Reading File
analyse_media
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a full explanation of this ultrasound report.
Ultrasound Abdomen Report - Explanation
Patient: Male, 42 years | Date: 14/7/2026
Hospital: Govt Headquarters Hospital, Karaikudi (Dept. of Radiodiagnosis)
What the Report Says (Finding by Finding)
| Organ | Finding | Meaning |
|---|---|---|
| Liver | Normal size, uniform echopattern, no focal/diffuse pathology, bile ducts not dilated | Liver structure is okay structurally, but see Impression below |
| Gall Bladder | Few calculi (stones) in the body, largest ~10 mm; wall thickness 4 mm (thickened) | Stones present with wall inflammation |
| Pancreas | Normal contour, echo, no calcifications, duct not dilated | Pancreas is fine |
| Spleen | Normal size and echo, no focal lesions | Fine |
| Right Kidney | Normal, no calculi, corticomedullary differentiation preserved | Fine |
| Left Kidney | Normal, no calculi, corticomedullary differentiation preserved | Fine |
| Urinary Bladder | Adequately filled, normal wall, no calculus/mass | Fine |
| Prostate | Normal volume | Fine |
| Free Fluid | None | No internal bleeding or ascites |
IMPRESSION (Diagnosis)
The radiologist has reported two conditions:
1. Grade I Fatty Liver
What it means:
Fat has deposited inside the liver cells (hepatocytes). Ultrasound grades fatty liver from I to III based on how bright (echogenic) the liver looks compared to the kidney:
- Grade I (Mild): Slight increase in liver brightness. The liver-kidney contrast is mildly increased. This is what this patient has.
- Grade II: Moderate brightness, blood vessels become less visible.
- Grade III: Severe, blood vessels nearly invisible.
Why does it happen?
This is most commonly Non-Alcoholic Fatty Liver Disease (NAFLD), associated with:
- Obesity (especially central/abdominal fat)
- Type 2 diabetes or pre-diabetes (insulin resistance)
- High triglycerides / low HDL cholesterol (dyslipidemia)
- Hypertension
- Metabolic syndrome
The underlying mechanism: insulin resistance causes fat (free fatty acids) to accumulate in the liver instead of being oxidized normally. - Robbins & Kumar Basic Pathology, p. 1910
Is it serious?
Grade I fatty liver is mild and often reversible with lifestyle changes. However, if untreated, it can progress:
NAFLD → Non-Alcoholic Steatohepatitis (NASH) → Fibrosis → Cirrhosis → rarely Liver Cancer
What to do:
- Weight loss (even 5-10% body weight helps significantly)
- Diet: reduce refined carbohydrates, sugar, and saturated fats
- Regular exercise
- Control blood sugar, blood pressure, and cholesterol
- Avoid alcohol completely
- No specific drug is universally approved yet; lifestyle change is the primary treatment
2. Acute (Mild) Calculus Cholecystitis
What it means:
This is acute inflammation of the gallbladder caused by gallstones (calculi).
The report shows:
- Calculi (stones) in the gallbladder body - largest is ~10 mm
- Gallbladder wall thickness of 4 mm (normal is ≤3 mm - this is thickened, confirming inflammation)
How it happens:
A stone obstructs the gallbladder neck or bile outflow. This causes:
- Build-up of bile → chemical irritation of the gallbladder wall
- Phospholipases break down bile fats into toxic compounds (lysolecithin)
- Bile salts damage the mucosal lining
- Prostaglandins released → more inflammation
- Eventually, bacterial infection can be superimposed
Robbins & Kumar Basic Pathology, p. 2596-2598
Here is what gallstones look like on ultrasound (arrows pointing to stones and thickened wall):
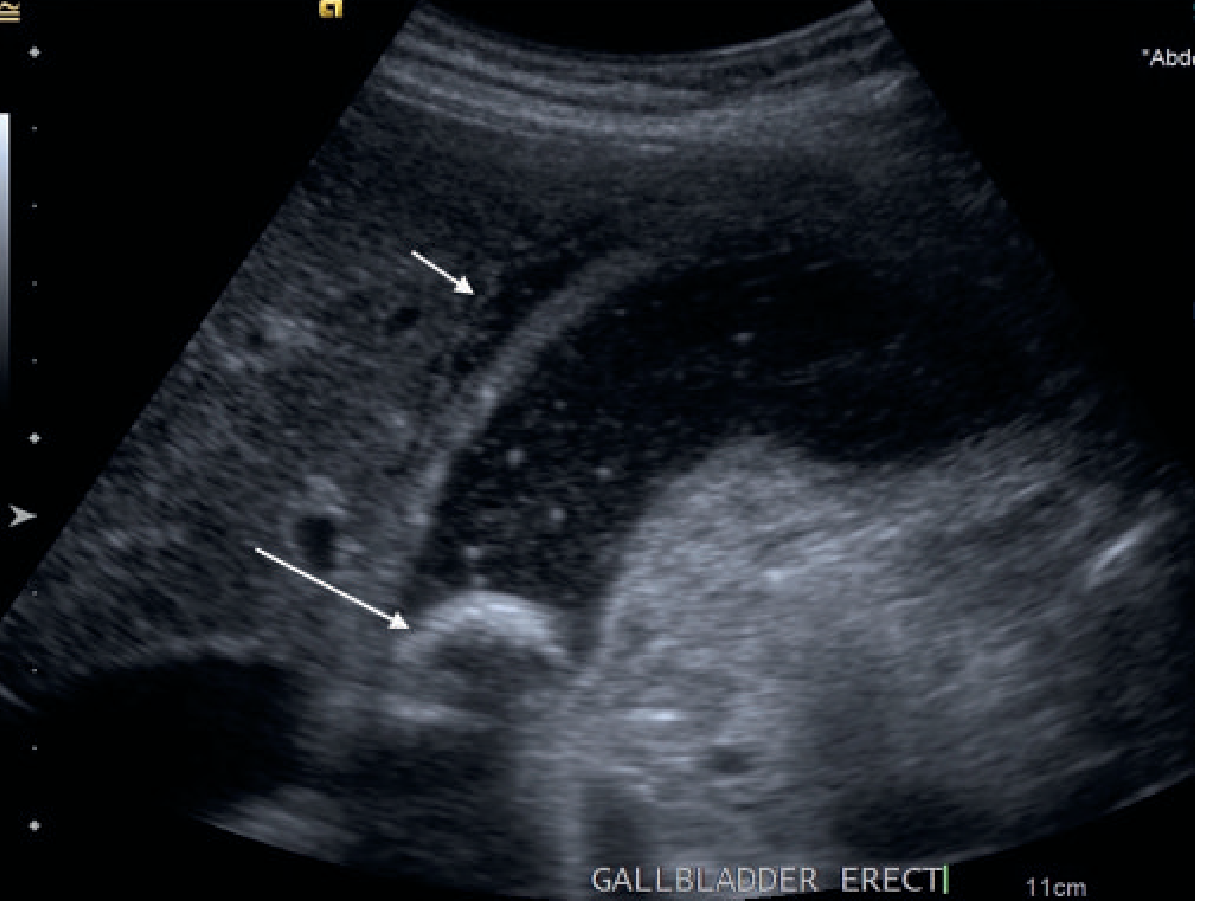
On ultrasound, the radiologist looks for:
