Varicose veins and causes of unilateral varicose veins and management in detail with examination points and history
Reading File
Finding Sources
Finding Sources
Searching Images
varicose veins anatomy examination
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Now I have comprehensive information. Let me compile a detailed, well-structured response.
Varicose Veins — Comprehensive Clinical Overview
Definition
Varicose veins are dilated, tortuous, elongated superficial veins that have lost their normal valve competence. They are present in at least 10% of the general population, arising most commonly in the lower limb superficial venous system.

Anatomy — The Venous System of the Lower Limb
Understanding the anatomy is essential to understanding why varicose veins develop.
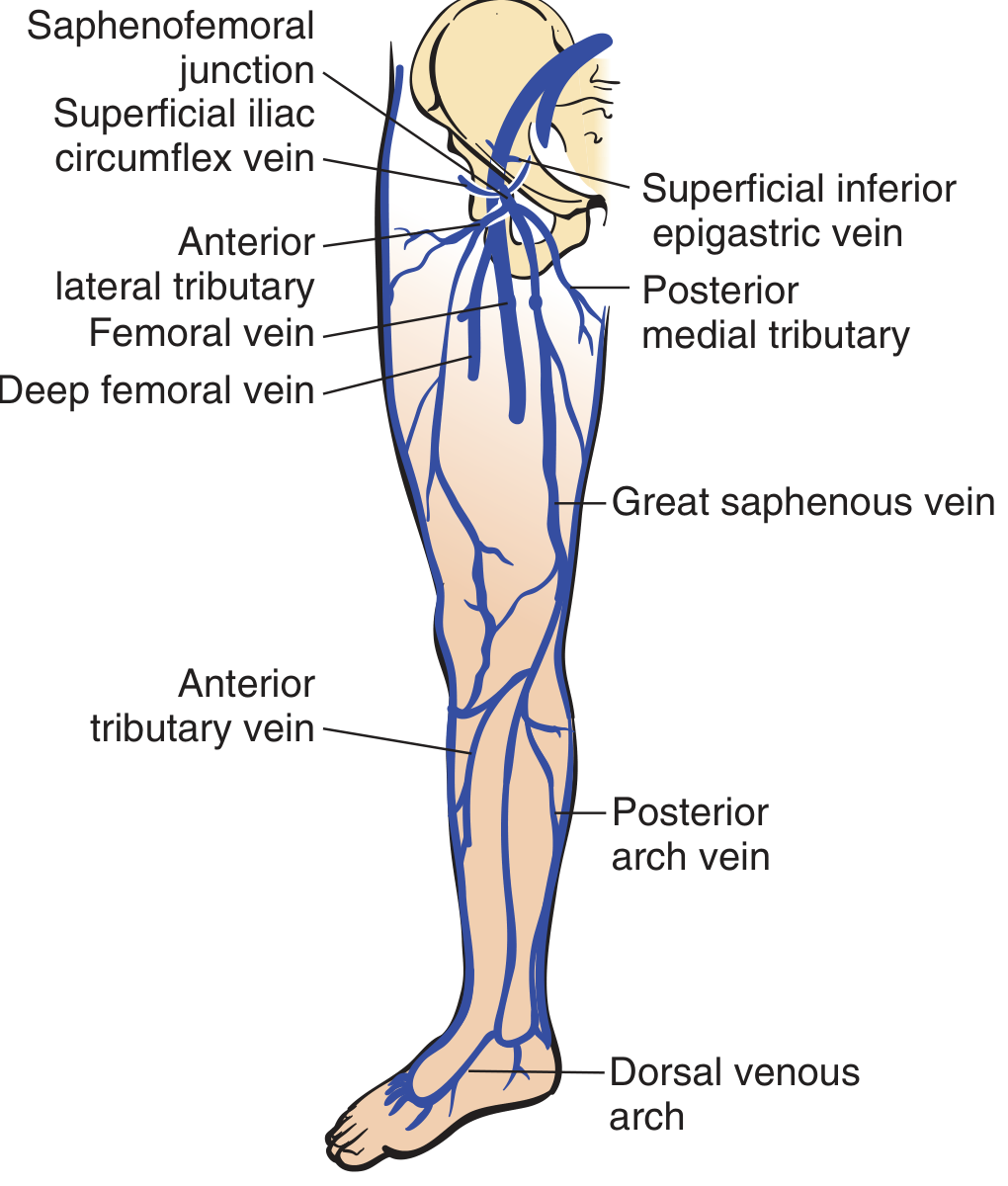
Three venous systems operate together:
- Deep veins — femoral, popliteal, tibial; enclosed in fascia and muscle
- Superficial veins — Great Saphenous Vein (GSV) and Small Saphenous Vein (SSV) with their tributaries
- Perforating (communicating) veins — connect the two systems; have valves that normally only allow flow from superficial → deep
Normal physiology:
- Calf muscle contraction generates up to 300 cm H₂O pressure, pumping blood proximally through the deep veins
- Valves prevent retrograde flow
- During relaxation, blood flows from the superficial system through perforators into deep veins (superficial system = "atrium"; deep veins = "ventricle")
- Standing still creates hydrostatic pressure of ~70–80 cm H₂O at the foot
— Pfenninger and Fowler's Procedures for Primary Care, p. 636
Pathophysiology
Valve incompetence is the central event — whether primary or secondary:
- Saphenofemoral junction (SFJ) incompetence → retrograde flow from common femoral → GSV → progressive dilation → distal valve failure → cascade incompetence of entire saphenous system
- Perforator incompetence → during calf contraction, blood flows from deep system backward into the superficial system (instead of the reverse) → venous hypertension → sustained dilation → stasis dermatitis, pigmentation, lipodermatosclerosis, ulceration
— Pfenninger and Fowler's Procedures for Primary Care, p. 637
Classification
| Type | Description |
|---|---|
| Primary varicose veins | Intrinsic abnormalities of the venous wall — no underlying deep venous pathology |
