Anti allergiec drugs for pharmacology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer.
Anti-Allergic Drugs (Pharmacology)
Overview: Histamine & Allergic Reactions
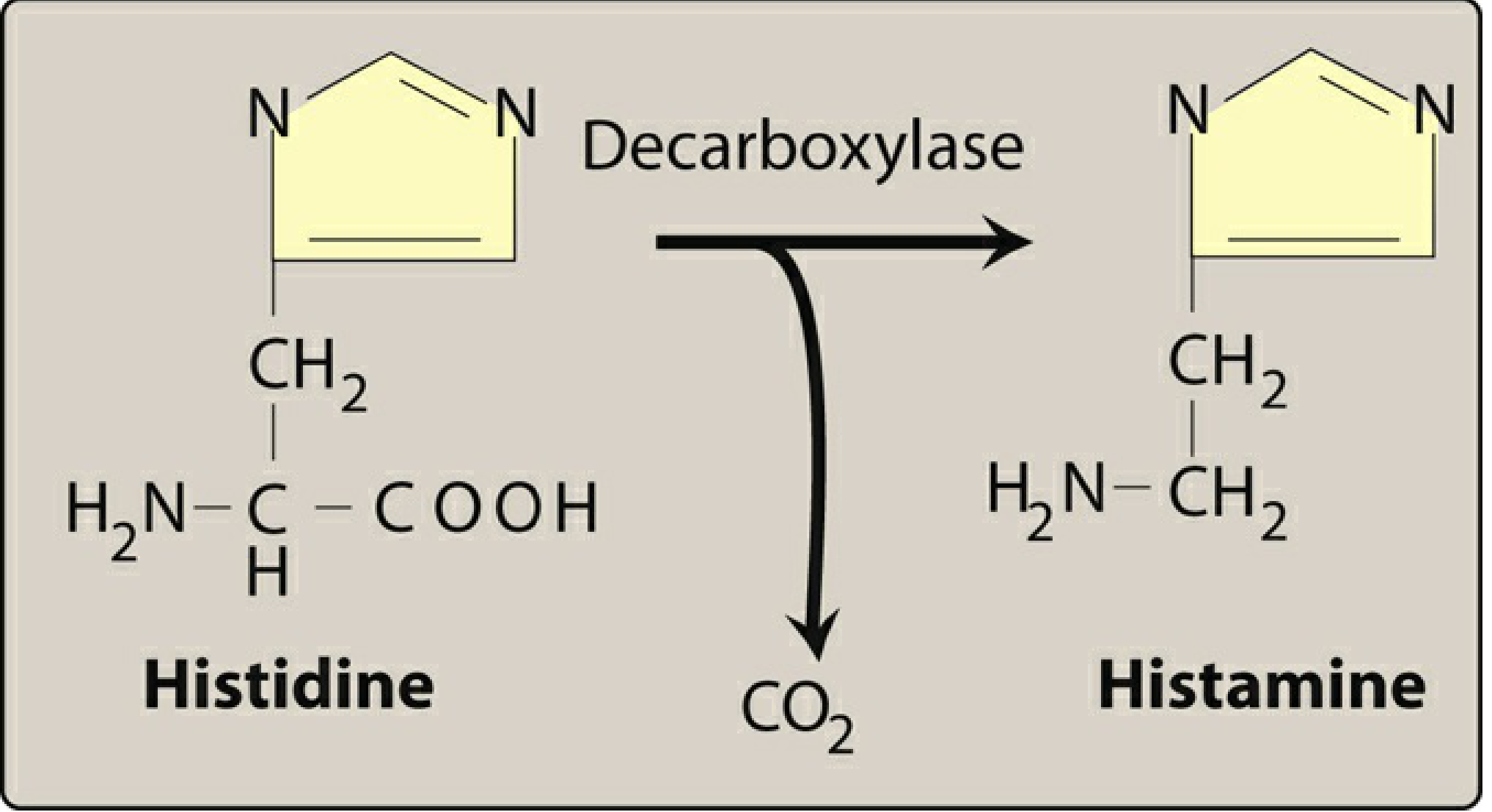
Histamine is the primary mediator of allergic reactions. It is synthesized by decarboxylation of histidine (by histidine decarboxylase) and stored in mast cells and basophils. On release, it binds to H1 and H2 receptors causing the spectrum of allergic symptoms.
