Congenital anomalies of the kidney: Hydronephrosis. Ureterohydronephrosis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of Hydronephrosis and Ureterohydronephrosis as congenital anomalies of the kidney, drawn from authoritative sources.
Hydronephrosis / Ureterohydronephrosis
Definition
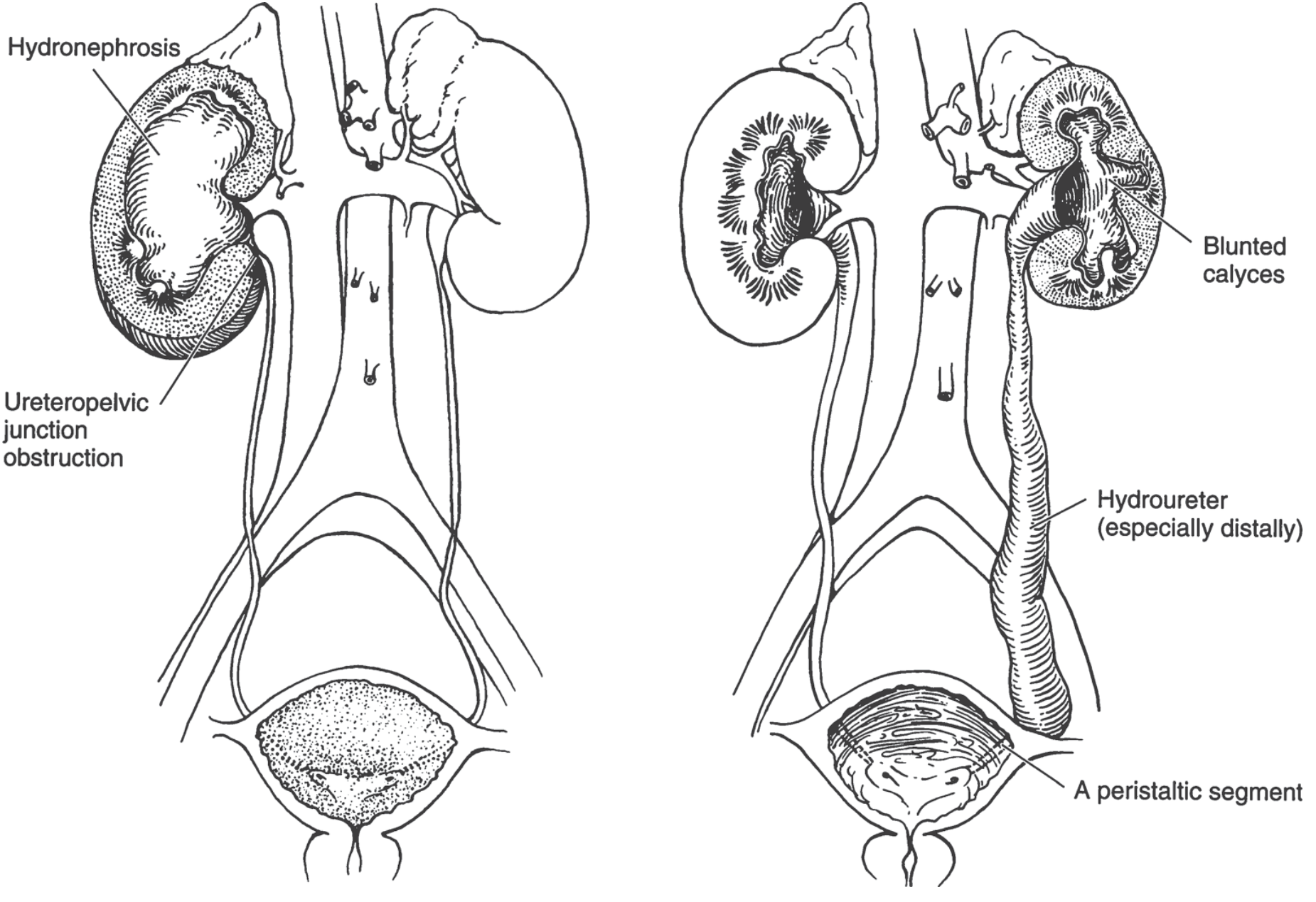
Hydronephrosis is dilation of the renal pelvis and calyces, with accompanying atrophy of the parenchyma, caused by obstruction to the outflow of urine. When the ureter is also dilated, the condition is termed ureterohydronephrosis (hydroureter + hydronephrosis). The obstruction may be sudden or insidious, and may occur at any level of the urinary tract — from the urethra to the renal pelvis.
