Congenital anomalies of the kidney: Hydronephrosis.and Ureterohydronephrosis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching Images
hydronephrosis kidney gross pathology dilation renal pelvis
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Now I have comprehensive information from multiple authoritative sources. Let me compile a thorough response.
Congenital Anomalies of the Kidney: Hydronephrosis and Ureterohydronephrosis
1. Definitions
Hydronephrosis is dilation of the renal pelvis and calyces, with accompanying atrophy of the parenchyma, caused by obstruction to the outflow of urine. The obstruction may be sudden or insidious and may occur at any level of the urinary tract, from the urethra to the renal pelvis.
Ureterohydronephrosis (hydroureteronephrosis) refers to combined dilation of the ureter and the renal pelvis/calyces, which occurs when the obstructing lesion is at or below the ureterovesical junction (UVJ), rather than at the ureteropelvic junction (UPJ).
2. Gross Pathology
FIG. 12.25 — Hydronephrosis (Robbins & Kumar Basic Pathology): Marked dilation of the pelvis and calyces with thinning of renal parenchyma.

3. Congenital Causes of Hydronephrosis
Congenital lesions that cause hydronephrosis/ureterohydronephrosis include:
| Lesion | Level | Result |
|---|---|---|
| Atresia of the urethra | Urethra | Bilateral hydroureteronephrosis + bladder distension |
| Posterior urethral valves (PUV) | Urethra | Bilateral hydroureteronephrosis |
| Ureteropelvic junction (UPJ) obstruction | UPJ | Hydronephrosis only (ureter NOT dilated) |
| Ureterovesical junction (UVJ) obstruction / Obstructed megaureter | UVJ | Hydroureteronephrosis |
| Aberrant renal artery compressing ureter | Ureter | Hydronephrosis |
| Abnormal renal position with ureteral kinking | Ureter | Hydronephrosis |
| Ureterocele | Intravesical | Hydroureteronephrosis of ipsilateral upper pole (duplex) |
| Vesicoureteral reflux | UVJ | Ureterohydronephrosis |
— Robbins & Kumar Basic Pathology; Smith and Tanagho's General Urology, 19th Edition; Goldman-Cecil Medicine
4. Ureteropelvic Junction (UPJ) Obstruction — The Most Common Congenital Cause
