Malaria
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Excellent — I now have all the material needed for a comprehensive clinician-level reference. Here is the full synthesis:
Malaria — Comprehensive Clinical Reference
1. Epidemiology
The WHO estimated >200 million cases worldwide in 2020, resulting in over 600,000 deaths. Malaria is endemic across sub-Saharan Africa and Asia; with global travel, cases appear worldwide. Humans are the only natural reservoir for the species that infect them.
— Robbins & Kumar Basic Pathology, p. 392
2. Causative Organisms
Five Plasmodium species infect humans:
| Species | Disease | Fever Cycle | Notes |
|---|---|---|---|
| P. falciparum | Tertian (falciparum) malaria | 48 h | Most dangerous; chloroquine-resistant in most regions |
| P. vivax | Benign tertian malaria | 48 h | Hypnozoite relapse; some chloroquine resistance |
| P. ovale | Benign tertian malaria | 48 h | Hypnozoite relapse |
| P. malariae | Quartan malaria | 72 h | Chronic nephropathy |
| P. knowlesi | Zoonotic malaria | 24 h | SE Asia; can be severe |
All are transmitted by the bite of female Anopheles mosquitoes.
3. Life Cycle & Pathogenesis

FIG. 10.8 — Life cycle of P. falciparum (Robbins & Kumar Basic Pathology)
Hepatic (exoerythrocytic) stage
- The mosquito inoculates sporozoites into the bloodstream
- Sporozoites bind to hepatocytes via thrombospondin-related adhesive protein and circumsporozoite protein (binding heparan sulfate proteoglycans)
- Within 1–4 weeks, sporozoites differentiate into merozoites inside hepatocytes
- Infected hepatocytes rupture, releasing merozoites into blood
- P. vivax and P. ovale can form dormant hypnozoites in the liver — the source of relapses months to years later
Erythrocytic stage
- A lectin-like molecule on the merozoite surface binds sialylated glycophorin on RBCs → invagination into a digestive vacuole
- Merozoites differentiate into trophozoites → schizonts
- Schizonts express PfEMP1 (knob-like extensions on RBC surface), which binds endothelial adhesion molecules (ICAM-1, VCAM-1, CD36) → cytoadherence and microvascular sequestration
- After ~48 h, schizonts differentiate into new merozoites → RBC lysis → next cycle
- Some trophozoites become gametocytes — taken up by another mosquito to restart the sexual cycle
— Robbins & Kumar Basic Pathology, p. 392
4. Pathology & Morphology
- Hemolytic anemia — destruction of RBCs; severity varies by species
- Malarial pigment (hematin/hemozoin) — brown pigment derived from hemoglobin degradation; deposits in spleen, liver, lymph nodes, bone marrow
- Splenomegaly (often massive) and hepatomegaly — from hyperplasia of mononuclear phagocytes
- Cerebral malaria (P. falciparum) — small cerebral vessels engorged and occluded by PfEMP1-mediated cytoadherence; rapidly progressive with convulsions, coma, death
- Blackwater fever — massive intravascular hemolysis → hemoglobinemia, hemoglobinuria, jaundice, renal failure (complication of P. falciparum)
- Nephrotic syndrome — particularly with P. malariae (quartan malaria nephropathy)
Each species shows a distinctive trophozoite morphology on Giemsa-stained thick blood smears, allowing expert species identification.
