How to learn everything ndt in pediatrics practically in detail
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Now I have enough from the textbooks plus comprehensive knowledge to give you a thorough, practical guide. Let me compile this.
How to Learn NDT (Neurodevelopmental Therapy / Bobath Technique) in Pediatrics — Practically & In Detail
NDT/Bobath is a hands-on clinical framework used primarily for children with cerebral palsy (CP), acquired brain injury, and other conditions affecting postural control and movement. Here is a structured, practical roadmap.
1. Understand What NDT Actually Is
NDT is not a rigid protocol — it is a problem-solving approach. The core philosophy:
- Facilitate normal movement while inhibiting abnormal tone and reflex activity using specific motor patterns
- Restore postural control as the foundation for all movement
- Coordinate patterns of muscle group activity (synergies) rather than isolating individual muscles
- Bobath therapists avoid provoking mass flexor synergies (shoulder–elbow–wrist flexion) or extensor synergies (knee–ankle extension) — these are pathological movement patterns that must be inhibited
- Therapy progresses in a neurodevelopmental sequence — mimicking normal infant motor development: rolling → prone on elbows → quadruped → sitting → standing → walking
(Bradley and Daroff's Neurology in Clinical Practice, p. 1166–1167)
2. Master the Foundational Knowledge First
Before touching a child, build this knowledge base:
A. Normal Neurodevelopment
- Milestone progression: head control (2–3 months) → rolling (4–5 m) → sitting (6–7 m) → crawling (8–9 m) → standing/cruising (9–12 m) → walking (12–15 m)
- Primitive reflex integration (ATNR, STNR, Moro, rooting) — NDT heavily uses reflex knowledge
- Postural reactions: righting reactions, equilibrium reactions, protective extension — these are the targets of NDT facilitation
- Normal tone, muscle activation patterns, biomechanics of pediatric gait
B. Pathological Conditions Where NDT Is Applied
| Condition | Key NDT Target |
|---|---|
| Spastic CP (hemiplegia, diplegia, quadriplegia) | Reduce spasticity, facilitate selective movement |
| Dyskinetic / athetoid CP | Improve postural stability, reduce involuntary movement |
| Hypotonic conditions (Down syndrome, etc.) | Increase co-contraction, stability |
| Acquired brain injury (TBI, stroke) | Re-establish postural control, inhibit synergies |
| Developmental coordination disorder | Motor learning, task-specific practice |
C. Key Neurophysiology Concepts
- Upper motor neuron (UMN) lesion effects: spasticity, exaggerated reflexes, loss of selective motor control
- Neuroplasticity — the biological basis for why NDT works: repetitive practice drives cortical reorganization and neurotrophic factor expression
- Sensory-motor integration: proprioception, vestibular input, and tactile input all influence tone and motor output — NDT uses all three
3. The Practical NDT Clinical Framework
Step 1 — Assessment (Before Any Handling)
Observe the child before touching:
- Resting posture: Where is the child's center of mass? Asymmetries? Head position?
- Tone at rest: Hypertonic (spastic/rigid), hypotonic, or fluctuating (dyskinetic)?
- Active movement: Can the child initiate movement? From where? Against gravity?
- Functional activities: Reaching, grasping, sitting, transferring weight
- Postural reactions: Does the child show equilibrium reactions? Protective extension?
- Primitive reflexes: Are they still present and interfering (e.g., ATNR locking the arm with head turn)?
Step 2 — Identify Key Problems (NDT Problem-Solving)
Ask:
- What is the primary impairment limiting function? (e.g., hip flexor spasticity preventing weight shift)
- What compensatory strategy is the child using? (e.g., trunk lateral flexion to clear the leg during gait)
- What is the functional goal? (e.g., walking independently, reaching overhead, self-feeding)
Step 3 — Handling and Key Points of Control (KPCs)
NDT is built on handling — where and how you place your hands determines what movement you facilitate or inhibit.
Key Points of Control (KPCs) are body parts through which the therapist influences movement. They include:
- Proximal KPCs: pelvis, shoulder girdle, head — most powerful for changing whole-body tone
- Distal KPCs: hands, feet — used for fine-tuning and selective movement
Practical examples:
- To facilitate trunk extension in a hypotonic infant: support at the pelvis (posterior-to-anterior pressure) + facilitate neck extension
- To inhibit lower limb extensor spasticity in a child with CP: flex and externally rotate the hip + dorsiflex the ankle before weight-bearing
- To prepare spastic upper limb for reach: elongate the side (weight-bearing through that arm in side-sitting), externally rotate the shoulder, extend the elbow
Step 4 — Movement Preparation ("Preparation Before Activity")
NDT always prepares the body before asking it to perform a function:
- Tone normalization: inhibit high tone through slow elongation, rhythmic rotation, weight-bearing through the limb
- Align the body: neutral pelvis, head over trunk, shoulder girdle over pelvis
- Activate target muscles: use facilitation tapping, weight-shifting, approximation (compression) to activate postural muscles
- Then introduce function: now ask the child to reach, transfer weight, or step — the movement should be easier and more normal
Step 5 — Facilitation Techniques (Core Skills)
| Technique | How | Purpose |
|---|---|---|
| Rhythmic rotation | Slowly rotate a limb or trunk in patterns | Reduce spasticity, normalize tone |
| Weight-bearing through limb | Press through the axis of the limb (approximation) | Activate co-contraction, normalize tone, stimulate proprioception |
| Weight-shifting | Gently shift child's CoM laterally or anteriorly | Elicit equilibrium and righting reactions |
| Slow elongation | Stretch a hypertonic muscle group in a sustained, slow fashion | Tone inhibition |
| Tapping | Quick mechanical tap to a hypotonic muscle | Facilitate activation in a weak/hypotonic muscle |
| Facilitation of righting reactions | Tilt body to elicit head-righting | Re-train automatic postural reactions |
| Compression/approximation | Press joint surfaces together along joint axis | Increase stability awareness, proprioceptive input |
| Inhibitory positioning | Position child to reduce tone (e.g., hip/knee/ankle flexion for extensor spasticity) | Baseline tone management |
4. Developmental Activity Sequence (The NDT Mat Program)
This progression mirrors normal motor development and is used for children with CP and brain injury:
- Supine — head control, rolling prep, hand-to-mouth, visual tracking
- Rolling — from supine to side-lying using trunk rotation (not mass flexion or extension)
- Side-lying — weight-bearing on one side, facilitating lateral trunk elongation
- Prone on elbows — neck/upper trunk extension against gravity, weight-shifting through forearms
- Quadruped (all-fours) — hip/knee/trunk stability, reciprocal limb movements
- Sitting — postural control in sitting, weight-shifting for reaching, protective extension
- Transitions — sit-to-stand, floor-to-stand (most functionally important)
- Standing — pelvic alignment, knee control, weight-shifting for gait
- Gait — step initiation, swing-phase clearance, heel-strike, dissociated arm swing
(Bradley and Daroff's Neurology in Clinical Practice, p. 2030)
5. Integration With Other Therapies
Modern NDT does not exist in isolation. The Harriet Lane Handbook (pediatric standard) emphasizes an interdisciplinary team:
- PT (Physical Therapy) — gross motor, gait, postural control (primary NDT domain)
- OT (Occupational Therapy) — fine motor, self-care, upper limb function
- SLP (Speech-Language Pathology) — feeding, communication, oral-motor tone
- Educators and school system — generalization of skills to real environments
- Community/parent advocacy — home program training for caregivers
Parents and caregivers must be taught NDT handling principles — the child spends 1 hour in therapy and 23 hours at home. Carryover is everything.