UPJ obstruction is the most common cause of prenatal hydronephrosis, accounting for up to 30% of urinary tract dilations detected on prenatal ultrasound. In children, it is seen more often in boys than girls (5:2 ratio).
Diagram: UPJ obstruction vs. obstructed megaureter (UVJ obstruction)
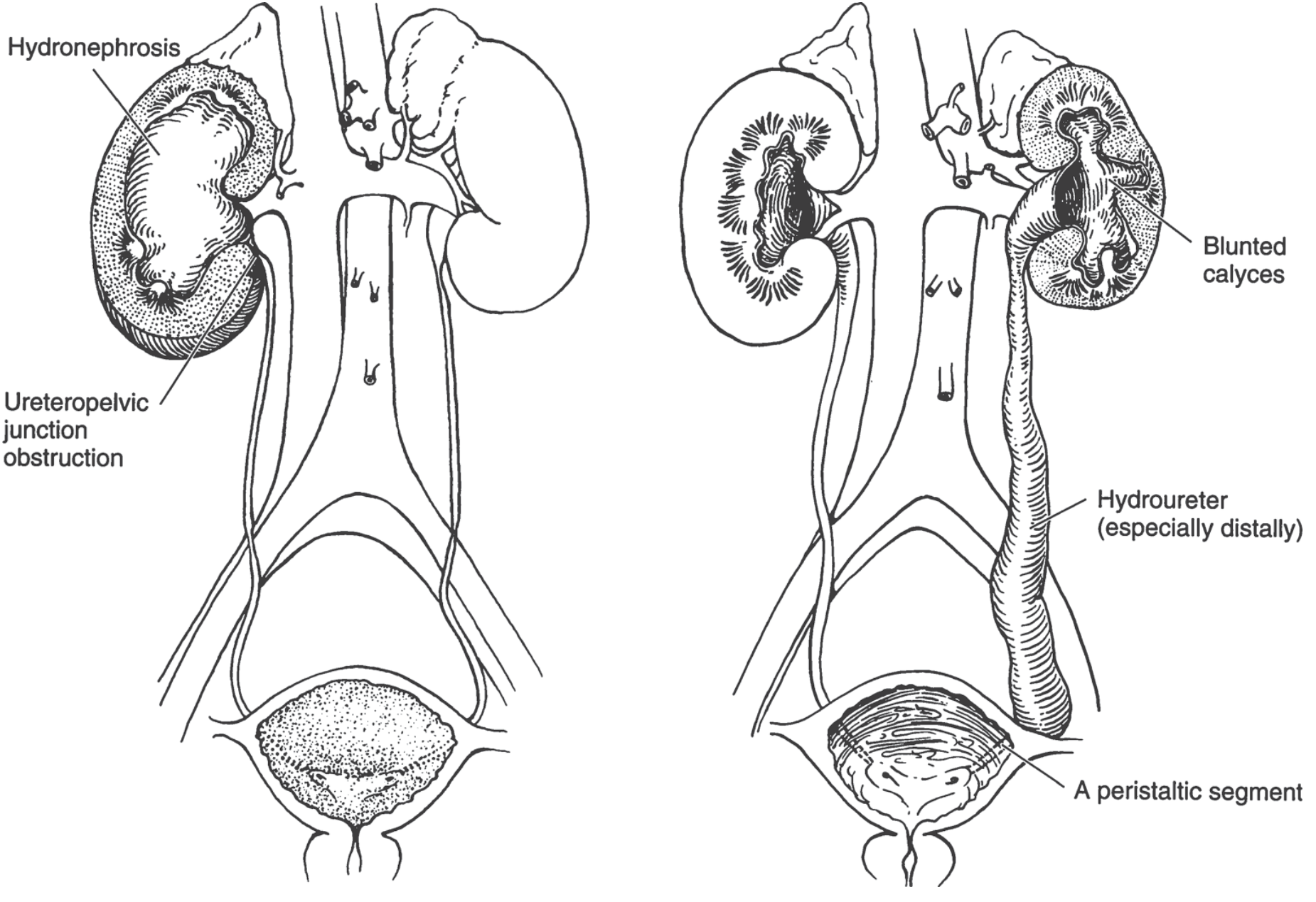
Left: Right UPJ obstruction → hydronephrosis only (ureter is normal). Right: Left UVJ obstruction (obstructed megaureter) → hydroureteronephrosis with blunted calyces and a dilated distal ureter.
Etiology of UPJ Obstruction
The cause is often unclear. Possible intrinsic mechanisms:
- Aperistaltic segment: thin-walled, hypoplastic proximal ureter with abnormal smooth muscle investment; characteristic histologic/ultrastructural changes impair peristalsis
- Overexpression of extracellular matrix and reduced nerve supply
- Decreased BMP4 signaling disrupting smooth muscle investment of the ureter
- True stenosis — rare
- High ureteral insertion into the renal pelvis
- Extrinsic: aberrant lower pole renal artery entrapping the proximal ureter (Stephens mechanism — abnormal renal rotation causes entrapment)
Most prenatally detected cases are intrinsic; many resolve spontaneously. Most adult cases are extrinsic, often in females.
— Smith and Tanagho's General Urology, 19th ed.; Campbell Walsh Wein Urology
5. Obstructed Megaureter (UVJ Obstruction)
When obstruction is at the ureterovesical junction, both the ureter and the pelvicalyceal system dilate — producing ureterohydronephrosis.
- 4× more common in boys than girls; may be bilateral (usually asymmetric); left side slightly more often affected
- Pathomechanism: In most cases there is NO anatomic stricture at the UVJ. Instead, a functional obstruction exists due to an aperistaltic distal ureteral segment with excess circular muscle fibers and collagen, causing failure of the peristaltic wave to propagate. Retrograde peristalsis is seen on fluoroscopy, transmitting abnormal pressures proximally
- Characteristic imaging: dilated distal ureter → less dilated proximal ureter → relatively normal renal pelvis → calyces blunted out of proportion to the pelvis
Most cases are now discovered on prenatal sonography.
— Smith and Tanagho's General Urology, 19th ed.
