Q. Discuss the etiopathology, clinical features and management of labrynthine fistula in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching Images
labyrinthine fistula lateral semicircular canal cholesteatoma
Loading Image
Loading Image
Loading Image
I now have comprehensive material from Cummings, KJ Lee, and clinical images. Let me compile the complete 50-mark answer.
LABYRINTHINE FISTULA — COMPREHENSIVE 50-MARK ESSAY
(RGUHS Examination Standard)
DEFINITION
A labyrinthine fistula is an erosive defect of the endochondral bone overlying the membranous labyrinth (semicircular canals, vestibule, or cochlea), without loss of perilymph into the middle ear — thereby distinguishing it from a perilymphatic fistula (which involves a breach of the endosteal membrane and actual perilymph leak). The protective bony shell of the otic capsule is lost, allowing pressure or mass-induced motion of the underlying endosteum, perilymph, and endolymphatic compartment, which evokes vestibular and sometimes auditory symptoms.
— Cummings Otolaryngology Head and Neck Surgery
INCIDENCE
| Parameter | Figure |
|---|---|
| Incidence in cholesteatoma cases | 7–10% (Gersdorff series; Cummings) |
| Lateral (horizontal) SCC involvement | ~98% of all fistulae |
| Associated facial nerve involvement | ~60% of labyrinthine fistula cases |
| Associated tegmen dehiscence | ~39% of labyrinthine fistula cases |
| Fistula test positivity | 30–50% of confirmed fistulae |
| Vertigo (subjective) | ~60% of patients with fistula |
| SNHL association | 60–70% (especially cochlear fistulae) |
— Cummings (Manolidis series, 111 patients); K.J. Lee's Essential Otolaryngology
ETIOPATHOLOGY
Primary Cause
Cholesteatoma is responsible for >95% of labyrinthine fistulae. Rarely, other destructive pathologies (tuberculosis, congenital anomalies, osteomyelitis, or iatrogenic injury) may be implicated.
Mechanism of Bone Erosion
Cholesteatoma erodes the otic capsule through two distinct mechanisms:
┌─────────────────────────────────────────────────────────┐
│ MECHANISMS OF LABYRINTHINE FISTULA FORMATION │
├────────────────────────────┬────────────────────────────┤
│ ENZYMATIC / MEDIATOR │ PRESSURE / MECHANICAL │
│ MECHANISM │ MECHANISM │
│ │ │
│ Cholesteatoma matrix │ Expanding cholesteatoma │
│ releases: │ sac exerts direct │
│ • Collagenases │ mechanical pressure on │
│ • Prostaglandins (PGE2) │ the otic capsule │
│ • Interleukins (IL-1, IL-6│ │
│ • TNF-α │ Pressure → ischemic │
│ • Matrix metalloprotein- │ osteonecrosis → │
│ ases (MMPs) │ demineralization │
│ → Osteoclast activation │ │
│ → Bone resorption │ │
└────────────────────────────┴────────────────────────────┘
Pathological sequence:
- Cholesteatoma contacts the otic capsule endochondral bone
- Enzymatic demineralization of the dense endochondral bone begins
- Progressive thinning of bone — visible intraoperatively as a "blue line" parallel to the semicircular canal lumen
- Complete erosion → bare endosteal membrane exposed
- Pressure from cholesteatoma → bulging/movement of endosteum → perilymph/endolymph displacement → vestibular symptoms
- Further erosion may breach the endosteum (perilymphatic fistula stage, Sade classification Type III/IV)
— Cummings Otolaryngology
Why the Lateral Semicircular Canal (LSCC)?
The LSCC is the most prominent bulge into the mastoid cavity at the level of the aditus ad antrum. As cholesteatoma fills the epitympanum and antrum, it first contacts and erodes the LSCC prominence. Additionally, the endochondral bone of the LSCC is the thinnest at its ampullated end.
CLASSIFICATION — SADE CLASSIFICATION OF LABYRINTHINE FISTULA
┌──────────────────────────────────────────────────────────────────┐
│ SADE CLASSIFICATION (1987) │
├─────────┬────────────────────────────────────────────────────────┤
│ Type I │ Erosion of periosteum only; endochondral bone intact │
├─────────┼────────────────────────────────────────────────────────┤
│ Type II │ Erosion of periosteum + endochondral bone; │
│ │ endosteum INTACT (true labyrinthine fistula) │
├─────────┼────────────────────────────────────────────────────────┤
│ Type III│ Endosteal membrane EXPOSED (cholesteatoma matrix │
│ │ rests directly on endosteum) │
├─────────┼────────────────────────────────────────────────────────┤
│ Type IV │ Endosteal membrane BREACHED → perilymph leaks │
│ │ (TRUE perilymphatic fistula; highest risk of SNHL) │
└─────────┴────────────────────────────────────────────────────────┘
Sade Types II–III are "classic" labyrinthine fistulae. Type IV = perilymphatic fistula (distinct entity).