6. Complementary Approaches to Learn Alongside NDT
Modern evidence has shifted toward combining NDT with these techniques:
| Approach | Key Use in Pediatric Rehab |
|---|---|
| Constraint-Induced Movement Therapy (CIMT) | Hemiplegic CP — constraining unaffected limb to force use of affected arm |
| Task-Oriented Practice | Massed practice of real-world tasks; drives neuroplasticity more directly than passive facilitation |
| Treadmill training (with/without body weight support) | Gait re-education in CP and brain injury |
| Hippotherapy / pool therapy | Proprioceptive and vestibular input, tone normalization |
| Sensory Integration (Ayres) | Children with sensory processing differences affecting tone and attention |
| Kinesio Taping | Facilitate weak muscles or inhibit spastic muscles as adjunct to NDT |
| Orthotics (AFO, SMO) | Maintain alignment achieved in NDT sessions; prevent contracture |
| Botulinum toxin (Botox) + NDT | Toxin reduces spasticity window → NDT maximizes the functional gain in that window |
7. How to Learn Practically — Step-by-Step Pathway
Phase 1: Observe (Months 1–3)
- Observe experienced NDT-trained therapists with children of different CP types and ages
- Watch every handling transition — where are the hands? What changes in the child?
- Practice identifying tone (hyper vs. hypo), asymmetry, compensatory patterns before any handling
Phase 2: Hands-On Foundations (Months 3–6)
- Practice tone assessment — learn to grade spasticity (Modified Ashworth Scale) and identify ATNR/STNR in real children
- Practice rhythmic rotation and weight-bearing on willing volunteer children or adult models first
- Learn the 5 classic KPCs and practice facilitation of each postural reaction in a controlled setting
Phase 3: Clinical Practice (Months 6–18)
- Treat under supervision — have an NDT mentor observe your handling and give direct feedback
- Video record your sessions (with consent) — reviewing footage reveals hand placement errors you cannot feel in the moment
- Practice across CP subtypes: spastic hemiplegia, spastic diplegia, hypotonia (different NDT approach for each)
- Learn to write functionally-framed goals (e.g., "Child will independently transition from floor-sit to standing using bilateral upper extremity support within 6 months")
Phase 4: Formal Certification
- NDTA (Neurodevelopmental Treatment Association) — the international certifying body
- Basic NDT Course: 8-day intensive course with hands-on labs; prerequisite is a clinical degree (PT, OT, SLP)
- Advanced/Specialty Courses: pediatric focus, CP-specific, upper limb, feeding
- NDTA certification exam follows after completing required coursework and clinical hours
Phase 5: Evidence-Based Refinement
- Critically read the NDT literature — the evidence base is mixed (some RCTs show equivalence, not superiority, over other approaches)
- Integrate motor learning principles: repetition, variability of practice, task specificity, feedback timing are now known to drive neuroplasticity more powerfully than passive facilitation alone
- Stay current with NDTA, Academy of Pediatric Physical Therapy (APPT), and CanChild publications
8. Key Assessment Tools to Master Alongside NDT
| Tool | What It Measures |
|---|---|
| GMFCS (Gross Motor Function Classification System) | Functional level of CP (I–V) — guides prognosis and goal setting |
| GMFM-66/88 (Gross Motor Function Measure) | Quantitative measure of gross motor ability; tracks NDT outcomes |
| Modified Ashworth Scale | Spasticity grading in each muscle group |
| Pediatric Balance Scale | Functional balance in school-age children |
| QUEST (Quality of Upper Extremity Skills Test) | Upper limb quality of movement in CP |
| PEDI (Pediatric Evaluation of Disability Inventory) | Functional skills and caregiver assistance in self-care, mobility, social |
| Tardieu Scale | More sensitive spasticity measure than Ashworth; distinguishes spasticity from contracture |
Summary Practical Checklist
- Understand normal neurodevelopment milestones and postural reactions cold
- Know primitive reflexes, when they integrate, and how they interfere when retained
- Learn to clinically classify CP (type, distribution, GMFCS level)
- Master tone assessment (Ashworth, Tardieu)
- Learn the 5 proximal and distal KPCs and their effects
- Practice rhythmic rotation and weight-bearing before any other technique
- Work through the developmental activity sequence on a mat with supervised patients
- Train parents/caregivers — carryover is the multiplier
- Enroll in NDTA-certified basic course when clinically ready
- Pair NDT with task-oriented practice and CIMT where evidence supports it
Key sources used:
- Bradley and Daroff's Neurology in Clinical Practice, pp. 1166–1168 (Physical therapy techniques, Bobath/NDT, motor learning)
- The Harriet Lane Handbook, 23rd ed. (Pediatric interdisciplinary rehabilitation team structure)
All demonstrations in detail
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
NDT Bobath handling techniques cerebral palsy pediatric therapy
Searching Images
pediatric physical therapy developmental sequence mat activities sitting standing gait
Loading Image
Loading Image
Loading Image
Excellent — I have strong clinical images and comprehensive textbook content. Here is the full detailed demonstrations guide.