6. Pathogenesis of Obstruction-Induced Injury
Even with complete obstruction, glomerular filtration persists initially and filtered fluid diffuses back into the renal interstitium and perirenal spaces, eventually returning via lymphatics and veins. Because filtration continues, the renal pelvis and calyces become markedly dilated. The high intrapelvic pressure is transmitted retrograde through collecting ducts, compressing renal vasculature → arterial insufficiency + venous stasis.
- Initial injury is predominantly tubular (impaired concentrating ability), because papillae are subjected to the greatest pressure increases
- Later: glomerular filtration declines
- Obstruction also triggers interstitial inflammation → fibrosis
— Robbins & Kumar Basic Pathology
7. Morphology
Gross:
- Massively enlarged kidney (up to 20 cm) with greatly distended pelvicalyceal system
- Renal parenchyma compressed and atrophied; papillae obliterated; pyramids flattened
- With sudden complete obstruction: filtration ceases relatively early → dilation may be comparatively mild
- Depending on the level, one or both ureters may also be dilated (hydroureter)
Microscopy:
- Early: tubular dilation and atrophy
- Late: loss of glomeruli → replacement by fibrous tissue
- Minimal inflammatory reaction in uncomplicated cases
- Superimposed pyelonephritis is common
8. Grading of Hydronephrosis (Ultrasound)
On ultrasound, hydronephrosis appears as anechoic branching interconnected areas in the collecting system and is graded:
| Grade | Findings |
|---|---|
| Mild | Dilation of renal pelvis and calyces; parenchymal architecture retained |
| Moderate | Medullary pyramids begin to flatten; increasing pelvicalyceal dilation |
| Severe | Ballooned pelvis and calyces occupying most of the kidney; corticomedullary differentiation lost; parenchyma thin |
If the hydronephrotic area shows internal echoes, consider pyonephrosis (infected collecting system).
False negatives can occur with acute/partial obstruction, volume depletion, and retroperitoneal fibrosis.
— Comprehensive Clinical Nephrology, 7th Edition
9. Associated Anomalies
In congenital UPJ obstruction, urologic anomalies of the contralateral system are common, including:
- Renal agenesis
- Renal dysplasia / multicystic dysplastic kidney
- Vesicoureteral reflux
Approximately 10% of UPJ obstruction patients also have ipsilateral VUR (3× higher than the general pediatric population).
— Goldman-Cecil Medicine; Campbell Walsh Wein Urology
10. Clinical Features
| Setting | Features |
|---|---|
| Prenatal | Antenatal hydronephrosis on fetal ultrasound (most common presentation today) |
| Neonates | Palpable abdominal mass, UTI, hematuria, failure to thrive |
| Older children | Intermittent flank/abdominal pain + nausea/vomiting, worsened by brisk diuresis ("Dietl's crisis" — e.g., after caffeine or alcohol) |
| Adults | Palpable mass on routine examination; symptoms from the cause (calculi, tumor) |
| Bilateral obstruction | Anuria and renal failure; or paradoxically polyuria (incomplete bilateral obstruction → tubular concentrating defect) |
| Unilateral | May be silent for long periods |
11. Diagnosis
- Renal ultrasound: first-line; identifies hydronephrosis and its degree
- Diuretic renography (MAG3 scan): characterizes severity of obstruction; provides differential renal function
- Voiding cystourethrogram (VCUG): rules out VUR or bladder outlet obstruction
- Antegrade pyelography with pressure-flow (Whitaker test): for equivocal cases
- CT scan: may reveal cause (calculi, crossing vessel, mass) and extent of dilation
12. Management
UPJ Obstruction:
- Observation: Many prenatally detected cases with mild hydronephrosis resolve spontaneously
- Surgical pyeloplasty (Anderson-Hynes dismembered pyeloplasty) is indicated when:
- Obstructive excretory curve on diuretic renography
- Loss of ipsilateral renal function on renography
- Progressive hydronephrosis on serial ultrasound
- Symptomatic patients (pain, recurrent UTI, stones)
- Endopyelotomy (percutaneous or ureteroscopic): ~80% success; now reserved primarily for failed initial repair or concurrent stones
- Robotic/laparoscopic pyeloplasty: now the preferred minimally invasive approach; cosmetic advantage, similar morbidity
Obstructed Megaureter (UVJ obstruction):
- Many cases diagnosed prenatally resolve spontaneously
- Ureteral reimplantation with excision of the distal aperistaltic segment; ureteral tapering or folding if markedly dilated
- Prognosis is excellent because the ureteral muscle proximal to the aperistaltic segment is generally healthy
Prognosis: Removal of obstruction usually permits full return of function within a few weeks; however, with longstanding obstruction, changes become irreversible.