ANATOMY RELEVANT TO LABYRINTHINE FISTULA
The otic capsule consists of:
- Periosteal layer — outer vascular
- Endochondral layer — dense avascular bone; uniquely resistant to remodelling
- Endosteal layer — inner layer lining the perilymphatic space
The lateral semicircular canal projects as a ridge into the medial wall of the mastoid antrum. It is the most vulnerable to cholesteatoma erosion because:
- It is the most prominent and accessible structure in the mastoid
- It lies in the direct path of expanding posterosuperior cholesteatoma
Sites affected (in order of frequency):
- Lateral (horizontal) SCC — 98%
- Superior SCC
- Posterior SCC
- Vestibule
- Cochlea (rarest; most severe hearing consequences)
CLINICAL FEATURES
Symptoms
| Symptom | Description |
|---|---|
| Vertigo | Episodic; triggered by pressure changes, sneezing, nose-blowing, Valsalva, loud sounds (Tullio phenomenon). Present in only ~60% |
| SNHL | Particularly with cochlear fistulae; present in 60–70% |
| Aural fullness | Common |
| Tinnitus | May accompany vertigo |
| Tullio phenomenon | Sound-induced vertigo/nystagmus — pathognomonic but uncommon |
| Chronic otorrhoea | Background feature of cholesteatoma |
| Hearing loss | Mixed (conductive + sensorineural) |
| Often asymptomatic | Fistula detected only at surgery in many cases |
— K.J. Lee's Essential Otolaryngology; Cummings
Signs
| Sign | Details |
|---|---|
| Fistula test (positive) | Hennebert's sign — nystagmus/vertigo on pneumatic compression; positive in only 30–50%; low sensitivity, high specificity |
| Nystagmus | May be spontaneous or pressure-induced |
| Hennebert sign | Fistula of membranous labyrinth without bony erosion (e.g. syphilis) |
| Cholesteatoma signs | Posterosuperior retraction pocket, keratin debris, aural polyp, foul discharge |
| Facial nerve paresis | In ~60% of fistula cases (Manolidis) |
| Rinne/Weber | Mixed hearing loss pattern |
Fistula Test (in detail)