NDT (Neurodevelopmental Therapy / Bobath) — Complete Demonstration Guide for Pediatrics
PART 1: TONE ASSESSMENT BEFORE ANY HANDLING
Before every session, assess tone. Your entire treatment plan depends on it.
How to Assess Spasticity (Modified Ashworth Scale)
Demonstration — Upper limb (elbow flexors):
- Child supine, relaxed
- Support the child's upper arm with one hand at the humerus
- With your other hand, hold the forearm and passively extend the elbow from full flexion to full extension in 1 second (fast)
- Feel for the "catch" — the point where resistance is felt
- Grade:
- 0 = No increase in tone
- 1 = Slight catch then release
- 1+ = Catch then minimal resistance through less than half the range
- 2 = Marked increase but limb moves easily
- 3 = Considerable increase; passive movement difficult
- 4 = Limb rigid in flexion or extension
Demonstration — Lower limb (hamstrings, hip adductors in CP):
- For hamstrings: child supine → lift the leg from hip (keep knee extended) → measure popliteal angle at resistance
- For hip adductors: child supine → abduct both hips symmetrically → note angle of resistance and asymmetry (key for spastic diplegia)
- For plantarflexors: dorsiflex the foot quickly → feel for equinus "catch" (very common in CP)
Tardieu Scale (more specific):
- Perform movement at two speeds: V1 (very slow) and V3 (fast as possible)
- R2 = angle of arrest at slow speed (true contracture)
- R1 = angle of catch at fast speed (spasticity)
- Spasticity angle = R2 − R1 — greater than 10° confirms dynamic spasticity (treatable) vs. fixed contracture
PART 2: PRIMITIVE REFLEX TESTING (Must Know Before Handling)
These reflexes, if retained, block normal movement and dictate your NDT handling strategy.
1. Asymmetric Tonic Neck Reflex (ATNR)
Demo:
- Child supine, head midline, limbs relaxed
- Slowly rotate head to one side (45–90°) and hold 5 seconds
- Positive: Arm and leg on the face side extend; arm and leg on skull side flex ("fencer position")
- Should integrate by: 4–6 months
- NDT impact: Keep head midline during all activities; ATNR will lock the arm in extension when head turns — avoid head rotation during reaching tasks
2. Symmetric Tonic Neck Reflex (STNR)
Demo:
- Child in quadruped (all-fours) or draped over your knee prone
- Flex the neck (chin to chest): arms flex, hips extend
- Extend the neck (lift head): arms extend, hips flex
- Should integrate by: 6–8 months
- NDT impact: In children with retained STNR, crawling is impossible in the normal pattern — must inhibit before training quadruped
3. Tonic Labyrinthine Reflex (TLR)
Demo:
- Supine position: Increases extensor tone throughout body (back arches, neck extends, legs extend)
- Prone position: Increases flexor tone throughout body (flexion posture)
- Should integrate by: 3–4 months
- NDT impact: Supine work increases extensor spasticity — must counteract this; prone work is used deliberately to increase flexor activation in hypotonic children
4. Moro Reflex
Demo:
- Child semi-supine, supported in your arms
- Slightly drop the head (2 cm drop) or make a sudden loud sound
- Positive: Arms abduct and extend symmetrically, then flex and adduct ("embrace")
- Should integrate by: 4–5 months
- NDT impact: Retained Moro = child startles easily, disrupts postural stability; must control head support and avoid sudden movements during sessions
5. Galant Reflex (Spinal Incurvature)
Demo:
- Child in prone suspension (held horizontally by abdomen)
- Stroke firmly down one side of the spine (paravertebral, not on spine itself)
- Positive: Trunk curves toward the stroked side (hip hiking)
- Should integrate by: 3–5 months
- NDT impact: If retained, sitting is unstable because any pressure on one side curves the trunk; affects sitting in children with CP
PART 3: POSTURAL REACTION TESTING (NDT Treatment Targets)
These are the reactions NDT aims to facilitate. Always test first to know your baseline.
1. Head Righting Reactions
Demo:
- Hold child in vertical suspension (hands around trunk)
- Tilt the body laterally 30° to the right
- Normal: Head immediately rights itself to vertical (eyes horizontal, mouth horizontal)
- Purpose in NDT: If absent, facilitate it — tilt the child slowly and wait for them to initiate the head righting; do not do it for them
2. Lateral Righting (Sideways Equilibrium)
Demo — Sitting on therapy ball:
- Child seated on therapy ball, feet off floor
- Slowly roll the ball to one side
- Normal: Child's trunk elongates on the lowered side and weight shifts — the opposite side shows lateral trunk flexion toward midline + protective arm extension downward
- Grading: Does the head right? Does the trunk react? Is protective extension present?
3. Protective Extension (Parachute Reaction)
Demo — Forward:
- Hold child vertically in your arms, facing down
- Quickly lower them toward the mat as if falling forward
- Normal: Arms extend symmetrically to "catch" the fall by 6–7 months
- Lateral protective extension: Seat child, rapidly push them to one side → arms should extend laterally to the same side
- NDT use: If absent, facilitate by gently pushing the child off-balance in sitting and waiting; placing hands at the shoulders (not catching them) so they must generate the response
4. Equilibrium Reactions (Dynamic Balance)
Demo — On therapy ball or tilt board:
- Seat child on therapy ball with feet grounded
- Slowly shift the ball laterally, anteriorly, or posteriorly
- Normal: Trunk bends away from the tilt, center of mass is maintained over base of support, limbs adjust
- Absent: Child falls rigidly with no trunk adjustment
PART 4: KEY POINTS OF CONTROL (KPCs) — HANDLING DEMONSTRATIONS
KPCs are the specific body points through which the therapist's hands direct movement. This is the core of NDT handling.
Proximal KPCs
1. Pelvis (Most Powerful KPC)
Why: Pelvic position controls the entire trunk, hips, and lower limbs. Anterior pelvic tilt = lumbar lordosis + hip flexor shortening. Posterior tilt = trunk collapse + reduced hip extension for gait.