— Smith and Tanagho's General Urology, 19th ed.; Robbins & Kumar Basic Pathology; Campbell Walsh Wein Urology
Congenital anomalies of the kidney I need proper explanation of both with different in treatment and diagnosis Hydronephrosis.and Ureterohydronephrosis
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching Images
hydronephrosis vs ureterohydronephrosis diagram UPJ UVJ obstruction kidney ureter
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive data from multiple authoritative sources. Here is the complete, well-structured comparison.
Congenital Anomalies of the Kidney: Hydronephrosis vs. Ureterohydronephrosis
PART I — HYDRONEPHROSIS
Definition
Hydronephrosis is dilation of the renal pelvis and calyces with accompanying atrophy of the renal parenchyma, caused by obstruction to the outflow of urine. The obstruction may be sudden or insidious, and the ureter is NOT dilated — the obstruction lies at or above the ureteropelvic junction (UPJ).
"Hydronephrosis is dilation of the renal pelvis and calyces, with accompanying atrophy of the parenchyma, caused by obstruction to the outflow of urine." — Robbins & Kumar Basic Pathology
Gross Pathology
FIG. 12.25 — Hydronephrosis of the kidney with marked dilation of the pelvis and calyces and thinning of the renal parenchyma. — Robbins & Kumar Basic Pathology
The Most Important Congenital Cause: UPJ Obstruction
Ureteropelvic Junction (UPJ) Obstruction is the most common congenital cause of hydronephrosis, accounting for up to 30% of all prenatal urinary tract dilations. It is the most common congenital ureteral obstruction overall.
- More common in boys (male:female = 5:2)
- More often affects the left kidney
- Bilateral involvement in 10–40% of cases
Diagram — Key Distinction
Figure 37-9. Congenital ureteral obstruction. Left: UPJ obstruction → hydronephrosis (ureter normal). Right: UVJ obstruction (obstructed megaureter) → ureterohydronephrosis with hydroureter (especially distally) and blunted calyces. — Smith and Tanagho's General Urology, 19th Edition
Congenital Causes of Hydronephrosis (at or above UPJ)
| Congenital Cause | Mechanism |
|---|---|
| UPJ intrinsic stenosis | Aperistaltic, fibrotic, hypoplastic proximal ureter segment |
| Aberrant lower pole renal artery | Extrinsic compression/entrapment of the UPJ |
| High ureteral insertion | Ureter arises from a non-dependent position on the pelvis |
| Abnormal renal rotation | Causes ureteral kinking |
| Ureteral polyps/valves | Rare intrinsic obstructing lesions |
— Smith and Tanagho's General Urology, 19th ed.; Robbins & Kumar Basic Pathology
Pathogenesis
Even with complete obstruction, glomerular filtration persists for some time. The filtrate diffuses into renal interstitium and perirenal spaces, eventually returning via lymphatics and veins. Because filtration continues:
- Pelvis and calyces become markedly dilated
- High intrapelvic pressure is transmitted retrograde through collecting ducts
- Renal vasculature is compressed → arterial insufficiency + venous stasis
- Papillae are most vulnerable (greatest pressure) → initial tubular injury (impaired concentrating ability)
- Later: glomerular filtration declines
- Chronic obstruction → interstitial inflammation → fibrosis
— Robbins & Kumar Basic Pathology
Morphology
Gross:
- Massively enlarged kidney (up to 20 cm)
- Greatly distended pelvicalyceal system
- Parenchyma compressed, atrophied
- Papillae obliterated; pyramids flattened
- Ureter: normal caliber (this is the key distinguishing feature)
Microscopy:
- Early: tubular dilation and atrophy
- Late: glomerular loss → replaced by fibrous tissue
- Minimal inflammation in uncomplicated cases
- Superimposed pyelonephritis is common
Clinical Features — Hydronephrosis (UPJ Obstruction)
| Age Group | Presentation |
|---|---|
| Prenatal | Antenatal ultrasound — dilated renal pelvis without ureteral dilation |
| Neonates | Palpable flank/abdominal mass; UTI; hematuria; failure to thrive |