- Gallstones present (yes - up to 10 mm stone)
- Gallbladder wall > 3 mm (yes - 4 mm here, confirming inflammation)
- Positive sonographic Murphy sign (pain when probe presses over gallbladder)
- Pericholecystic fluid (not mentioned here - hence "mild")
Grainger & Allison's Diagnostic Radiology, p. 1086
Is it serious?
Acute calculus cholecystitis is a surgical emergency in severe cases. This patient's case is described as mild, meaning:
- No pericholecystic fluid (no leakage)
- No gangrene or perforation signs
- Wall thickening is only slightly elevated (4 mm)
What to do (typical management):
- Immediate: Hospitalization, IV fluids, nil by mouth (NPO), pain relief (NSAIDs or opioids), antibiotics (e.g., cefuroxime + metronidazole)
- Definitive treatment: Laparoscopic cholecystectomy (surgical removal of the gallbladder) - this is the gold standard. For mild cases, it can be done within 72 hours of onset (early cholecystectomy) or electively after the acute episode settles.
- Avoid fatty meals until surgery is done.
Summary for the Patient
| Condition | Severity | Action Needed |
|---|---|---|
| Fatty Liver Grade I | Mild | Diet, exercise, weight loss; follow up in 6 months |
| Acute Calculus Cholecystitis (mild) | Mild-Moderate | See a surgeon promptly; likely needs gallbladder removal |
The most urgent issue here is the cholecystitis - the patient should consult a general surgeon as soon as possible. The fatty liver is a long-term concern managed through lifestyle modification.
Disclaimer: This explanation is for educational purposes. Please follow the treating doctor's advice for all medical decisions.
Is this serious
Based on this report, here is an honest, straightforward answer:
Is it serious?
The Cholecystitis (Gallbladder) — YES, needs prompt attention
This is the more urgent finding. Even though the radiologist says "mild," acute calculus cholecystitis is not something to ignore or delay treatment for.
Here is why:
- The gallbladder wall is already inflamed (thickened at 4 mm)
- There is a 10 mm stone obstructing normal bile flow
- If left untreated, it can progress to:
- Gangrenous cholecystitis (gallbladder tissue dies)
- Perforation (gallbladder bursts - life-threatening)
- Sepsis (infection spreads to blood)
The patient likely has or will develop: right upper abdomen pain (especially after eating fatty food), nausea, vomiting, and possibly fever.
Action: See a general surgeon within the next 24-48 hours. The standard treatment is surgical removal of the gallbladder (laparoscopic cholecystectomy). Delaying increases the risk of complications.
The Fatty Liver (Grade I) — NOT immediately dangerous, but a warning sign
- Grade I is the mildest stage - the liver is not damaged yet, just has fat in it
- It will not cause a crisis today or tomorrow
- BUT it is a warning that the metabolic health (weight, blood sugar, cholesterol) needs attention
- If ignored for years, it can silently progress to liver damage
Action: Lifestyle changes over the next few months - diet, exercise, weight control. No surgery needed.
Bottom Line
| Urgency | |
|---|---|
| Gallbladder (cholecystitis) | See a surgeon soon - within 1-2 days |
| Fatty liver (Grade I) | Not urgent today, but address within weeks-months |
The patient should not wait on the gallbladder issue, especially if there is abdominal pain, fever, or vomiting. Those symptoms would make it an emergency room visit immediately.
This is general medical information. The treating doctor makes the final call on urgency and treatment.
This is a shared conversation. Sign in to Orris to start your own chat.