Demonstration — Pelvic facilitation in sitting:
- Sit behind the child on a plinth or therapy ball
- Place both thumbs on the posterior iliac crests, fingers wrapping around the iliac crests anteriorly
- Anterior tilt facilitation: Gently press thumbs downward and forward (imagine rocking the pelvis so the "bowl" tips forward) — activates lumbar extensors and hip extensors
- Posterior tilt facilitation: Hands guide pelvis backward and under — reduces lordosis
- Weight-shift right: Right thumb presses the right iliac crest downward, left hand lifts slightly — child's weight shifts right, eliciting left trunk elongation
- Practice: Without the child — practice on yourself in a chair, feel how pelvic position changes your entire trunk posture
2. Shoulder Girdle
Why: Controls upper trunk extension, arm function, and breathing. Protracted (rounded) shoulders are common in spastic quadriplegia and hypotonia.
Demonstration:
- Stand or kneel behind the child
- Place hands over both shoulder girdles (fingers on anterior chest, thumbs on scapulae)
- Facilitate scapular retraction: Gently draw shoulders back and down (retract + depress scapulae)
- Observe: Head lifts, thoracic extension occurs, arm function improves
- Caution: Never force — this is a gentle approximation, not a stretch
3. Head and Neck
Demonstration — Head control facilitation in supine:
- Child supine on mat
- Sit at the head end, cup both hands under the occiput (cradle hold)
- Gently flex the neck (chin tuck) — this inhibits extensor spasticity (TLR-supine)
- Hold 10–15 seconds, then slowly bring head to neutral
- Then tilt head to one side and wait for lateral neck righting to initiate
Distal KPCs
4. Hands / Wrists
Demonstration — Upper limb tone inhibition for spastic hemiplegic child:
- Hold the child's affected hand, fingers in your palm
- Slowly extend the wrist and fingers (against flexor spasticity) — use slow, sustained pressure, not force
- Simultaneously supinate the forearm (palm up)
- With your other hand, externally rotate the shoulder gently
- Hold the inhibitory position 10–20 seconds — feel the tone gradually decrease (this is "reflex inhibiting pattern" or RIP for the upper limb)
- Now the arm is prepared for weight-bearing or reaching activity
5. Feet / Ankles
Demonstration — Lower limb tone inhibition (equinus, extensor spasticity):
- Child supine
- Hold the heel firmly in your palm (heel cup)
- Slowly dorsiflex the ankle — slow and sustained to inhibit the gastrocnemius/soleus spasticity
- Simultaneously flex and externally rotate the hip
- Flex the knee to 90°
- This combined position (hip flexed + ER + knee flexed + ankle dorsiflexed) is the reflex-inhibiting pattern for lower limb extensor spasticity
- Hold 15–20 seconds before any weight-bearing activity
PART 5: DEVELOPMENTAL SEQUENCE MAT ACTIVITIES — FULL DEMONSTRATIONS
🔵 POSITION 1: SUPINE (Lying on Back)
Problem in CP/brain injury: Extensor spasticity from TLR-supine, ATNR locking the arms
NDT Demonstration:
- Child supine on mat
- Inhibit extensor tone first: Flex both hips and knees (bring knees to chest), then add hip external rotation — rock gently side-to-side ("log roll" preparation)
- Maintain head midline to neutralize ATNR
- Facilitate head lifting: Place hands under occiput, give slight flexion cue — child initiates chin tuck and lifts head
- Midline hand activity: Bring child's hands to chest midline, facilitate hand-to-hand and hand-to-mouth
- Facilitate rolling preparation: Flex one hip and knee across midline → this initiates trunk rotation → prepares rolling
🔵 POSITION 2: ROLLING (Supine → Side-Lying → Prone)
Normal pattern: Head leads, shoulder girdle follows, pelvis follows — using trunk rotation (not mass movement)
NDT Demonstration — Rolling to right:
- Child supine, head midline
- KPC: Shoulder girdle — place hands on left shoulder girdle
- Gently bring left shoulder across midline toward the right → this initiates segmental trunk rotation
- Do NOT pull the whole body as one unit (that is mass movement — abnormal pattern)
- Wait for the child to respond — do not roll them passively
- As the shoulder comes over, the pelvis follows — facilitate at pelvis if needed
- Alternative KPC: Pelvis — hold the left hip/pelvis and bring it over — pelvis leads, shoulder follows
- The child arrives in side-lying — key intermediate position
Side-lying pause:
- This is excellent for children with strong extensor or flexor spasticity — side-lying is a "neutral" tone position
- Facilitate trunk elongation on the lower side by lifting the upper trunk slightly
- Weight-bearing through the lower shoulder/arm → proprioceptive input
🔵 POSITION 3: PRONE ON ELBOWS
Goal: Neck and upper trunk extension against gravity, upper extremity weight-bearing, scapular stability
NDT Demonstration:
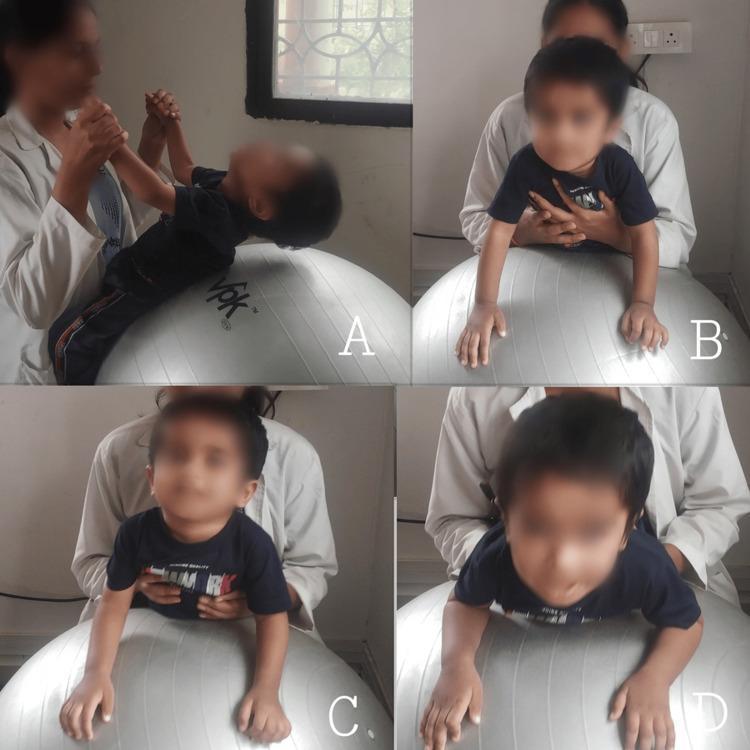
Above: Panel A — supine traction on physioball to prepare shoulder/neck extensors. Panel B — prone on elbows on ball with chest support. Panel C — prone on hands (progressed). Panel D — head extension with scapular retraction.