| Older children | Intermittent flank or abdominal pain + nausea/vomiting, worsened by brisk diuresis ("Dietl's crisis" — e.g. after caffeine/alcohol) |
| Adults | Palpable mass discovered incidentally; symptoms from complications (calculi, infection) |
| Unilateral | May remain silent for long periods |
| Bilateral | Anuria and renal failure; or paradoxical polyuria (incomplete bilateral obstruction → tubular concentrating defect masking the true diagnosis) |
Diagnosis of Hydronephrosis (UPJ Obstruction)
| Investigation | Findings | Purpose |
|---|---|---|
| Renal ultrasound (1st line) | Dilated pelvis + calyces; ureter NOT visualized/dilated; thinned parenchyma | Initial detection; monitoring |
| Diuretic renography (MAG3 scan) | Obstructive excretory curve; impaired drainage after furosemide; differential renal function | Confirms obstruction severity; quantifies renal function |
| VCUG (voiding cystourethrogram) | Rules out VUR (~10% co-exist with UPJ obstruction) | Indicated if hydroureter or recurrent UTI present |
| IVU / Retrograde pyelogram | Sharp cutoff at UPJ; normal ureter below; ballooned pelvis above | Anatomical localization of obstruction |
| CT urography | Shows crossing vessel, calculi, or other extrinsic cause | When cause is unclear |
| MR urography | Excellent functional + anatomic detail without radiation | Increasingly used especially in children (requires anesthesia) |
| Whitaker test (pressure-flow) | Antegrade perfusion; elevated pressure confirms true obstruction | Reserved for equivocal cases |
Key ultrasound hallmark: Dilated pelvicalyceal system with a NORMAL ureter.
Treatment of Hydronephrosis (UPJ Obstruction)
Conservative (Observation)
Indicated for mild–moderate asymptomatic hydronephrosis with preserved renal function, since many prenatally detected cases resolve spontaneously. Serial ultrasound monitoring is performed. Up to 25% may ultimately require intervention.
Surgical: Pyeloplasty (Definitive Treatment)
Indications for surgery:
- Obstructive excretory curve on diuretic renography
- Loss of differential renal function on renography
- Progressive hydronephrosis on serial ultrasound
- Symptomatic patients (pain, recurrent UTI, stones)
- Massive hydronephrosis or impaired renal function at diagnosis
Procedure — Dismembered Pyeloureteroplasty (Anderson-Hynes):
The obstructed/aperistaltic proximal ureteral segment is excised; the ureter is spatulated and re-anastomosed to the renal pelvis in a dependent, funnel-shaped configuration that allows gravity-assisted drainage. Success rate: >95%.
Other pyeloplasty variants:
- Foley Y-V plasty — when UPJ is in a dependent position but the pelvis is large and extrarenal
- Culp-De Weerd flap — pelvic flap procedures; preserve ureteral blood supply; suited for dependent UPJ with large pelvis
- Y-V plasty + Foley — for horseshoe/pelvic kidneys where anatomy prevents dependent anastomosis
Surgical Approaches:
- Open pyeloplasty (traditional gold standard)
- Laparoscopic pyeloplasty — equivalent outcomes, less morbidity
- Robotic-assisted pyeloplasty — now the preferred minimally invasive approach; cosmetically superior, widely adopted
Endopyelotomy (percutaneous or ureteroscopic): direct incision through the obstruction, stenting, healing by secondary intention; success rate ~80% — reserved for failed initial pyeloplasty or concurrent ureteral calculi.
Prophylactic antibiotic coverage is given perioperatively to prevent pyelonephritis.
"Removal of obstruction usually permits full return of function within a few weeks; however, with longstanding obstruction the changes become irreversible." — Robbins & Kumar Basic Pathology
PART II — URETEROHYDRONEPHROSIS (HYDROURETERONEPHROSIS)
Definition
Ureterohydronephrosis (also called hydroureteronephrosis) is the combined dilation of the ureter AND the renal pelvis/calyces, resulting from obstruction at or below the ureterovesical junction (UVJ). Unlike hydronephrosis, the entire upper urinary tract from calyx to distal ureter is dilated.