FISTULA TEST TECHNIQUE:
Tragal compression → ↑ EAC pressure → moves TM → ossicles → oval window →
perilymph displacement → if fistula present → displacement of endosteum →
cupula deflection → nystagmus + vertigo
Positive = onset of nystagmus within 10 seconds of pressure application
Sensitivity: 30–50% Specificity: HIGH
False negative: Matrix of cholesteatoma may "plug" the fistula
— Dhingra, Cummings
DIAGNOSIS
1. Clinical Assessment
- Thorough otoscopy with microscope
- Careful examination for cholesteatoma extent
- Fistula test
2. Audiological Assessment
- Pure tone audiogram: mixed hearing loss
- Speech discrimination scores (depressed in cochlear involvement)
- Electrocochleography if cochlear fistula suspected
3. Imaging
HRCT Temporal Bone — Investigation of choice:
- Shows soft tissue density (cholesteatoma) eroding lateral SCC
- Focal bony dehiscence along SCC prominence
- Only 60% of confirmed fistulae visible on preoperative CT — a negative CT does NOT exclude fistula
- Better for identifying extent and adjacent dehiscences (tegmen, facial canal)
MRI Temporal Bone:
- Diffusion-weighted MRI (DW-MRI) — highly sensitive for cholesteatoma (non-echo planar > echo planar)
- Helps differentiate cholesteatoma from granulation tissue
- Useful in planned second-look surgeries to detect residual cholesteatoma
Imaging — Key CT Findings
Figure 1: HRCT Temporal Bone — Labyrinthine Fistula
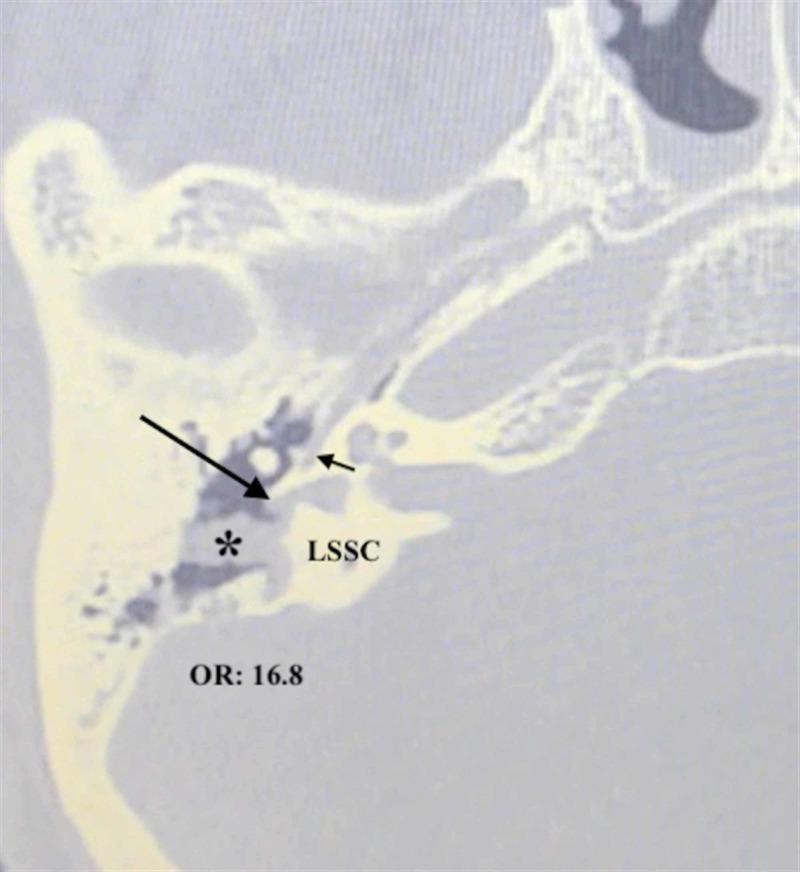
Fig. 1: Axial HRCT showing cholesteatoma (∗) eroding the LSSC causing a labyrinthine fistula (long arrow) with adjacent facial canal dehiscence (short arrow). Note the OR of 16.8 for co-occurrence of these two complications.
Figure 2: Axial HRCT — Bony Dehiscence of LSCC
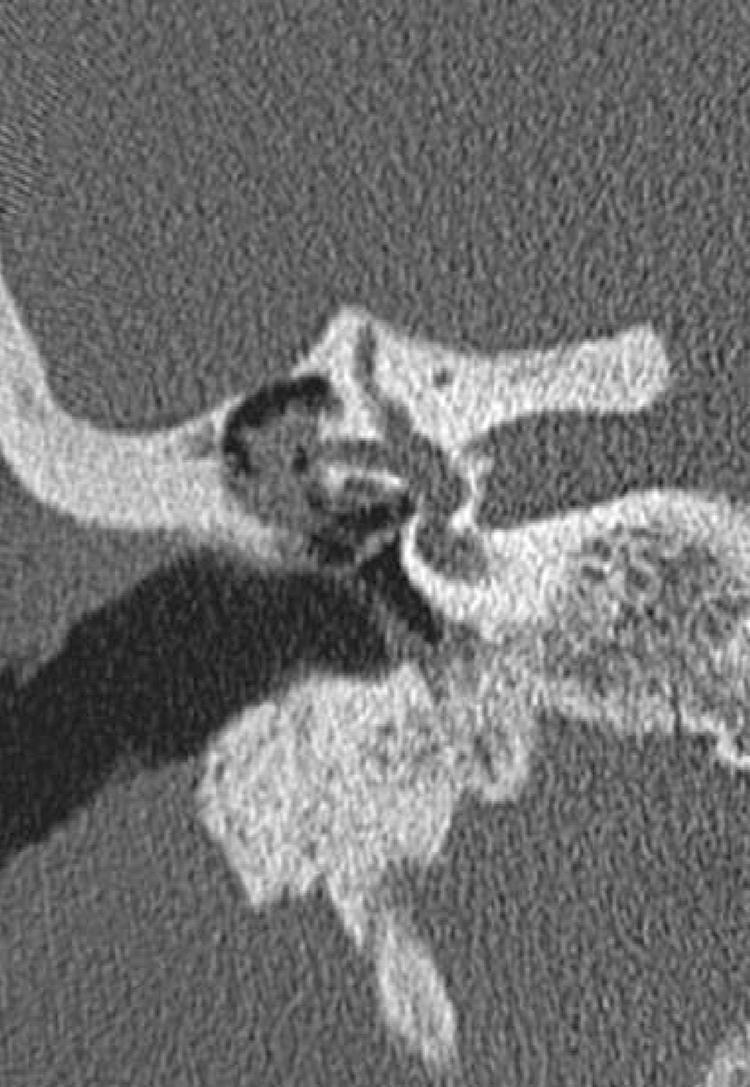
Fig. 2: Axial HRCT temporal bone demonstrating focal bony dehiscence at the LSCC prominence with adjacent soft tissue density consistent with cholesteatoma.