On the mat:
- Child prone, elbows under shoulders (90° elbow flexion), forearms flat
- Therapist kneels at child's side — one hand on sternum (support), one on pelvis
- Facilitate head lifting: Gentle pressure on thorax from behind + verbal/visual cue → child lifts head against gravity
- Facilitate weight shift through arms: Gently rock child's weight forward onto forearms (approximation/compression through elbows) — activates shoulder girdle stabilizers
- Progress: Place toy slightly lateral to child → they reach with one arm → single-arm weight-bearing (builds to quadruped)
On a physioball (as shown in image):
- Drape child prone over the ball (chest on ball, hands hanging)
- Slowly lower ball toward floor → child extends neck to lift head (neck righting)
- Slowly tilt ball side to side → elicits trunk righting reactions in prone
🔵 POSITION 4: QUADRUPED (All-Fours / Crawling Position)
Goal: Hip/knee stability, trunk co-contraction, reciprocal limb movement (pre-gait pattern)
NDT Demonstration:
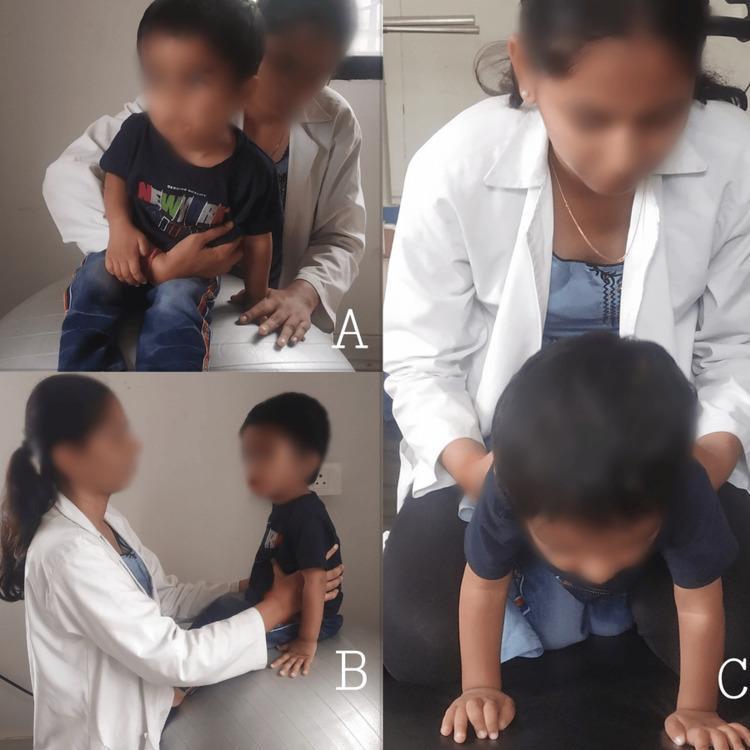
Above: Panel C shows therapist facilitating quadruped position on the mat — hands at trunk guiding rocking and reaching movements.
Step-by-step:
- Getting into quadruped: From side-lying, guide the upper arm to push up, then flex both knees — avoid letting child "log roll" into quadruped
- Establish stable quadruped:
- Hips directly over knees (90° hip flexion)
- Shoulders directly over hands
- Spine neutral (not collapsed into kyphosis or hyperlordosis)
- KPC: Pelvis — hands on iliac crests, give gentle anterior-posterior oscillations → activates lumbar extensors and abdominals simultaneously (co-contraction)
- Joint approximation/compression through limbs:
- Press gently down through shoulder joints (through the arm into the mat) → activates rotator cuff and scapular stabilizers
- Press gently down through the hips → activates gluteals and hip stabilizers
- Weight shifting — prerequisite for crawling:
- Shift weight to left arm + left knee → right arm and knee are freed to advance
- Progress to: child reaches forward with one hand → this forces weight onto the other 3 limbs (diagonal pattern)
- Facilitate reciprocal crawling:
- KPC pelvis — guide the pelvis in the reciprocal rotation pattern (right hip forward with left arm forward)
- Begin with assisted pattern, reduce assistance gradually
Note on STNR and crawling: If child's arms collapse when they flex neck → retained STNR is interfering → first work on STNR inhibition (head midline, small neck movement range) before full crawling training
🔵 POSITION 5: SITTING
This is the most clinically important position for daily function.
Above: Panel A — therapist behind child seated, bilateral pelvic/trunk facilitation. Panel B — seated on therapy ball with lateral support for dynamic equilibrium training.
A. Establishing Stable Sitting
- Child seated on plinth, feet flat on floor (or on a step if feet don't reach)
- KPC: Pelvis — sit behind child, thumbs on posterior iliac crests
- Guide pelvis to anterior tilt (neutral to slight anterior) — this is the foundation
- Check alignment: Trunk upright, head over pelvis, shoulders level
- Arms free at sides — resist the urge to support the arms (they need to be free for equilibrium responses and protective extension)
B. Weight-Shifting in Sitting (Equilibrium Facilitation)
- From behind, hands on pelvis (iliac crests)
- Slowly shift child's weight to the right:
- Right side: right side of trunk shortens (compresses)
- Left side: left trunk elongates (stretches)
- Observe: Does the head right to vertical? Does left arm extend laterally (protective extension)?