"Ureterovesical junction obstruction, also known as primary megaureter, is a physiologic obstruction at the ureterovesical junction, causing megaureter and hydronephrosis, in the absence of bladder dysfunction or reflux." — Creasy & Resnik's Maternal-Fetal Medicine
Key Congenital Causes — Ureterohydronephrosis
| Congenital Cause | Level | Comment |
|---|---|---|
| Obstructed megaureter (UVJ obstruction / primary megaureter) | UVJ | Most common congenital cause; aperistaltic distal ureteral segment |
| Posterior urethral valves (PUV) | Urethra | Bilateral; always check bladder and urethra |
| Urethral atresia | Urethra | Bilateral ureterohydronephrosis + massive bladder distension |
| Ureterocele | Intravesical | Upper pole ureterohydronephrosis in duplex kidney |
| Vesicoureteral reflux (VUR) | UVJ | Retrograde urine causes dilation; not true obstruction |
The Most Important Congenital Cause: Obstructed Megaureter (UVJ Obstruction)
- 4× more common in boys than girls
- May be bilateral (usually asymmetric); left ureter more often affected
- Also called primary megaureter when due to intrinsic UVJ abnormality
Pathomechanism
There is usually no anatomic stricture at the UVJ. A retrograde catheter can typically be passed through the area at operation. The obstruction is functional: an aperistaltic distal ureteral segment contains excess circular muscle fibers and collagen, preventing the normal peristaltic wave from propagating distally. On fluoroscopy, retrograde peristalsis is seen, transmitting abnormal pressures back up toward the kidney.
- Pathologically: excess circular muscle fibers + collagen in distal ureter → aperistalsis
- BMP4 signaling deficiency may contribute (as in UPJ obstruction)
Morphology
Gross:
- Markedly dilated distal ureter (most pronounced distally)
- Less dilated proximal ureter
- Relatively normal-appearing renal pelvis
- Calyces blunted out of proportion to the renal pelvis ← pathognomonic pattern
- Kidney parenchyma variably thinned depending on severity
Key distinguishing gross feature: In UPJ obstruction, the pelvis is massively dilated and the ureter is normal. In UVJ obstruction/megaureter, the distal ureter is most dilated and calyceal blunting is out of proportion to pelvic dilation.
Clinical Features — Ureterohydronephrosis (Obstructed Megaureter)
| Age Group | Presentation |
|---|---|
| Prenatal | Antenatal ultrasound — dilated ureter + renal pelvis; may see dilated distal ureter near bladder |
| Neonates | Palpable abdominal mass; febrile UTI (high infection risk — prophylactic antibiotics recommended 1–2 years) |
| Children | Recurrent UTI; flank pain; hematuria |
| Adults | Often discovered incidentally; may present with UTI, flank pain, or renal calculi |
| Bilateral disease | Anuria, renal failure, azotemia (e.g. PUV) |
Additional features of PUV specifically: bilateral ureterohydronephrosis + enlarged, trabeculated bladder; urinary stream abnormality in males; detectable on fetal ultrasound as early as 28 weeks.
Diagnosis of Ureterohydronephrosis
| Investigation | Findings | Purpose |
|---|---|---|
| Renal + bladder ultrasound (1st line) | Dilated ureter (especially distally) + dilated pelvis/calyces + normal or near-normal renal pelvis relative to calyceal blunting; sometimes dilated distal ureter behind bladder | Initial detection; differentiate from UPJ obstruction |
| VCUG (voiding cystourethrogram) | Mandatory — rules out VUR, posterior urethral valves, bladder dysfunction | Essential in ALL cases of ureterohydronephrosis |
| MAG3 diuretic renogram | Assesses differential renal function; obstructive washout curve | Functional assessment; guides surgical timing |
| IVU / Antegrade pyelogram | Classic appearance: dilated distal ureter, less dilated proximal ureter, blunted calyces | Anatomic confirmation; identifies site of narrowing |
| Fluoroscopy / retrograde ureterogram | Retrograde peristalsis visible; confirms functional aperistaltic segment | If diagnosis uncertain |
| Cystoscopy | Assess bladder; identify ureterocele; locate ureteral orifice | If VUR or ureterocele suspected |
Key ultrasound hallmark: Dilated distal ureter visible behind the bladder + dilated pelvis with blunted calyces out of proportion to pelvic dilation.
