; moderate efficacy (~50%)
Key Points Summary
- P. falciparum is the deadliest species due to capillary sequestration via PfEMP1
- P. vivax and P. ovale have hypnozoites requiring primaquine/tafenoquine for radical cure (G6PD screen first)
- Diagnosis: Giemsa-stained blood smear ± rapid antigen test ± PCR
- Severe malaria is a medical emergency requiring IV artesunate
- Drug resistance, especially in P. falciparum, shapes treatment selection by geographic region
This is a shared conversation. Sign in to Orris to start your own chat.