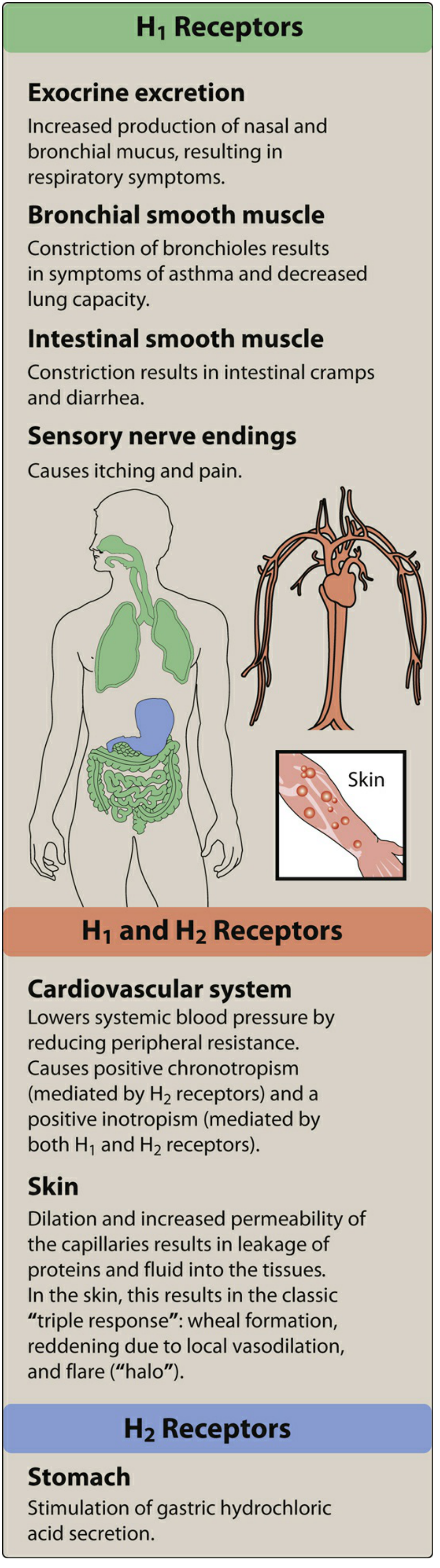
H1 receptor effects: Smooth muscle contraction, ↑ capillary permeability, vasodilation (via NO), bronchoconstriction, pruritus
H2 receptor effects: Gastric acid secretion, some cardiac effects
Classification of Anti-Allergic Drugs
I. H1-RECEPTOR BLOCKERS (Antihistamines)
The cornerstone of anti-allergic pharmacotherapy. Divided into two generations:
First-Generation H1 Blockers
Mechanism: Competitive H1 receptor antagonists (inverse agonists). They stabilize the inactive form of H1 receptors. They cross the blood-brain barrier (lipophilic) and block muscarinic, α-adrenergic, and serotonin receptors as well.
Chemical Classes & Drugs:
| Class | Examples | Key Features |
|---|---|---|
| Ethanolamines | Diphenhydramine (Benadryl), Dimenhydrinate, Doxylamine | High sedation, significant anticholinergic effects |
| Alkylamines | Chlorpheniramine, Brompheniramine, Triprolidine | Less sedation, CNS stimulation possible |
| Piperazines | Hydroxyzine (Vistaril), Meclizine, Cyclizine | Hydroxyzine: anxiolytic; Meclizine: motion sickness |
| Phenothiazines | Promethazine (Phenergan) | Strong antiemetic, high sedation |
| Piperidines | Cyproheptadine | Also blocks 5-HT; used for appetite stimulation |
| Ethylenediamines | Clemastine | Moderate sedation |
Pharmacokinetics:
- Oral: well absorbed; onset 15–30 min
- Duration: 4–6 hours
- Metabolized by CYP450 in liver
Therapeutic Uses:
- Allergic rhinitis, urticaria, atopic dermatitis
- Motion sickness (dimenhydrinate, meclizine)
- Nausea/vomiting (promethazine)
- Sleep aid (diphenhydramine, doxylamine)
- Anaphylaxis (adjunct to epinephrine)
- Common cold (drying of secretions)
Adverse Effects:
- CNS: Sedation, impaired cognition, dizziness (most common)
- Anticholinergic: Dry mouth, urinary retention, blurred vision, constipation, tachycardia
- Paradoxical CNS excitation in children (insomnia, tremors)
- Appetite stimulation (cyproheptadine)
- Toxic doses: Convulsions, hyperthermia
Second-Generation H1 Blockers
Mechanism: Selective peripheral H1 blockers. Made polar (carboxyl groups added) → do not cross the blood-brain barrier → minimal sedation. No significant anticholinergic effects.