Congenital Causes
The most clinically important congenital cause is ureteropelvic junction (UPJ) obstruction:
- UPJ obstruction is the most common cause of hydronephrosis in infants and children
- Incidence: approximately 1 in 500 live births screened by routine antenatal ultrasound
- More common in boys than girls when presenting early in life
- Bilateral in ~20% of early-presenting cases
- Agenesis of the contralateral kidney occurs in a minority of cases
- In adults, UPJ obstruction is more common in females and is most often unilateral
Mechanism of UPJ Obstruction
- Abnormal organization of smooth muscle bundles at the UPJ
- Excess stromal collagen deposition between smooth muscle bundles
- Rarely: extrinsic compression by aberrant renal vessels
Other congenital causes include:
| Cause | Description |
|---|---|
| Urethral atresia | Complete obstruction at the level of the urethra |
| Valve formations | Mucosal valves in the ureter or urethra |
| Aberrant renal artery | Compresses the ureter |
| Abnormal kidney position | Torsion or kinking of the ureter |
| Vesicoureteral reflux (VUR) | Reverse urine flow causing dilation |
| Posterior urethral valves (PUV) | Major cause of bilateral obstruction in boys |
Pathogenesis
Even with complete obstruction, glomerular filtration persists for some time. The filtrate diffuses back into the renal interstitium and perirenal spaces, returning to the lymphatic and venous systems. Because filtration continues, the affected calyces and pelvis become progressively dilated. The resulting elevated pressure is transmitted back through the collecting ducts and:
- Compresses the renal vasculature → arterial insufficiency and venous stasis
- Exerts maximum pressure on the papillae (most vulnerable site)
- Initial functional defect: impaired tubular concentrating ability
- Later: glomerular filtration begins to fall
- Interstitial inflammatory reaction → eventually fibrosis
Morphology (Gross and Microscopic)

Gross:
- Kidney may reach lengths of ~20 cm with subtotal or intermittent obstruction
- Organ consists almost entirely of the greatly distended pelvicalyceal system
- Renal parenchyma is compressed and atrophied
- Papillae are obliterated; pyramids are flattened
- If blockage is at or above the ureters: unilateral involvement
- If obstruction is below the ureters (e.g., bladder outlet): bilateral involvement
- With sudden complete obstruction: glomerular filtration fails early → renal function ceases with only mild dilation
Microscopic:
- Early: tubular dilation and atrophy
- Later: loss of glomeruli
- End-stage: replacement of renal parenchyma by fibrous tissue
- Inflammatory reaction is minimal in uncomplicated cases
- Superimposed pyelonephritis is common
Ultrasound Grading
On ultrasound, hydronephrosis appears as anechoic branching interconnected areas in the collecting system. Severity is graded qualitatively:
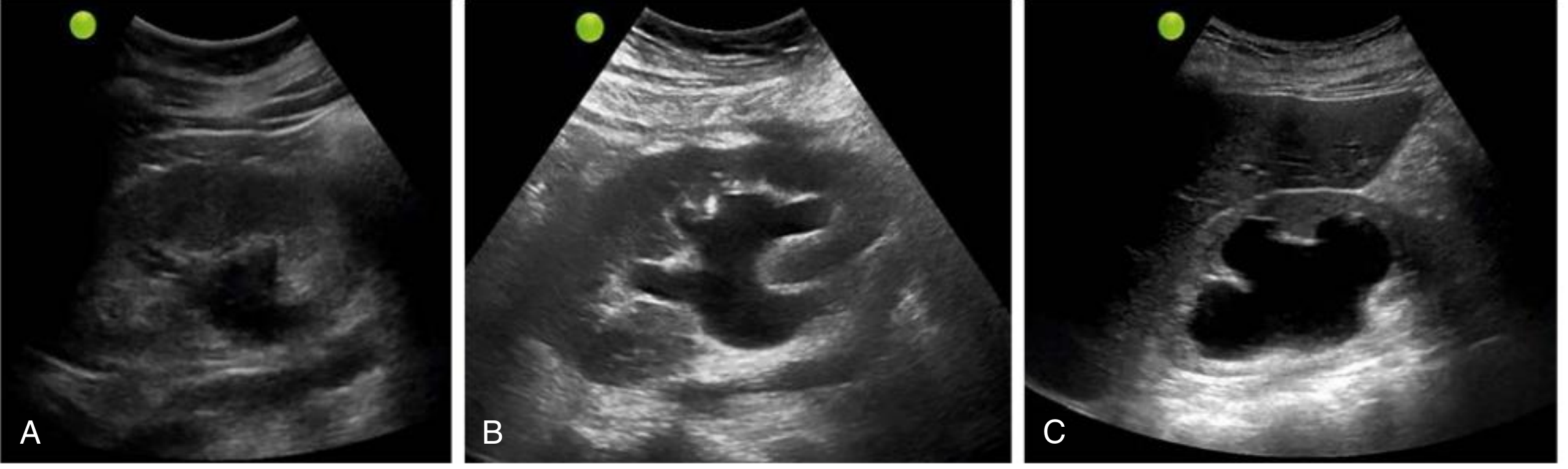