— Robbins & Kumar Basic Pathology, p. 392
5. Clinical Features
| Feature | Detail |
|---|---|
| Classic presentation | Headache and fatigue → episodic rigors, fever, sweating, prostration |
| Fever periodicity | 24 h (P. knowlesi), 48 h (P. falciparum, P. vivax, P. ovale), 72 h (P. malariae) |
| Hemolytic anemia | Universal; degree varies by species and parasitemia load |
| Cerebral malaria | P. falciparum; convulsions, impaired consciousness, coma; fatal within days if untreated |
| Blackwater fever | Massive hemolysis, hemoglobinuria, AKI — P. falciparum |
| Relapsing malaria | Months–years after apparent cure — P. vivax, P. ovale (hypnozoites) |
| Hyperparasitemia | P. falciparum — hallmark of severe disease; >5% parasitized RBCs |
— Lippincott Illustrated Reviews: Pharmacology; Robbins & Kumar Basic Pathology
6. Diagnosis
- Thick and thin blood smears (Giemsa stain) — gold standard; thick smear for detection, thin smear for species ID
- Rapid antigen tests — HRP2 (P. falciparum), pan-malaria LDH
- PCR — most sensitive; species and resistance genotyping
- CBC — thrombocytopenia, anemia, leukopenia common
- LFTs, creatinine, blood glucose — assess severity and complications
7. Treatment & Pharmacology
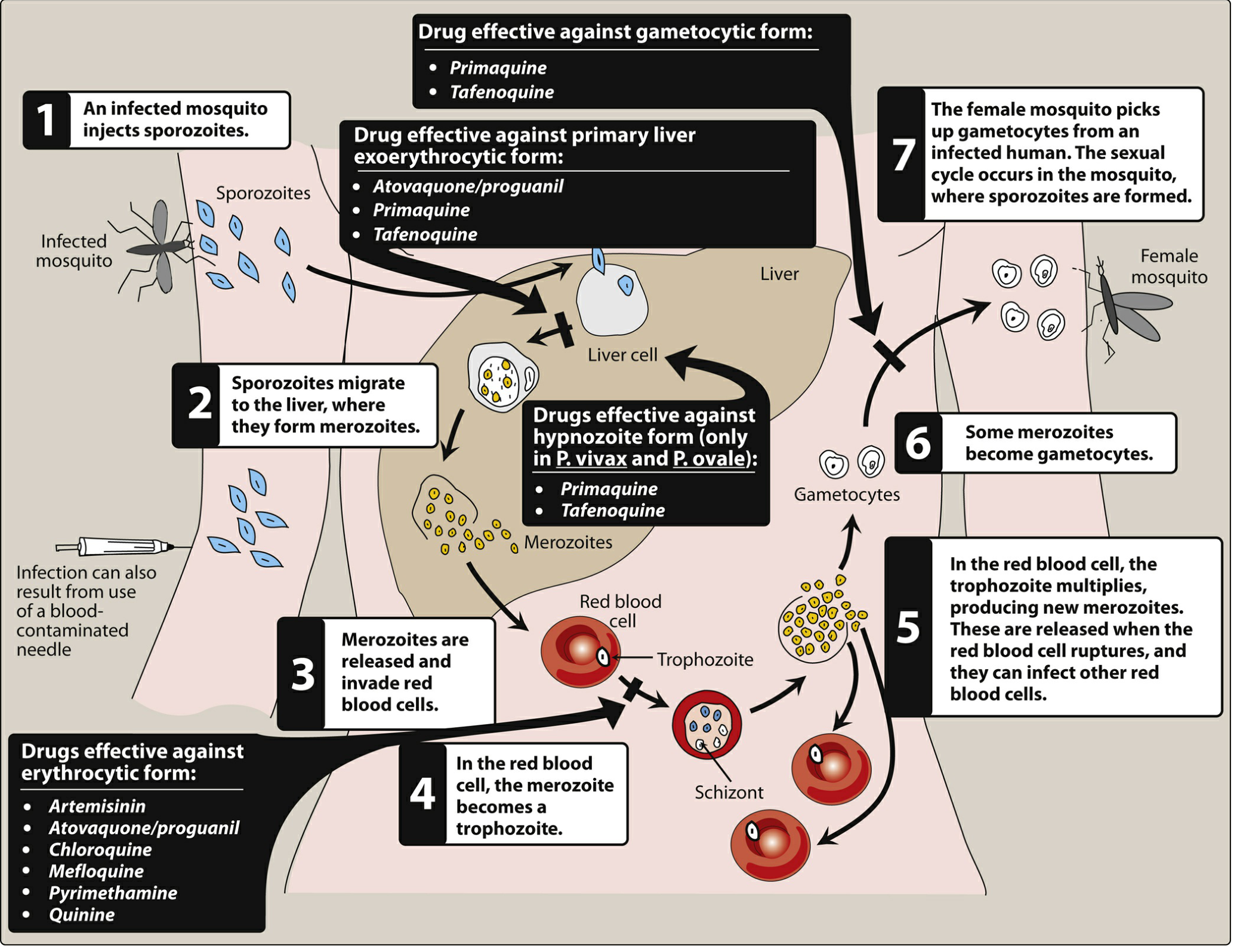
Figure 35.5 — Sites of action of antimalarial drugs (Lippincott Illustrated Reviews: Pharmacology)
Guiding principles (Goldman-Cecil)
- Most drugs act on erythrocytic (blood) stages
- Drug choice depends on species and regional resistance patterns
- Artemisinin-based combination therapy (ACT) — e.g., artemether-lumefantrine — is first-line for acute malaria from chloroquine-resistant areas
- Chloroquine — treatment and prophylaxis only where Plasmodium remains sensitive (very limited geography for P. falciparum)
- Primaquine and tafenoquine are the only agents that eradicate liver hypnozoites (P. vivax, P. ovale)
— Goldman-Cecil Medicine, p. 3381
Key Drug Summary
| Drug | Stage Targeted | Mechanism | Key Toxicities / Notes |
|---|---|---|---|
| Artemisinin/derivatives (artemether, artesunate) | Erythrocytic | Reactive oxygen species generation after iron-mediated cleavage; rapid schizonticide | Drug of choice for severe/resistant falciparum; use always in combination (ACT) |
| Lumefantrine | Erythrocytic | Inhibits heme polymerization | Only used with artemether; QT prolongation |
| Chloroquine | Erythrocytic | Accumulates in parasite vacuole; inhibits heme polymerization to hemozoin → toxic heme accumulates | Resistance near-universal for P. falciparum; retinal toxicity with long-term use; QT prolongation |
| Mefloquine | Erythrocytic | Inhibits hemozoin formation | CNS side effects (vivid dreams, psychosis); use declining |
| Atovaquone-proguanil (Malarone) | Erythrocytic + primary liver stage | Atovaquone blocks mitochondrial electron transport (cytochrome bc1); proguanil inhibits DHFR | Prophylaxis and treatment for chloroquine-resistant areas |
| Quinine/quinidine | Erythrocytic | Inhibits hemozoin formation | IV quinidine/quinine for severe malaria; cinchonism; hypoglycemia |
| Primaquine | Liver (primary + hypnozoites) + gametocytes | Oxidative disruption of mitochondria | G6PD deficiency must be tested before use — causes hemolytic anemia; contraindicated in pregnancy |
| Tafenoquine | Liver (hypnozoites) + gametocytes | Similar to primaquine (8-aminoquinoline) | Single-dose for P. vivax radical cure; G6PD testing mandatory; not for acute treatment |