| Secondary varicose veins | Consequence of deep or superficial venous thrombosis, or arteriovenous fistula with resulting venous hypertension |
By vessel size (Sadick classification):
| Type | Vessel | Diameter | Color |
|---|---|---|---|
| I | Telangiectases (spider veins) | 0.1–1 mm | Red |
| Ia | Telangiectatic matting | <0.2 mm | Red |
| II | Venulectasia | 1–2 mm | Violaceous |
| III | Reticular veins | 2–4 mm | Blue |
| IV | Non-saphenous varicosities (perforator-related) | 3–8 mm | Blue |
| V | Saphenous varicosities (GSV/SSV truncal) | ≥5–8 mm | Blue |
— Pfenninger and Fowler's Procedures for Primary Care, p. 637 / Dermatology 2-Volume Set 5e, p. 3136
Risk Factors
- Female sex
- Obesity
- Family history (strong genetic component)
- Prolonged standing or inactivity
- Pregnancy (increased intra-abdominal pressure + progesterone-induced vein wall relaxation)
- Previous DVT or thrombophlebitis
- Age
— Schwartz's Principles of Surgery, 11th Ed, p. 1023
Causes of Unilateral Varicose Veins
Bilateral varicose veins are generally due to primary (constitutional) venous wall weakness. Unilateral varicose veins demand active exclusion of secondary causes:
1. Deep Vein Thrombosis (DVT) — most important
- Previous DVT causes valve destruction in the deep system → post-thrombotic syndrome
- Deep venous occlusion forces collateral drainage through the superficial system → secondary varicosities
- Look for: history of immobilisation, thrombophilia, prior leg swelling, asymmetric oedema
2. Iliac Vein or IVC Compression/Obstruction
- May-Thurner syndrome: Left common iliac vein compression by the right common iliac artery → unilateral left leg varicosities
- Pelvic masses (fibroid uterus, ovarian cysts, lymph nodes, retroperitoneal tumours) compressing iliac vein
- Pregnancy — particularly asymmetric if uterus rotates
3. Arteriovenous Fistula (AVF)
- Congenital or acquired (post-trauma, post-surgical)
- High-pressure arterial flow enters the venous system → venous hypertension → varicosities
- Clinical clue: warm limb, thrill/bruit, dilated pulsatile veins, leg length discrepancy
4. Congenital Venous Anomalies
- Klippel-Trénaunay syndrome: triad of port wine stain, varicosities, and limb hypertrophy — typically unilateral
- Involves posterolateral tributary veins and anterolateral superficial thigh veins
- Associated with absence of deep venous system (surgical stripping contraindicated)
5. Pelvic Congestion Syndrome