Critical difference from hydronephrosis: The ureter IS dilated in ureterohydronephrosis; VCUG is mandatory to exclude VUR and bladder outlet obstruction.
Treatment of Ureterohydronephrosis (Obstructed Megaureter / UVJ Obstruction)
Conservative (Observation — First-line in most)
The majority of prenatally detected moderate megaureters resolve spontaneously with observation — this is the most important management shift in recent decades.
- Serial ultrasound monitoring
- Prophylactic antibiotics for 1–2 years in neonates (high infection risk)
- Observation is appropriate in all asymptomatic patients initially
Surgical: Ureteral Reimplantation (Definitive Treatment)
Indications for surgery:
- Recurrent febrile UTIs despite prophylaxis
- Progressive loss of renal function on renography
- Persistent severe hydroureteronephrosis with symptoms (pain, stones)
- Failure of spontaneous resolution after adequate observation period
Procedure:
- Excision of the distal aperistaltic ureteral segment (the functionally obstructing portion)
- Ureteral reimplantation into the bladder with an adequate submucosal tunnel (anti-reflux technique)
- Because of excessive ureteral dilation, ureteral tapering or folding may be necessary before reimplantation (to reduce the caliber to allow effective peristalsis and a proper tunnel)
- Excision + tapering/folding + reimplantation = curative; prognosis is excellent because the ureteral muscle proximal to the aperistaltic segment is healthy
Temporizing options (for very young patients or severe bilateral disease):
- Cutaneous ureterostomy — temporary diversion while awaiting definitive repair
For Posterior Urethral Valves (bilateral ureterohydronephrosis):
- Primary valve ablation (transurethral resection of valves) — addresses the root cause
- Bladder drainage (catheterization) as initial step
- Upper tract decompression if indicated
SIDE-BY-SIDE COMPARISON TABLE
| Feature | Hydronephrosis | Ureterohydronephrosis |
|---|---|---|
| Definition | Dilation of renal pelvis + calyces only | Dilation of renal pelvis + calyces + entire ureter |
| Obstruction site | At or above UPJ | At or below UVJ |
| Ureter | Normal caliber | Dilated (especially distally) |
| Most common congenital cause | UPJ obstruction | Obstructed megaureter (UVJ obstruction) |
| Sex predominance | Boys (5:2) | Boys (4:1) |
| Laterality | More often left; bilateral 10–40% | More often left; may be bilateral |
| Key gross morphology | Massively dilated pelvis; papillae obliterated; flattened pyramids | Dilated distal ureter > proximal ureter; blunted calyces out of proportion to pelvis |
| Pathomechanism | Intrinsic UPJ stenosis / extrinsic compression / aperistaltic segment | Aperistaltic distal ureteral segment (functional obstruction); excess collagen + circular muscle |
| Hallmark ultrasound finding | Dilated pelvis + calyces; ureter NOT seen dilated | Dilated distal ureter behind bladder + dilated pelvis + blunted calyces |
| Essential extra investigation | Diuretic renography (MAG3) | VCUG is mandatory (rule out VUR, PUV, bladder dysfunction) |
| Spontaneous resolution | Common with mild prenatal cases | Majority resolve spontaneously |
| Definitive surgery | Pyeloplasty (dismembered Anderson-Hynes) | Ureteral reimplantation ± tapering/folding of ureter |
| Surgical principle | Excise aperistaltic UPJ segment; create funnel-shaped dependent drainage | Excise aperistaltic distal ureter; reimplant with adequate submucosal tunnel |
| Success rate | >95% with pyeloplasty | Excellent (healthy ureteral muscle proximal to obstruction) |
| Approach options | Open / Laparoscopic / Robotic pyeloplasty | Open or laparoscopic reimplantation; cutaneous ureterostomy as bridge |
| Prophylactic antibiotics | Given peri-operatively | 1–2 years in neonates (high UTI risk) |
| Prognosis | Good if treated early; irreversible with longstanding obstruction | Excellent — majority resolve without surgery |
Sources: Robbins & Kumar Basic Pathology; Smith and Tanagho's General Urology, 19th Edition; Campbell Walsh Wein Urology; Mulholland and Greenfield's Surgery; Creasy & Resnik's Maternal-Fetal Medicine; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.