| Pyrimethamine | Erythrocytic | DHFR inhibition | Used in combination regimens; rarely as monotherapy |
| Doxycycline | Erythrocytic | Inhibits apicoplast protein synthesis | Prophylaxis for chloroquine-resistant areas; not for children <8 y or pregnancy |
— Lippincott Illustrated Reviews: Pharmacology, pp. 1167–1177
Radical Cure (Preventing Relapse)
For P. vivax and P. ovale, treatment must include a hypnozoitocidal agent to prevent relapse:
- Primaquine 15 mg/day × 14 days (or 30 mg/day × 7 days)
- Tafenoquine single dose (450 mg) — requires G6PD quantitative testing prior to administration
Severe/Cerebral Malaria
- IV artesunate is first-line
- IV artesunate superior to IV quinine (fewer adverse effects, faster parasite clearance)
- Adjunctive care: maintain glucose (quinine causes hypoglycemia), control seizures, manage fluid balance carefully (risk of ARDS and cerebral edema)
8. Prophylaxis
Travelers to endemic areas — selected based on destination resistance profile:
| Drug | Regimen | Use Case |
|---|---|---|
| Atovaquone-proguanil | Daily, start 1–2 d before, 7 d after | Chloroquine-resistant areas |
| Doxycycline | Daily, start 1–2 d before, 4 wk after | Chloroquine-resistant areas |
| Mefloquine | Weekly, start 2 wk before, 4 wk after | Chloroquine-resistant areas (where mefloquine-sensitive) |
| Chloroquine | Weekly | Only chloroquine-sensitive areas (limited) |
| Tafenoquine | Weekly + single terminal dose | Includes hypnozoite coverage for P. vivax |
Country-specific recommendations: CDC Travelers' Health (www.cdc.gov/travel/)
9. Resistance
- Chloroquine resistance in P. falciparum: near-universal globally (mediated by mutations in pfcrt and pfmdr1 — chloroquine efflux from parasite vacuole)
- Partial artemisinin resistance emerging in Southeast Asia (kelch13 mutations); managed by switching ACT partner drugs
- P. vivax chloroquine resistance documented in parts of SE Asia and Oceania
10. Prevention (Public Health)
- Insecticide-treated bed nets
- Indoor residual spraying
- Elimination of standing water (larval breeding sites)
- RTS,S/AS01 (Mosquirix) — first approved malaria vaccine; targets circumsporozoite protein of P. falciparum; partial protection (~30–56%), deployed in sub-Saharan Africa for children; expected to prevent thousands of cerebral malaria deaths
- R21/Matrix-M — newer vaccine with higher efficacy (~75%) now approved in several endemic countries
— Robbins & Kumar Basic Pathology, p. 392; Goldman-Cecil Medicine
Key Sources:
- Robbins & Kumar Basic Pathology, p. 391–393
- Goldman-Cecil Medicine (International Ed.), p. 3381
- Lippincott Illustrated Reviews: Pharmacology, pp. 1167–1177
CRL OF 66.3 cm corresponds to which month of pregnancy
Reading File
Finding Sources
Reading File
Reading File
I have everything needed. Here is the answer:
CRL of 66.3 mm → Gestational Age
Using the standard formula from obstetric ultrasound:
Gestational age (weeks) = (CRL [mm] + 65) / 10
Calculation:
(66.3 + 65) / 10 = 131.3 / 10 = 13.13 weeks
Result: approximately 13 weeks gestational age (by last menstrual period)
Converting to months
| Convention | Value |
|---|---|
| Obstetric months (4 weeks each) | ~3.3 months |
| Calendar months | ~3 months |
| Lunar months | ~3.3 lunar months |
This places the pregnancy at the end of the first trimester (12–14 weeks).