- Ovarian vein incompetence / pelvic varicosities draining to the thigh
- Typical pattern: posterior thigh varicosities — a key clinical sign pointing to a pelvic venous source
- Common in multiparous women
6. Inferior Vena Cava (IVC) Obstruction
- Thrombosis, tumour invasion (renal cell carcinoma), external compression
- Bilateral initially but can present unilaterally depending on level and collateral pathways
7. Trauma or Previous Surgery
- Post-surgical ligation of deep veins or previous stripping procedures
- Limb trauma causing AVF or deep vein damage
8. Tumour Infiltrating Pelvic/Inguinal Lymph Nodes
- Lymphatic-venous communications allow recurrence of varicosities after treatment
— Pfenninger and Fowler's Procedures for Primary Care / Schwartz's Principles of Surgery / search_image analysis
History — Key Points to Elicit
Presenting Complaint
- Site, distribution, and onset of varicosities
- Cosmetic concern only, or symptomatic?
Symptoms
- Aching, heaviness, dragging in the leg (worse after prolonged standing, relieved by elevation)
- Itching or burning over varicosities
- Ankle swelling (especially evening)
- Restless legs or cramps at night
- Skin changes — pigmentation, eczema, ulceration
Aggravating / Relieving Factors
- Worse with prolonged standing/sitting → better with leg elevation (classic)
- Worse in hot weather, premenstrually
Complications to Ask About
- Thrombophlebitis — localised redness, tenderness, hard cord
- Bleeding — spontaneous or traumatic bleeding from varicosity
- Venous ulceration — around the medial malleolus
- Lipodermatosclerosis — woody induration and pigmentation of gaiter area
Relevant Past History
- Previous DVT, PE, or thrombophlebitis
- Unilateral only: previous hip/knee surgery, trauma, pelvic surgery, malignancy
- Pregnancies — how many, which legs affected
- Previous treatment for varicosities (sclerotherapy, stripping)
Family History
- Varicose veins (strong hereditary component)
- Thrombophilia
Drug/Social History
- OCP / HRT (venous thrombosis risk)
- Occupation — prolonged standing (nurse, teacher, surgeon)
- BMI
Systems Review (for secondary causes)
- Pelvic pain, dyspareunia → pelvic congestion
- Weight loss, haematuria → malignancy / RCC / IVC thrombosis
- Skin birthmark, limb length discrepancy → Klippel-Trénaunay
Examination
The patient must be examined standing in good light, examining the whole lower limb from groin to foot.