4. Definitive Diagnosis: Surgery
Definitive diagnosis is intraoperative only. Up to 40% of fistulae are detected only at surgery and were not apparent on preoperative CT.
INVESTIGATIONS — SUMMARY FLOWCHART
SUSPECTED LABYRINTHINE FISTULA
(COM with cholesteatoma + vertigo/SNHL/positive fistula test)
│
▼
┌─────────────────────┐
│ HRCT TEMPORAL BONE │ ← First-line imaging
└─────────────────────┘
│ │
CT positive CT negative
(60% cases) (40% cases)
│ │
└────────┬────────┘
▼
┌──────────────┐
│ AUDIOGRAM │ (PTA, speech discrimination)
└──────────────┘
│
▼
┌───────────────┐
│ MRI (DW-MRI) │ ← Characterise cholesteatoma
└───────────────┘
│
▼
┌────────────────────────┐
│ SURGICAL EXPLORATION │ ← Definitive diagnosis
│ (Tympanomastoidectomy) │ AND treatment
└────────────────────────┘
MANAGEMENT
Principles
"The otologic surgeon should ASSUME possible fistula in EVERY cholesteatoma case." — K.J. Lee's Essential Otolaryngology
Management of labyrinthine fistula remains controversial — particularly regarding whether cholesteatoma matrix should be removed from over the fistula or left in place.
Preoperative Preparation
- Baseline audiogram (critical for documenting pre-existing SNHL)
- HRCT temporal bone
- Consent including risk of SNHL, vertigo, dead ear
- Inform patient: fistula management approach may be decided intraoperatively
- Prophylactic IV corticosteroids (high-dose dexamethasone) advocated by some surgeons perioperatively
SURGICAL MANAGEMENT — DECISION ALGORITHM
┌──────────────────────────────────────────────────────────────────────┐
│ SURGICAL MANAGEMENT ALGORITHM │
│ FOR LABYRINTHINE FISTULA │
└──────────────────────────────────────────────────────────────────────┘
│
Tympanomastoidectomy performed
│
┌─────────▼──────────┐
│ Fistula identified │
└─────────┬──────────┘
│
┌───────────────┼──────────────────┐
│ │ │
SMALL FISTULA LARGE FISTULA COCHLEAR FISTULA
(Type II) (Type III) (Any size)
Endosteum Endosteum bare Highest SNHL risk
intact or but intact
nearly so
│ │ │
▼ ▼ ▼
┌──────────────┐ ┌───────────────┐ ┌──────────────┐
│Complete │ │Canal wall DOWN│ │Canal wall │
│removal of │ │Mastoidectomy │ │DOWN │
│matrix + │ │ │ │ │
│fistula repair│ │Leave matrix │ │Leave matrix │
└──────┬───────┘ │over fistula │ │in place over │
│ └───────┬───────┘ │cochlea │
│ │ └──────┬───────┘
▼ ▼ ▼
