What is Differential for Large weird looking lymphnodes
Reading File
Finding Sources
Finding Sources
Searching PubMed
lymphadenopathy differential diagnosis
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have everything needed for a complete, well-organized answer.
Differential Diagnosis: Large / Abnormal-Looking Lymph Nodes (Lymphadenopathy)
"Large, weird-looking" lymph nodes - clinically termed lymphadenopathy - have a broad differential. The most useful framework organizes causes by category, then narrows by location, node characteristics, patient age, and associated symptoms.
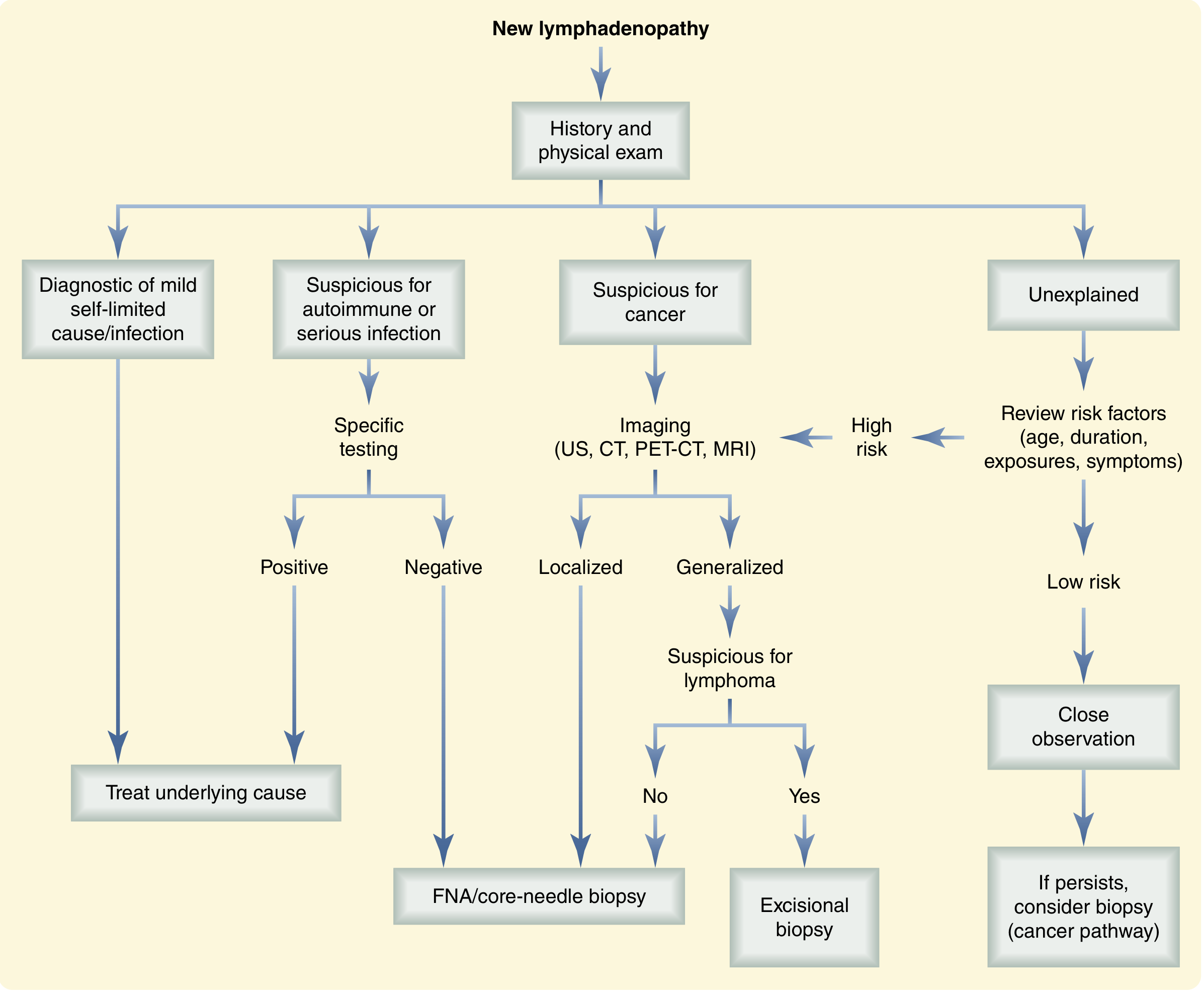
Diagnostic Algorithm
The Full Differential (by Category)
1. Infectious (Most Common Overall)
| Subtype | Examples |
|---|---|
| Bacterial | Group A Strep, Staph skin infections, syphilis, cat-scratch disease (Bartonella henselae), typhoid fever, tuberculosis, bubonic plague (Yersinia pestis - "buboes") |
| Mycobacterial | TB (classic cervical adenopathy = "scrofula"), atypical mycobacteria (MAC) |
| Viral | EBV (infectious mononucleosis), CMV, HIV |
| Fungal | Histoplasmosis, blastomycosis, coccidioidomycosis |
| Parasitic | Toxoplasmosis, malaria |
2. Malignant (Must Not Miss)
| Type | Notes |
|---|---|
| Hodgkin Lymphoma | Classic "rubbery," non-tender, mediastinal mass; B symptoms (fever, night sweats, weight loss) |
| Non-Hodgkin Lymphoma | Wide spectrum; generalized adenopathy more common |
| Leukemia | CLL, ALL - diffuse adenopathy |
| Myeloproliferative neoplasms | |
| Metastatic solid tumors | Breast → axillary nodes; head/neck, thyroid, lung → cervical/supraclavicular; prostate → iliac; GI/GYN → inguinal |
Key rule: Supraclavicular and epitrochlear adenopathy in any adult is highly suspicious for malignancy until proven otherwise. - Goldman-Cecil Medicine, p. 1775
3. Immune-Mediated / Autoimmune
- Rheumatoid arthritis
- Systemic lupus erythematosus (SLE)
- Drug reactions (antiepileptics, antibiotics, allopurinol - can mimic lymphoma histologically)
4. Rare / Unusual ("Weird-Looking" Nodes)
These are especially relevant when nodes appear atypical on imaging or biopsy:
| Condition | Key Feature |
|---|---|
| Sarcoidosis | Non-caseating granulomas; bilateral hilar adenopathy |
| Castleman Disease | Unicentric or multicentric; can involve mediastinum |
| Kikuchi-Fujimoto Disease | Necrotizing lymphadenitis; young women; self-limiting |
| Kimura Disease | Asian males; eosinophilia; soft tissue masses near lymph nodes |
| Rosai-Dorfman Disease | Sinus histiocytosis with massive lymphadenopathy |