Important caveats
- CRL is most accurate for dating between 7–12 weeks. At ≥13 weeks, the fetus begins to flex and extend significantly, making it difficult to obtain the true maximal diameter — so CRL becomes less reliable beyond this point, and biparietal diameter (BPD), head circumference, femur length, and abdominal circumference become the preferred dating parameters.
- The formula gives gestational age from LMP (menstrual/obstetric age), which is 2 weeks ahead of embryologic (post-fertilization) age.
- Measurements should be averaged from three satisfactory sagittal images, measuring the longest straight-line dimension excluding limb buds and yolk sac.
— Pfenninger and Fowler's Procedures for Primary Care; The Developing Human: Clinically Oriented Embryology
NTEP
Finding Sources
Finding Sources
Finding Sources
Finding Sources
The library does not contain a dedicated NTEP chapter (this is an India-specific national health programme, not covered in the international textbooks in the library). I'll answer from established knowledge.
NTEP — National Tuberculosis Elimination Programme (India)
What is NTEP?
The National Tuberculosis Elimination Programme (NTEP) is India's government-run programme for TB control and elimination. It was renamed from RNTCP (Revised National TB Control Programme) to NTEP in 2020, reflecting the shift in goal — from control to elimination of TB by 2025 (ahead of the global SDG target of 2030).
- Nodal ministry: Ministry of Health & Family Welfare, Government of India
- Implemented through: Central TB Division (CTD)
Historical Evolution
| Year | Milestone |
|---|---|
| 1962 | National Tuberculosis Programme (NTP) launched |
| 1993 | RNTCP piloted (with World Bank support) |
| 1997 | RNTCP rolled out nationally |
| 2006 | Full national coverage achieved |
| 2012 | RNTCP Phase II — universal DST, private sector engagement |
| 2017 | National Strategic Plan (NSP) 2017–2025 — "End TB" target |
| 2018 | PM Modi's commitment: TB-mukt Bharat by 2025 |
| 2020 | RNTCP renamed NTEP |
Core Strategy
NTEP follows the WHO End TB Strategy, built on three pillars:
- Integrated, patient-centred care and prevention
- Bold policies and supportive systems
- Intensified research and innovation
Key Components of NTEP
1. Case Finding
- Presumptive TB cases identified at all health facilities
- Active case finding in high-risk groups (PLHIV, contacts, undernourished, diabetics, prisoners, etc.)