┌──────────────┐ ┌───────────────┐ ┌──────────────┐
│ If endosteum │ │ Eliminates │ │ Second-look │
│ is TORN → │ │ pressure & │ │ procedure │
│ Revert to │ │ further bone │ │ after 6-12 │
│ CWD + leave │ │ erosion │ │ months │
│ matrix │ └───────────────┘ └──────────────┘
└──────────────┘
— K.J. Lee; Cummings Otolaryngology
SPECIFIC SURGICAL OPTIONS
Option A: Canal Wall Down (Modified Radical/Radical Mastoidectomy) + Leave Matrix
Indications:
- Large fistulae (Sade Type III)
- Cochlear fistulae
- Endosteal membrane exposed or breached
- Revision cases with multiple prior operations
- Preoperative dead ear or severe SNHL
- High-risk cases (only hearing ear)
Advantages:
- Eliminates pressure from cholesteatoma sac → halts further bone erosion
- Lower immediate risk of SNHL
- Better disease control
Disadvantages:
- Leaves living cholesteatoma matrix → recurrence risk
- Requires second-look surgery in 6–12 months
- "Marsupialization" of cholesteatoma
Option B: Complete Removal of Cholesteatoma + Fistula Repair
Indications:
- Small fistulae (Sade Type II)
- Endosteum intact
- NOT recommended for cochlear fistulae
Technique of Fistula Repair:
- Remove cholesteatoma matrix carefully (use "underwater" technique with Ringer's lactate irrigation to keep endosteum moist)
- Avoid suction directly over fistula
- Cover defect with:
- Bone wax (most common)
- Tragal perichondrium
- Temporalis fascia
- Bone pâté
- Fat graft
- Canal wall up or canal wall down decision based on overall extent
Advantages:
- Eliminates cholesteatoma completely
- No second-look needed if complete excision confirmed
- Better long-term disease control
Disadvantages:
- Higher risk of SNHL (particularly if matrix adherent to endosteum)
- True risk of SNHL with manipulation unknown (conflicting evidence)
— K.J. Lee; Cummings
INTRAOPERATIVE IMAGES
Figure 3: Intraoperative Endoscopic View — Labyrinthine Fistula Management
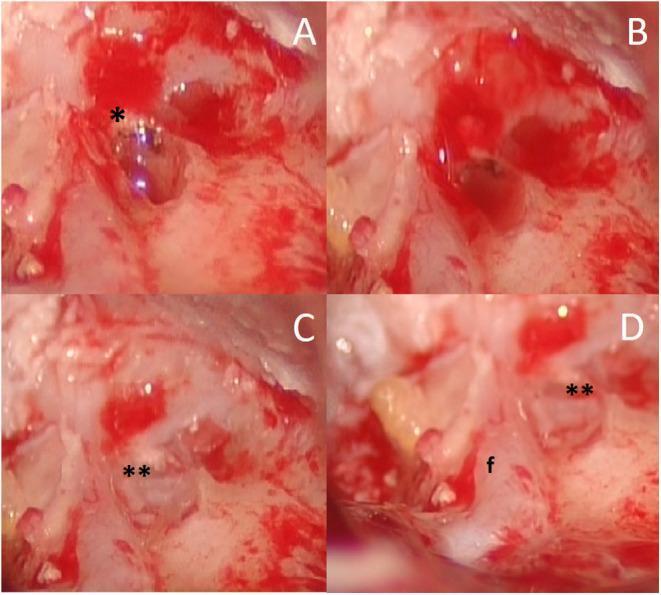
Fig. 3: Intraoperative endoscopic views of labyrinthine fistula repair. (A) Exposed fistula of the lateral and superior SCCs after cholesteatoma matrix removal (∗). (B) Underwater technique — membranous labyrinth submerged in Ringer's solution. (C) Bone wax (∗∗) applied to seal the defect. (D) Final view showing spatial relationship of fistula (∗∗) to the facial nerve (f) positioned inferiorly.