- Shift forward: Tilt pelvis anteriorly and shift CoM forward — activates ankle dorsiflexors, gluteals, trunk extensors
- Shift backward: Gently push sternum backward → child must activate abdominals to recover → starts with hands on belly to feel activation
C. Sitting on Therapy Ball (Dynamic)
- The unstable surface automatically challenges equilibrium reactions continuously
- Start with slow, small-amplitude tilts; progress to larger tilts as control improves
- Therapist controls the ball, not the child's body — the child must respond to the ball's movement
D. Reach from Sitting (Functional Integration)
- Present a toy slightly outside the child's reach (lateral, forward, overhead)
- Do not hand it to them — they must weight-shift to reach
- Therapist guides at pelvis only — the child generates the movement
- Graded: within base of support → at edge of BOS → outside BOS (most challenging)
🔵 POSITION 6: TRANSITIONS — SIT TO STAND
This is the most functional transition — critical for independence.
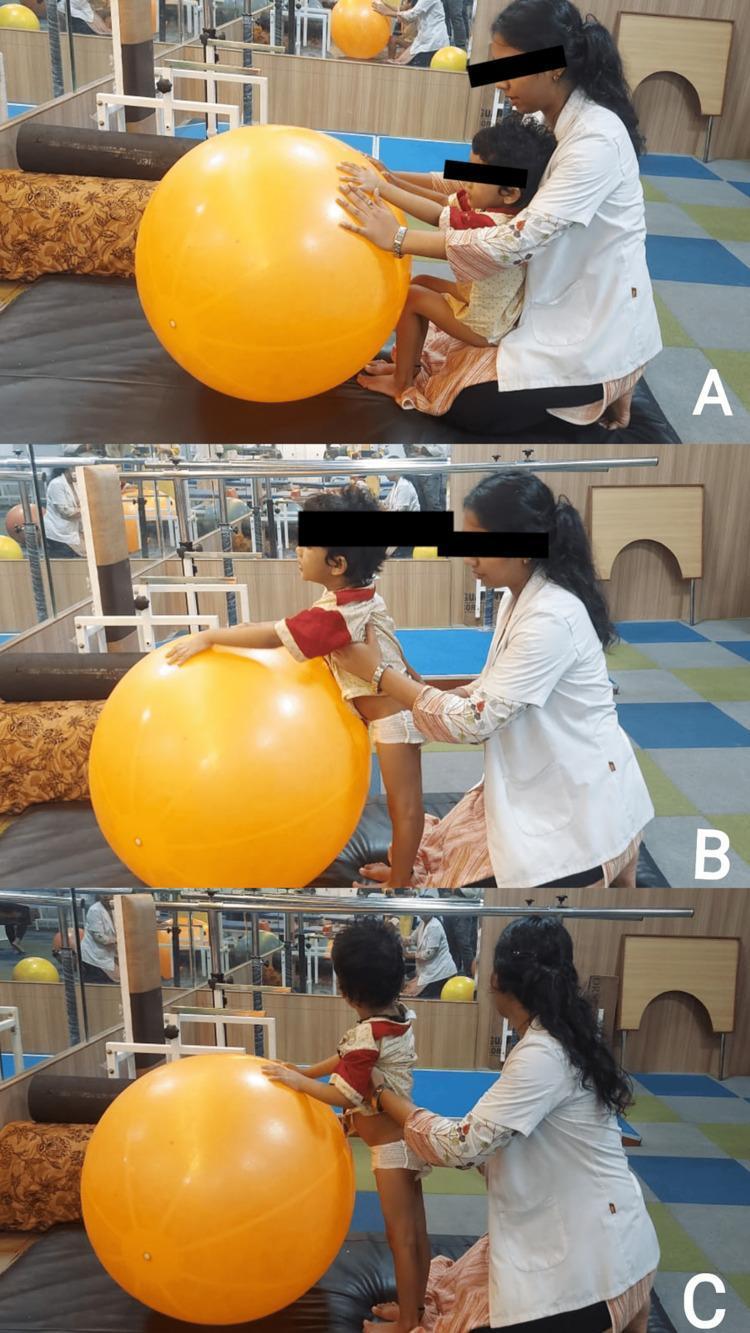
Above: A — seated position with hands on ball for UE support. B — transition phase, therapist guides at trunk and hips. C — full standing achieved with therapist support at lower trunk.
Preparation (NDT tone inhibition first):
- Inhibit plantarflexor spasticity (heel cups → dorsiflexion + hip flexion → hold 15 seconds)
- Ensure pelvis is in anterior tilt in sitting (neutral pelvis cannot extend into standing efficiently)
- Feet hip-width apart, flat on floor
Step-by-step demonstration:
- KPC: Pelvis from behind — hands on iliac crests
- Phase 1 — "Nose over toes": Guide pelvis and trunk forward so child's trunk leans over their feet (center of mass shifts forward) — this is the most common failure point in CP
- Phase 2 — Rise: As CoM passes over the feet, guide the pelvis upward and forward — activate hip extensors and knee extensors
- Phase 3 — Full standing: Guide pelvis to neutral in standing — avoid anterior pelvic tilt (common compensatory pattern)
- Common errors to correct:
- Child extends neck backward to initiate the rise (using neck extensors as a substitution) → block this by keeping head in neutral
- Child pushes through the arms rather than loading the legs → remove arm support progressively
- Child's heels lift (equinus) → return, inhibit plantarflexors, then retry
Graded assistance:
- Full: therapist guides entire movement at pelvis
- Moderate: therapist at pelvis, child initiates
- Minimal: therapist hands at ready, child performs independently
- Independent: child performs; therapist observes for quality
🔵 POSITION 7: STANDING — WEIGHT-SHIFTING AND BALANCE
Goal: Symmetric weight-bearing, pelvic control, step initiation
NDT Demonstration:
-
Establish stance:
- Feet hip-width, toes forward (externally rotated feet → "fix" at pelvis first)
- KPC: Pelvis — guide to neutral (not posterior tilt, not excessive lordosis)
- Head over trunk over pelvis over feet = vertical alignment
-
Weight-shift laterally:
- KPC: Pelvis — shift to the right → right hip loads, left foot lightens → left foot is freed for stepping
- Facilitate hip abductor activation on right (Trendelenburg prevention): gentle pressure into the right iliac crest downward
-
Forward weight-shift:
- Guide CoM forward → child must recruit ankle strategy (calf/dorsiflexor co-contraction)
- Progress to stepping forward with the lightened limb
-
Single-leg stance preparation:
- Child standing, weight on right leg
- Therapist at right pelvis — stabilize the right pelvis
- Left knee slowly raised (hip flexion) — check for trunk lateral lean (should not be excessive)
🔵 POSITION 8: GAIT TRAINING
Analysis before training — What to observe:
| Gait Phase | Common CP Deviations | NDT Target |
|---|---|---|
| Initial contact | No heel-strike (equinus) | Inhibit plantarflexors, facilitate TA activation |
| Loading response | Knee hyperextension OR excessive flexion | Knee control facilitation |
| Midstance | Trendelenburg sign (hip drop) | Facilitate hip abductor activation |
| Terminal stance | No push-off (spastic plantarflexors block it) | Facilitate calf eccentric then concentric |
| Swing phase | Circumduction (hip hikes to clear foot) | Facilitate hip flexion + knee flexion (limb shortening) |
| Trunk | Excessive lateral trunk sway | Stabilize pelvis, improve hip abductor strength |
Demonstration — Gait facilitation with pelvic KPC:
- Stand behind and slightly to one side of the child
- Hands on iliac crests (bilateral)
- Facilitate reciprocal pelvic rotation: As right leg steps forward, right pelvis rotates forward → hands guide this
- Facilitate pelvic lateral tilt: As right leg enters stance, slightly lower the right side of pelvis (simulate normal pelvic obliquity)
- Progress: Reduce hands to one pelvis side → then fingertip contact → then remove
Facilitation of swing phase (for circumduction):