| Kawasaki Disease | Vasculitis; mainly children; cervical adenopathy |
| Gaucher / Niemann-Pick | Storage diseases |
| Amyloidosis | Associated with myeloma or chronic inflammation |
| Endocrinopathies | Thyroid disease, Addison disease |
Location-Based Differential
| Location | Think First About |
|---|---|
| Cervical / submandibular | Infection (EBV, strep), head/neck cancer, lymphoma, TB |
| Supraclavicular | Lung/esophageal cancer, GI cancer, lymphoma - high malignancy risk |
| Axillary | Breast cancer, infection, lymphoma |
| Mediastinal | Lymphoma, sarcoidosis, Castleman, lung cancer, anthrax |
| Epitrochlear | Sarcoidosis, lymphoma, infections of forearm - always worry |
| Inguinal | STIs, lower extremity infections, GU/GYN/GI malignancy, lymphoma |
Sabiston Textbook of Surgery, p. 1458
Red Flags Suggesting Malignancy
- Age >40 years (4% risk vs. 0.4% in <40 years)
- Hard, fixed, non-tender node
- Supraclavicular or epitrochlear location
- B symptoms (fever, drenching night sweats, >10% weight loss)
- Progressive growth over weeks-months
- Node persisting >4-6 weeks with no obvious benign cause
Workup at a Glance
- History and exam - duration, location, tenderness, mobility, associated symptoms, exposures, medications
- CBC with differential - atypical lymphocytes suggest EBV/CMV
- Serology - Monospot, EBV/CMV titers, HIV, ANA, RPR as directed
- Imaging - Ultrasound (children, first-line adults), CT chest/abdomen/pelvis (suspicious nodes), PET-CT (staging once malignancy confirmed)
- Biopsy - FNA/core needle for localized suspicious nodes; excisional biopsy preferred when lymphoma is suspected (to preserve architecture for pathology)
Recent Literature
Three recent reviews confirm this framework remains current:
- Lymphadenopathy: Evaluation and Differential Diagnosis - Falk et al., Am Fam Physician 2025 (PMID: 40961306)
- Lymphadenopathy: Differential Diagnosis and Indications for Evaluation - Stanford et al., Pediatr Rev 2024 (PMID: 39085185) - pediatric focus
- Infectious Mononucleosis: An Updated Review - Leung et al., Curr Pediatr Rev 2024 (PMID: 37526456)
Bottom line: Most lymphadenopathy in young patients resolves with infection treatment. In adults >40, nodes that are large, hard, fixed, supraclavicular, or persistent without clear cause warrant imaging and biopsy. The "weird-looking" quality on exam or imaging should push you toward lymphoma, metastatic cancer, or one of the unusual entities (sarcoidosis, Castleman, Kikuchi).
This is a shared conversation. Sign in to Orris to start your own chat.