SPECIFIC SURGICAL PRECAUTIONS
CRITICAL INTRAOPERATIVE RULES:
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
1. Never use suction directly over fistula site
2. Keep membranous labyrinth moist at all times
("underwater technique" — Ringer's lactate)
3. Use sharp dissection for matrix removal
4. Always check facial nerve integrity — dehiscence
in ~60% of cases with labyrinthine fistula
5. Check for tegmen dehiscence (~39%)
6. Avoid vigorous irrigation
7. If endosteum tears → STOP matrix removal,
convert to CWD, leave matrix, repair tear
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
— Cummings (Manolidis precautions)
POSTOPERATIVE MANAGEMENT
| Aspect | Details |
|---|---|
| Antibiotics | IV initially, then oral culture-directed therapy |
| Corticosteroids | Perioperative dexamethasone to reduce labyrinthine inflammation |
| Vestibular rehabilitation | In cases with persistent vertigo/imbalance |
| Audiological follow-up | PTA at 6 weeks, 3 months, 1 year |
| Second-look surgery | If matrix left in place, at 6–12 months |
| MRI DWI | Non-echo-planar DWI for residual cholesteatoma detection at 12 months |
COMPLICATIONS
Intraoperative
- Dead ear (sensorineural hearing loss) — risk 5–15% for small fistulae; up to 50% for fistulae penetrating perilymph/endolymph
- Profound vertigo
- Iatrogenic perilymph fistula (endosteal tear)
- Facial nerve injury (given co-existing dehiscence in 60%)
Postoperative
- Residual/recurrent cholesteatoma
- Persistent vertigo
- Progressive SNHL
- Labyrinthitis — spread of infection to inner ear via fistula if endosteum breached
- Meningitis (if labyrinthitis progresses)
— Cummings; K.J. Lee
SPECIAL CONSIDERATIONS
Labyrinthine Fistula as a Risk Factor for Suppurative Labyrinthitis
OTITIS MEDIA WITH CHOLESTEATOMA
│
▼
Labyrinthine Fistula (endosteum exposed)
│
▼
Bacterial entry through fistula
│
▼
Serous Labyrinthitis → Suppurative Labyrinthitis
│
▼
Profound SNHL + Complete Vestibular Loss
│ │
▼ ▼
Labyrinthine Intracranial spread
Ossificans (Meningitis)
— K.J. Lee (Etiology of Labyrinthitis — bacterial entry through labyrinthine fistula or congenital anomaly)
Fistula in Previously Operated Ears
- Average 2.6 prior surgeries in Manolidis series
- Higher incidence of facial nerve dehiscence and tegmen dehiscence
- Greater technical difficulty
- Higher risk of SNHL with matrix removal
PERILYMPHATIC FISTULA vs. LABYRINTHINE FISTULA
| Feature | Labyrinthine Fistula | Perilymphatic Fistula |
|---|---|---|
| Definition | Bony erosion; endosteum intact | Endosteum breached; perilymph leaks |
| Cause | Cholesteatoma (mainly) | Stapes surgery, barotrauma, Valsalva |
| Perilymph loss | No | Yes |
| Fistula test | Positive (30–50%) | Usually positive |
| Treatment | Mastoidectomy ± repair | Remove prosthesis, tissue graft (in stapes surgery context) |
| SNHL risk | Moderate | High |
— Cummings Otolaryngology; the post-stapes perilymph fistula is a separate complication historically more common with Gelfoam patch technique; now rare with small fenestra techniques.
RECENT ADVANCES
1. Non-Echo Planar Diffusion-Weighted MRI (nEP-DWI)
- Superior to CT for detecting small or residual cholesteatoma (sensitivity >90%)
- Allows non-invasive second-look evaluation instead of planned surgical re-exploration
- Reduces need for second surgeries in canal wall up procedures
2. Endoscopic Ear Surgery (EES)
- Improved visualization of medial wall structures
- Single-port endoscopic approach for fistula identification and repair
- Reduces need for extensive canal wall down mastoidectomy in selected cases
- "Underwater" endoscopic technique demonstrated for safe matrix removal over fistula
3. Intraoperative Monitoring
- Continuous intraoperative facial nerve monitoring — mandatory given 60% facial dehiscence rate
- Cochlear nerve monitoring advocated in centers with cochlear fistulae
4. Perioperative Corticosteroids
- High-dose dexamethasone (0.5–1 mg/kg) perioperatively reduces risk of postoperative SNHL in cases where matrix is removed
- Cochrane-level evidence lacking but widely adopted
5. Bone Cement / Hydroxyapatite Repair
- Hydroxyapatite cement for fistula repair provides a more rigid seal and may allow better osteointegration than bone wax alone
6. Cortical Mastoidectomy with Obliteration
- For recurrent or bilateral cholesteatoma with large fistulae, canal wall down with cavity obliteration using abdominal fat reduces cavity maintenance burden
COMPREHENSIVE MANAGEMENT FLOWCHART
CHRONIC OTITIS MEDIA WITH CHOLESTEATOMA
│
▼
Symptoms: Vertigo / SNHL / Aural fullness
Signs: +ve fistula test / Tullio phenomenon
│
▼
┌─────────────────────────────────┐
│ INVESTIGATIONS │
│ • PTA + Speech discrimination │
│ • HRCT Temporal Bone │
│ • DW-MRI (if available) │
│ • Fistula test │
└─────────────┬───────────────────┘
│
▼
CT shows erosion of SCC?