- Assist the hip flexion and knee flexion of the swing limb using a hand under the thigh
- Tap the anterior tibialis (below the knee on the shin) during swing to facilitate dorsiflexion
PART 6: CONDITION-SPECIFIC DEMONSTRATIONS
🟠 SPASTIC HEMIPLEGIA (One Side Affected)
Typical posture: Affected arm — shoulder internally rotated, elbow flexed, wrist/fingers flexed; Affected leg — hip internally rotated, knee may hyperextend, equinovarus foot
Key NDT Demo sequence:
- Inhibit upper limb spasticity (RIP):
- External rotation of shoulder + elbow extension + wrist/finger extension + forearm supination
- Hold the position slowly, 20–30 seconds — tone will gradually decrease
- Weight-bearing through affected arm:
- Seat child in side-sitting with affected arm extended to the side (hand flat on mat)
- Guide weight through that arm (approximation through the shoulder)
- Activates proprioceptors, normalizes tone, facilitates triceps and shoulder stabilizers
- Bilateral hand activities:
- After tone inhibition, present toys requiring two hands (cylinder to hold, ball to push)
- Guide the affected hand to participate — do not let the child ignore it (forced use concept)
- Lower limb — gait preparation:
- Inhibit equinovarus: heel cup + slow dorsiflexion + eversion + hip ER
- Practice weight transfer in standing: shift onto affected leg, facilitate hip abductors
🟡 SPASTIC DIPLEGIA (Both Legs, Arms Relatively Spared)
Typical posture: Scissoring (hip adductor spasticity), crouched gait (hip/knee flexion), equinus
Key NDT Demo sequence:
- Hip adductor inhibition:
- Child supine, flex both hips and knees
- Slowly abduct both hips simultaneously — use slow rhythmic movement
- Work toward 45° abduction on each side (normal)
- Note: never force abduction against tight adductors — sustained slow pressure only
- Sitting with hip abduction (ring-sitting or W-sitting modification):
- Ring-sitting (long legs abducted and externally rotated in front) is preferred over W-sitting (internal rotation, which tightens the entire pattern)
- Guide pelvis to anterior tilt in this position
- Standing with equinus:
- Always inhibit plantarflexors before weight-bearing (heel cup, slow dorsiflexion, 15 seconds)
- Use AFOs if dynamic spasticity persists — AFO maintains the inhibited position functionally
- Gait:
- Facilitate hip extension in stance (push pelvis backward into extension at terminal stance)
- Facilitate knee extension in stance (check for crouch pattern)
🟢 HYPOTONIA (Low Tone — Down Syndrome, Hypotonic CP)
Opposite problem: Not too much tone but too little — child collapses into gravity
Key NDT Demo sequence:
- Activation techniques (NOT inhibition):
- Tapping: Quick mechanical tap directly over the muscle belly to activate it (e.g., tap the quadriceps during sit-to-stand to facilitate knee extension)
- Approximation/compression: Press joint surfaces together to increase co-contraction and stability awareness
- Fast movements: Brief, quick stretches to activate muscle spindles (opposite of spasticity management)
- Trunk activation in sitting:
- Child on therapy ball — use fast tilts (not slow) to provoke quick equilibrium responses
- Place hands on trunk and give quick lateral perturbations — child must react
- Prone facilitation:
- Use prone over a wedge or therapy ball (prone increases flexor tone via TLR-prone)
- Facilitate neck extension + scapular retraction (tap the paraspinals and scapular retractors)
- Standing with compression:
- Child standing, hands on pelvis
- Give gentle vertical compression (press downward through the pelvis into the floor) — activates postural muscles throughout the axial skeleton
- Child must hold the position against this load
🔴 DYSKINETIC / ATHETOID CP (Fluctuating Tone)
Challenge: Tone fluctuates (hypo → hyper → hypo) — unpredictably; involuntary movements disrupt voluntary function
Key NDT Demo sequence:
- Goal: Proximal stability first
- These children have excellent desire to move but no stable base — fix the trunk and pelvis before asking for any upper limb function
- Seat child with trunk supported by the therapist (hands on pelvis + thorax)
- Reduce all extraneous stimulation (noise, visual distractors increase dyskinesia)
- Work in gravity-assisted positions:
- Side-lying reduces the effect of gravity and reduces dyskinetic movements
- Prone over a wedge is also useful
- Slow rhythmic input calms dyskinesia:
- Slow rhythmic rotation at the pelvis and shoulder girdle reduces involuntary movements
- Slow sustained compression through the joints (not quick — quick input worsens dyskinesia)
- Distal tasks after proximal control established:
- Only after the trunk is stabilized can the child attempt fine motor tasks
- Use wrist weights or weighted spoons to dampen involuntary arm movements
PART 7: CAREGIVER / PARENT TRAINING DEMONSTRATIONS
The child spends 1 hour in therapy. Carryover at home is the multiplier.