Drugs:
| Drug | Brand | Notes |
|---|---|---|
| Loratadine | Claritin | Least sedating; metabolized to desloratadine |
| Desloratadine | Clarinex | Active metabolite of loratadine |
| Fexofenadine | Allegra | Least sedating; no CYP450 interaction |
| Cetirizine | Zyrtec | Carboxylated hydroxyzine; mild sedation possible |
| Levocetirizine | Xyzal | Active enantiomer of cetirizine |
| Azelastine | Astelin | Nasal spray; also ophthalmic formulation |
| Olopatadine | Pataday | Ophthalmic; used for allergic conjunctivitis |
| Bepotastine | Bepreve | Ophthalmic |
| Alcaftadine | Lastacaft | Ophthalmic |
| Ketotifen | Zaditor | Ophthalmic; mast cell stabilizer properties |
Therapeutic Uses:
- Seasonal/perennial allergic rhinitis (first-line)
- Urticaria, allergic skin conditions
- Allergic conjunctivitis (topical agents)
Adverse Effects:
- Minimal sedation (fexofenadine, loratadine, desloratadine = least sedating)
- Cetirizine/levocetirizine: mild drowsiness in some patients
- No anticholinergic effects
II. MAST CELL STABILIZERS
Mechanism: Prevent degranulation of mast cells → inhibit release of histamine, leukotrienes, and other mediators. Work best as prophylactic agents.
| Drug | Route | Use |
|---|---|---|
| Cromolyn sodium | Inhaled / nasal / ophthalmic | Allergic rhinitis, asthma prophylaxis, conjunctivitis |
| Nedocromil | Inhaled | Asthma prophylaxis |
| Lodoxamide | Ophthalmic | Allergic conjunctivitis |
| Ketotifen | Oral / ophthalmic | Also H1 blocker |
Key point: Must be used before allergen exposure. Not useful for acute attacks.
III. CORTICOSTEROIDS
The most potent anti-inflammatory/anti-allergic drugs.
Mechanism: Bind glucocorticoid receptors → ↓ cytokine production, ↓ eosinophil survival, ↓ mast cell mediator release, ↓ vascular permeability.
| Drug | Route | Use |
|---|---|---|
| Fluticasone, Mometasone, Budesonide | Intranasal | First-line for allergic rhinitis |
| Beclomethasone, Flunisolide | Inhaled | Asthma |
| Prednisolone, Dexamethasone | Oral/IV | Severe allergy, anaphylaxis, asthma exacerbation |
| Hydrocortisone, Triamcinolone | Topical | Urticaria, atopic dermatitis |
IV. LEUKOTRIENE RECEPTOR ANTAGONISTS (LTRAs)
Mechanism: Block cysteinyl leukotriene (LTC4, LTD4, LTE4) receptors → ↓ bronchoconstriction, ↓ mucus secretion, ↓ airway inflammation.
| Drug | Use |
|---|---|
| Montelukast (Singulair) | Allergic rhinitis, asthma; safe in children |
| Zafirlukast | Asthma |
Zileuton blocks 5-lipoxygenase → ↓ leukotriene synthesis (upstream mechanism).
V. EPINEPHRINE (Adrenaline)
Drug of choice for anaphylaxis.
Mechanism: α1 agonist → vasoconstriction, ↓ edema; β2 agonist → bronchodilation; β1 → ↑ cardiac output.
Route: IM (vastus lateralis) or IV in severe cases (EpiPen).
VI. ANTI-IgE THERAPY (Biologics)
| Drug | Mechanism | Use |
|---|---|---|
| Omalizumab (Xolair) | Monoclonal antibody against free IgE → ↓ mast cell/basophil activation | Severe allergic asthma, chronic urticaria |
| Dupilumab (Dupixent) | Blocks IL-4Rα → inhibits IL-4 and IL-13 signaling | Atopic dermatitis, asthma |
| Mepolizumab, Benralizumab | Anti-IL-5 / anti-IL-5Rα → ↓ eosinophils | Eosinophilic asthma |
VII. β2-AGONISTS (for Allergic Bronchospasm)
| Drug | Type | Use |
|---|---|---|
| Salbutamol (Albuterol) | Short-acting (SABA) | Acute bronchospasm |
| Salmeterol, Formoterol | Long-acting (LABA) | Asthma maintenance (with ICS) |
Summary Comparison: 1st vs 2nd Generation Antihistamines
| Feature | 1st Generation | 2nd Generation |
|---|---|---|
| CNS penetration | Yes | Minimal |
| Sedation | High | Low to none |
| Anticholinergic effects | Yes | No |
| Duration | 4–6 hrs | 12–24 hrs |
| Selectivity | Non-selective | Peripheral H1 selective |
| Examples | Diphenhydramine, Chlorpheniramine, Promethazine | Loratadine, Fexofenadine, Cetirizine |
Key Exam Points
- Epinephrine = drug of choice in anaphylaxis (not antihistamines)
- Fexofenadine = least sedating, no QTc prolongation
- Diphenhydramine = prototype 1st-gen; also used as sleep aid and antiemetic
- Promethazine = contraindicated in children < 2 years (respiratory depression)
- Meclizine/Dimenhydrinate = motion sickness
- Cyproheptadine = serotonin antagonist + appetite stimulant
- Cromolyn = prophylaxis only, not for acute attacks
- Montelukast = safe in children with allergic rhinitis + asthma
- Omalizumab = for IgE-mediated severe allergic disease
Sources: Lippincott Illustrated Reviews: Pharmacology; Katzung's Basic and Clinical Pharmacology, 16th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.