YES (60%) / NO (40% — suspect clinically)
│
▼
┌─────────────────────────────────┐
│ SURGICAL DECISION │
│ TYMPANOMASTOIDECTOMY │
│ (Assume fistula present) │
└─────────────┬───────────────────┘
│
Intraoperative
fistula found?
│ │
YES NO
│ │
▼ ▼
┌──────────────┐ Continue
│Classify size │ standard
│& location │ mastoid
└──────┬───────┘ surgery
│
┌──────▼──────────────────────┐
│ SMALL fistula, endosteum │──► Complete cholesteatoma removal
│ intact (Sade II, LSCC) │ + Fistula repair (bone wax/fascia)
└─────────────────────────────┘ Canal wall UP possible
┌──────────────────────────────┐
│ LARGE fistula, bare │──► Canal wall DOWN
│ endosteum (Sade III) or │ Leave matrix over fistula
│ multiple SCCs involved │ Second-look at 12 months
└──────────────────────────────┘ (DWI-MRI surveillance)
┌──────────────────────────────┐
│ COCHLEAR fistula (any size) │──► Canal wall DOWN ALWAYS
└──────────────────────────────┘ Leave matrix; no matrix removal
Counsel re: SNHL risk
┌──────────────────────────────┐
│ Endosteum TORN intraop │──► STOP matrix removal
│ (perilymph visible) │ Convert to CWD
└──────────────────────────────┘ Pack with fascia
Postop high-dose steroids
│
▼
┌─────────────────────────────────┐
│ POSTOPERATIVE CARE │
│ • IV → oral antibiotics │
│ • Perioperative dexamethasone │
│ • Audiogram at 6w, 3m, 1yr │
│ • Vestibular rehab if needed │
│ • DWI-MRI / second-look at 12m │
└─────────────────────────────────┘
SUMMARY TABLE
| Aspect | Key Points |
|---|---|
| Definition | Erosion of endochondral bone of otic capsule without perilymph loss |
| Most common cause | Cholesteatoma (>95%) |
| Incidence | 7–10% of cholesteatoma cases |
| Most common site | Lateral (horizontal) SCC (~98%) |
| Pathogenesis | Enzymatic (MMP, collagenase, cytokines) + pressure mechanisms |
| Key symptom | Vertigo (60%); SNHL (60–70%) |
| Key sign | Positive fistula test (30–50%); Tullio phenomenon |
| Diagnosis | HRCT (60% sensitivity); definitive = intraoperative |
| Classification | Sade I–IV |
| Management | Tympanomastoidectomy; matrix removal vs. leaving matrix (controversial) |
| Cochlear fistula | CWD always; leave matrix; highest SNHL risk |
| Facial nerve | Dehiscent in ~60% of labyrinthine fistula cases |
| Recent advances | nEP-DWI, endoscopic ear surgery, perioperative steroids, HA cement repair |
REFERENCES
- Cummings Otolaryngology Head and Neck Surgery (7th Edition) — Chapter 141 (Complications of Otitis Media); Chapter on Stapes Surgery complications
- K.J. Lee's Essential Otolaryngology (11th Edition) — Labyrinthine Fistula; Labyrinthitis
- Manolidis S. — Review of 111 patients with labyrinthine fistulae, Am J Otolaryngol 24:51–60, 2003
- Gersdorff M et al. — Labyrinthine fistula after closed tympanoplasty for cholesteatoma (large series)
- Sade J — Classification of labyrinthine fistulae (1987)
- Soda-Merhy A — Surgical treatment of labyrinthine fistula caused by cholesteatoma (2015)
- Dhingra PL — Diseases of Ear, Nose and Throat (7th ed) — Fistula test; complications of CSOM
- Hazarika P — Textbook of Ear Nose Throat & Head Neck Surgery
- Stell & Maran's Otolaryngology — Complications of chronic suppurative otitis media
- Scott Brown's Otorhinolaryngology, Head and Neck Surgery (8th ed) — Cholesteatoma complications; labyrinthine fistula
Note on image generation: Detailed flowcharts and anatomical diagrams have been provided in text format above. Custom diagram generation is currently unavailable (monthly limit reached). Please contact support or upgrade your plan for image generation. The clinical CT and intraoperative photographs above (Figs. 1–3) are sourced from peer-reviewed medical literature and illustrate all key radiological and surgical findings.
This is a shared conversation. Sign in to Orris to start your own chat.