General Inspection
- Distribution: unilateral vs bilateral; GSV distribution (medial) vs SSV distribution (posterior/lateral calf)
- Assess entire limb for skin changes
Look
| Feature | Significance |
|---|---|
| Dilated tortuous superficial veins | Primary finding |
| Saphena varix — groin swelling that disappears on lying | SFJ incompetence |
| Medial ankle / gaiter hyperpigmentation (haemosiderin) | Chronic venous hypertension |
| Venous eczema (stasis dermatitis) | CVI |
| Lipodermatosclerosis — woody induration of the gaiter area | Advanced CVI |
| Venous ulcer — typically medial malleolar | Severe CVI |
| Port wine stain / limb hypertrophy | Klippel-Trénaunay |
| Posterior thigh distribution | Pelvic venous source |
Feel
- Temperature — warm over varicosities; very warm limb may suggest AVF
- Tenderness — localised tenderness over vein (thrombophlebitis)
- Oedema — pitting vs non-pitting; bilateral vs unilateral
- Lipodermatosclerosis — firm, woody induration; "inverted champagne bottle" leg
- Saphenofemoral junction — feel for saphena varix in the groin
Special Tests
1. Cough Impulse Test (Morrissey's test)
- Patient stands; place fingers over the SFJ in the groin
- Ask patient to cough
- A thrill or impulse felt = SFJ incompetence (valve failure)
2. Trendelenburg Test (Brodie-Trendelenburg)
- Elevate leg to empty veins → apply tourniquet at upper thigh → stand patient up
- Veins fill slowly from below (>30 sec) → tourniquet controls filling = SFJ incompetence confirmed (releasing tourniquet causes rapid retrograde filling)
- Veins fill rapidly from below despite tourniquet = perforator incompetence below the tourniquet
- Can repeat at different levels to locate incompetent perforators
3. Perthes' Test (deep vein patency)
- Apply tourniquet mid-thigh with patient standing
- Ask patient to walk / exercise for a few minutes
- Veins disappear → deep veins patent (blood redirected to deep system)
- Veins remain or pain worsens → deep vein obstruction or incompetent perforators (do NOT strip — deep veins may be the only functional drainage)
4. Fegan's Test (perforator localisation)
- Elevate leg; mark dimples along the line of the GSV (sites of incompetent perforators — fascial gaps)
- These correspond to standard perforator locations: Dodd (mid-thigh), Boyd (below knee), Cockett I/II/III (medial calf/ankle)
5. Tap Test (Schwartz test)
- Tap the vein proximally and feel for an impulse distally (or vice versa)
- Positive impulse transmitted = continuous column of blood = valve incompetence
6. Auscultation
- Over varicosity — bruit suggests AVF
7. Examine Abdomen and Pelvis
- Palpate for masses, hepatomegaly, lymphadenopathy
- In women with unilateral varicosities: bimanual pelvic examination if indicated
Investigations
| Investigation | Indication |
|---|---|
| Duplex Ultrasound (colour Doppler) | Gold standard — maps reflux, identifies SFJ/SPJ/perforator incompetence, assesses deep vein patency |
| Venography | Rarely needed; reserved for complex anatomy or pre-operative planning |
| CT/MR venography | Suspected iliac vein compression, pelvic congestion, IVC obstruction — especially for unilateral disease |
| Ankle-Brachial Pressure Index (ABPI) | Before compression therapy — exclude arterial disease (ABPI <0.7 is contraindication to compression) |
| Thrombophilia screen | Recurrent DVT / post-thrombotic secondary varicosities |
| Pelvic ultrasound | Suspected pelvic mass or pelvic congestion syndrome |
CEAP Classification (Clinical, Aetiological, Anatomical, Pathophysiological)
| Class | Description |
|---|---|
| C0 | No visible venous disease |
| C1 | Telangiectases / reticular veins |
| C2 | Varicose veins |
| C3 | Oedema |
| C4a | Pigmentation / eczema |
| C4b | Lipodermatosclerosis / atrophie blanche |
| C5 | Healed venous ulcer |
| C6 | Active venous ulcer |
Management
1. Conservative (All Patients)
- Weight reduction — reduces venous pressure
- Leg elevation — at rest and at night
- Avoid prolonged standing
- Exercise — regular walking activates the calf muscle pump