Teach parents these key techniques:
| Home Activity | NDT Principle Applied |
|---|---|
| Carrying position | Carry child facing away from you, supporting under thighs (hips abducted/flexed) — avoids hip adductor/extensor spasticity pattern |
| Floor play | Encourage ring-sitting, not W-sitting; use prone propping on elbows for play |
| Bath time | Slow limb elongation in warm water (warmth reduces tone); practice rolling in bath |
| Dressing | Always dress affected limb first; dress in side-lying to avoid TLR-supine spasticity |
| Feeding | Seat child with trunk supported, pelvis in neutral; head midline; stabilize jaw from below if needed |
| Sleep positioning | Side-lying with pillow between knees (hip abduction) avoids scissoring in sleep |
Summary: Order of a Typical NDT Session
1. OBSERVE (2–3 min) — Posture, tone, spontaneous movement before touching
2. ASSESS (3–5 min) — Tone (Ashworth/Tardieu), reflexes, postural reactions
3. INHIBIT (5–10 min) — Reduce abnormal tone using RIPs, slow elongation, rhythmic rotation
4. PREPARE (5 min) — Align pelvis/trunk; activate target muscles
5. FACILITATE (20–30 min) — Practice developmental activities at child's level; use KPCs
6. FUNCTION (10–15 min) — Integrate into real task (reaching, sit-to-stand, walking)
7. HOME PROGRAM (5 min) — Teach/review 1–2 carryover activities with caregiver
Clinical images sourced from published pediatric rehabilitation literature. Techniques described based on: Bradley and Daroff's Neurology in Clinical Practice (NDT/Bobath handling, p. 1166–1168) and Harriet Lane Handbook 23rd ed. (pediatric interdisciplinary rehabilitation).
Ndt which book to refer demonstration
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Now I have the complete picture of what's in the library. The honest answer is important here.
NDT-Specific Books — What's in This Library vs. What You Actually Need
What This Medical Library Contains
The textbooks available here are primarily medical/clinical reference books (neurology, pediatrics, surgery, pharmacology, etc.). The NDT/Bobath content available is:
| Book in Library | NDT Content Available |
|---|---|
| Bradley and Daroff's Neurology in Clinical Practice | Best available here — covers Bobath technique, neurofacilitation, motor learning, physical therapy approaches (pp. 1166–1168) |
| The Harriet Lane Handbook | Pediatric interdisciplinary rehab team structure (PT, OT, SLP roles) |
| Adams and Victor's Principles of Neurology | Neurological basis of movement disorders |
These are good background books but do not contain NDT handling demonstrations.
The Dedicated NDT Books You Should Actually Use
These are the authoritative, demonstration-rich books used by NDTA-certified therapists worldwide. They are not in this library but are the standard references:
1. "Normal and Abnormal Development of the Brain and its Relationship to Movement" — Berta and Karel Bobath
- The original foundational text from the founders of NDT
- Explains the neurophysiological basis of all NDT handling principles
- Required reading before any practical course
2. "Motor Development in the Normal Child" — Berta Bobath
- Step-by-step descriptions of normal motor milestones as the basis for NDT treatment progression
- Explains postural reactions, reflex integration, and tone development
3. "Cerebral Palsy — Assessment, Treatment and Management" — Suzann Campbell, Diane Vander Linden, Robert Palisano
- Most comprehensive modern pediatric NDT textbook
- Detailed chapters on assessment (GMFCS, GMFM), handling for each CP type, evidence base
- Has illustrated handling techniques
4. "Children with Cerebral Palsy: A Manual for Therapists, Parents and Community Workers" — Archie Hinchcliffe
- Extremely practical with drawings and step-by-step demonstrations
- Widely used in low- and middle-income countries
- Covers all developmental positions with illustrated caregiver training
5. "Physiotherapy for Children" — Karen Dodd, Nicholas Taylor, Diane Damiano (Eds.)
- Evidence-based pediatric PT textbook
- NDT, CIMT, strengthening, gait training all covered with clinical protocols
6. "Neuro-Developmental Treatment (NDT) Practice Guidelines" — NDTA (Neurodevelopmental Treatment Association)
- Official clinical practice guidelines from the certifying body
- Available directly from NDTA website (ndta.org)
- Most current evidence-based framework
7. "Handling the Young Child with Cerebral Palsy at Home" — Nancie Finnie
- Best book specifically for parent/caregiver training demonstrations
- Illustrated handling for feeding, dressing, carrying, bathing, positioning
- A classic — nearly every NDT therapist recommends it to families
8. "Pediatric Physical Therapy" — Jan Tecklin (Ed.)
- Comprehensive textbook covering all pediatric conditions including CP, spina bifida, hypotonia
- NDT approach integrated with evidence-based practice throughout
For Practical Demonstration Learning (Beyond Books)
Books alone are insufficient for NDT — it is a hands-on skill. The best supplementary resources:
| Resource | What It Offers |
|---|---|
| NDTA Basic Course (ndta.org) | 8-day hands-on certified training with live demonstrations |
| NDTA online video library | Recorded handling demonstrations by certified instructors |
| YouTube — "NDT handling" | Free demonstration videos (variable quality — use only NDTA-affiliated sources) |
| Mentorship with NDTC therapist | Real-time feedback on your handling — irreplaceable |
| "Handling in Hemiplegia" — Berta Bobath | Specific handling demonstrations for stroke/hemiplegia, applicable to pediatric hemiplegia |
Bottom Line
For demonstrations specifically: Start with Nancie Finnie's "Handling the Young Child with Cerebral Palsy at Home" (caregiver demonstrations) and Suzann Campbell's "Cerebral Palsy" (clinical handling). Then enroll in an NDTA-certified basic course — no book fully substitutes for hands-on training with an experienced NDT instructor.
This is a shared conversation. Sign in to Orris to start your own chat.