- Nikshay — national TB notification and patient management IT portal (mandatory notification of all TB cases, public and private)
2. Diagnosis
- CBNAAT/GeneXpert (Cartridge Based Nucleic Acid Amplification Test) — first-line molecular diagnostic at district level; detects TB + rifampicin resistance simultaneously
- TrueNat — chip-based PCR platform; deployable at PHC level
- LPA (Line Probe Assay) — rapid detection of MDR/XDR-TB
- Liquid culture (MGIT) — Drug susceptibility testing (DST) at Intermediate Reference Laboratories (IRLs)
- Sputum smear microscopy — still used for monitoring (not primary diagnosis)
- Chest X-ray with AI-assisted reading being scaled up
3. Treatment Regimens (as per NTEP 2022 guidelines)
Drug-Sensitive TB (DS-TB)
| Category | Regimen | Duration |
|---|---|---|
| New cases (pulmonary & extrapulmonary) | 2HRZE / 4HRE | 6 months |
| Previously treated | DST-guided; empirically 2HRZES/1HRZE/5HRE | 8 months |
- H = Isoniazid, R = Rifampicin, Z = Pyrazinamide, E = Ethambutol, S = Streptomycin
- Daily dosing (not intermittent) — moved away from thrice-weekly DOT
- Fixed Dose Combinations (FDCs) — weight-based dosing
Drug-Resistant TB (DR-TB)
| Type | Regimen |
|---|---|
| MDR-TB (Rif + INH resistant) | Shorter oral BPaL regimen or longer regimen (18–20 months) |
| Pre-XDR/XDR-TB | BPaL — Bedaquiline + Pretomanid + Linezolid (6 months) |
| RR-TB | Treated as MDR-TB |
- Bedaquiline and Delamanid — newer drugs available under NTEP for DR-TB
- Pretomanid — added for XDR-TB regimens
4. DOT (Directly Observed Treatment)
- Shifted to 99-DOTS (digital adherence monitoring via IVR/missed-call system)
- Medication given in sealed blister packs with unique codes — patient calls a number to confirm dose
- Reduces need for physical supervision while maintaining accountability
5. Nikshay Poshan Yojana (NPY)
- Direct Benefit Transfer (DBT) of ₹500/month to every notified TB patient for nutritional support throughout treatment
- Aims to address undernutrition — a major risk factor for TB in India
6. Pradhan Mantri TB Mukt Bharat Abhiyaan (PMTBMBA)
- Community-based initiative (2022) — enlisting Ni-kshay Mitras (donors/supporters — individuals, corporates, elected representatives) to adopt TB patients and provide nutritional, diagnostic, and vocational support
7. Preventive Therapy
- TB Preventive Therapy (TPT) for high-risk contacts:
- PLHIV: 6H (6 months isoniazid) or 3HP (3 months weekly isoniazid + rifapentine)
- Household contacts of bacteriologically confirmed TB cases (especially children <5 years and immunocompromised)
8. HIV-TB Co-management
- All TB patients tested for HIV (provider-initiated)
- All HIV-TB co-infected patients initiated on ART irrespective of CD4 count
- Co-trimoxazole preventive therapy given
NTEP Programme Structure
Central TB Division (CTD) — National level
↓
State TB Cell (STC) — State level
↓
District TB Centre (DTC) — District level
↓
Tuberculosis Unit (TU) — covers ~500,000 population
↓
DMC (Designated Microscopy Centre) / CBNAAT site
↓
PHC / Sub-centre / ASHA (community level)
Targets & Indicators
| Indicator | NTEP Target |
|---|---|
| Treatment Success Rate (DS-TB) | ≥90% |
| MDR-TB Treatment Success | ≥75% |
| TB Notification Rate | Increasing (all sources) |
| TB Incidence reduction | 80% reduction by 2025 (vs 2015 baseline) |
| TB Mortality reduction | 90% reduction by 2025 |
| Zero catastrophic costs for TB families | By 2025 |
Private Sector Engagement
- Mandatory notification — all TB cases must be notified on Nikshay (legal requirement under Notifiable Diseases)
- PPSA (Public-Private Support Agency) model
- Ni-kshay digital platform links private providers
- Ni-kshay drug supply — free FDCs provided to private sector patients
Key Drugs Available Free Under NTEP
| Drug Type | Drugs |
|---|---|
| First-line FDCs | HRZE (various weight bands) |
| Injectable (if still needed) | Amikacin, Kanamycin, Capreomycin |
| Newer oral DR-TB drugs | Bedaquiline, Delamanid, Linezolid, Clofazimine, Cycloserine, Pretomanid |
| Preventive | Isoniazid, Rifapentine |
India's TB Burden (Context)
- India accounts for ~26% of global TB burden (highest in the world)
- ~2.8 million estimated TB cases per year
- ~480,000 estimated deaths per year (pre-NTEP scale-up era)
- Significant co-morbidity load: DM + TB, malnutrition + TB, HIV + TB
Note: NTEP guidelines are regularly updated by the Central TB Division. The most current treatment algorithms are available at tbcindia.gov.in. The NTEP is not covered in the international medical textbook library available here, so this answer is based on established programme knowledge up to early 2025.
This is a shared conversation. Sign in to Orris to start your own chat.