- Elastic compression stockings:
- 20–30 mmHg for mild symptoms
- 30–40 mmHg for moderate symptoms
- 40–50 mmHg for severe CVI / ulcers
- Knee-high to waist-high depending on extent of varicosities
- Provides sufficient symptom relief in many patients
— Schwartz's Principles of Surgery, p. 1023
2. Interventional Indications
Intervention is warranted when:
- Symptoms persist or worsen despite compression therapy
- Lipodermatosclerosis is present
- Active or recurrent venous ulceration
- Thrombophlebitis
- Bleeding from varicosity
- Patient preference (cosmesis)
3. Sclerotherapy
Mechanism: Sclerosant destroys venous endothelium → inflammation → fibrosis → obliteration
Sclerosing agents:
| Agent | Concentration for telangiectases | Concentration for large varicosities |
|---|---|---|
| Hypertonic saline | 11.7–23.4% | 23.4% |
| Sodium tetradecyl sulfate (STS) | 0.125–0.25% | 0.5–1% |
| Polidocanol | 0.5% | 0.75–1.0% |
- Foam sclerotherapy (sclerosant + air) is preferred for larger varicosities
- After injection: elastic bandage for 3–5 days, then compression stockings for ≥2 weeks
Complications: Allergic reaction, hyperpigmentation, thrombophlebitis, DVT, skin necrosis
Contraindications to sclerotherapy: Pregnancy, lactation, allergy, hypercoagulable state, non-ambulation, SFJ/SPJ reflux, vessels >6 mm (high recurrence risk), ABPI <0.7
— Pfenninger and Fowler's Procedures for Primary Care, p. 636
4. Endovenous Thermal Ablation
Indicated for symptomatic GSV or SSV reflux:
Radiofrequency Ablation (RFA) and Endovenous Laser Treatment (EVLT):
- GSV punctured under ultrasound guidance (distal thigh / proximal calf) with 21-gauge needle
- Guidewire → sheath → laser fibre or RFA catheter advanced to near SFJ
- Tumescent anaesthesia injected around the GSV
- Vein treated as catheter is withdrawn
- Results: durable ablation, comparable recurrence rates to open surgery, faster recovery
Risks: DVT, ecchymosis, saphenous nerve injury
— Schwartz's Principles of Surgery, p. 1024
5. Non-Thermal, Non-Sclerosant Ablation
- Mechanochemical ablation (MOCA) — combines catheter-based mechanical endoluminal injury with sclerosant (e.g., ClariVein)
- Cyanoacrylate glue (VenaSeal) — proprietary adhesive obliterates the vein lumen; no tumescent anaesthesia required; promising early results
6. Surgical Treatment
High saphenous ligation and stripping:
- Preferred for GSV >2 cm diameter
- Small incision in groin → ligate GSV flush with common femoral vein at SFJ + second incision just below knee
- GSV removed using blunt-tip catheter or invagination pin stripper
- Lower long-term recurrence than SFJ ligation alone
Complications: Ecchymosis, haematoma, lymphocele, DVT, infection, saphenous nerve injury (medial sensation loss)
Stab avulsion phlebectomy:
- For branch varicosities and larger residual varicosities after truncal ablation
- 2 mm stab incisions directly over varicosity → dissect and avulse the vein segment
- Bleeding controlled by elevation + compression + tumescent anaesthesia
— Schwartz's Principles of Surgery, p. 1024
Important Caveat: Perthes' Test Negative (Deep Vein Obstruction)
If deep veins are occluded (post-thrombotic), the superficial varicosities may represent collateral drainage. Stripping or ablation of these veins is contraindicated — it would critically impair venous return.
Complications of Untreated Varicose Veins
| Complication | Notes |
|---|---|
| Thrombophlebitis | Painful, red, indurated cord |
| Bleeding | Spontaneous or minor trauma → significant haemorrhage from attenuated vein |
| Chronic venous insufficiency | Oedema, pigmentation, lipodermatosclerosis |
| Venous ulcer | Medial malleolar; recalcitrant; significant morbidity |
| DVT | Especially with thrombophlebitis |
Key Sources:
- Schwartz's Principles of Surgery, 11th Ed, p. 1023–1024
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed, p. 636–638
- Dermatology 2-Volume Set, 5th Ed, p. 3136
This is a shared conversation. Sign in to Orris to start your own chat.