| Grade | Ultrasound Findings |
|---|---|
| Mild | Dilation of renal pelvis and calyces; overall parenchymal architecture retained |
| Moderate | Medullary pyramids begin to flatten; increasing pelvicalyceal dilation |
| Severe | Ballooned renal pelvis and calyces (occupying most of the kidney); corticomedullary differentiation lost; thin parenchyma |
Pitfalls: False negatives occur in acute/partial obstruction, volume depletion, and retroperitoneal fibrosis. Parapelvic cysts and prominent vasculature can mimic hydronephrosis — use color Doppler to differentiate vascular structures.
Clinical Features
- Bilateral hydronephrosis → anuria and renal failure
- Distal bladder obstruction → dominant symptoms are bladder distention
- Incomplete bilateral obstruction → paradoxically causes polyuria (due to tubular concentrating defect), which may obscure the diagnosis
- Unilateral hydronephrosis may remain clinically silent for long periods, especially if the contralateral kidney is functional — often discovered incidentally on physical exam or imaging
- Underlying causes (calculi, tumors) may produce symptoms that uncover the hydronephrosis
- Prognosis: removal of obstruction usually permits full functional recovery within weeks; however, longstanding obstruction produces irreversible changes
Fetal/Prenatal Hydronephrosis
- Increasingly detected prenatally by routine fetal ultrasonography
- A dilated collecting system may be the only indication of underlying congenital uropathy
- Two main mechanisms: VUR (reverse flow) or obstruction (impaired forward flow)
- Most common obstructive site: ureteropelvic junction
- Most cases are transient and resolve spontaneously
- Management protocol for confirmed fetal hydronephrosis:
- Postnatal renal ultrasound in first week of life
- If normal, repeat at 4 weeks and 1–2 years
- Urinalysis, urine culture, basic metabolic panel (if bilateral), VCUG (voiding cystourethrogram)
- If VCUG is normal → furosemide renography to assess obstruction degree
Ureteral Congenital Anomalies (Context)
Congenital ureteral anomalies are found in 2–3% of autopsies and include:
- Ureteral duplication
- Vesicoureteral reflux
- Double and bifid ureters
- Ureteropelvic junction obstruction (most clinically significant)
- Ureteral diverticula
Most have limited clinical significance, but those causing obstruction lead to ureterohydronephrosis and pyelonephritis.
Sources:
- Robbins & Kumar Basic Pathology — pp. 529–531
- Robbins, Cotran & Kumar Pathologic Basis of Disease — Congenital Anomalies, Ureters
- Comprehensive Clinical Nephrology, 7th Ed. — p. 81
- Textbook of Family Medicine, 9th Ed. — p. 1189
- Grainger & Allison's Diagnostic Radiology
Congenital anomalies of the kidney: HydronephrosisUreterohydronephrosis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive, textbook-sourced overview of Hydronephrosis and Ureterohydronephrosis as congenital anomalies of the kidney.
Hydronephrosis & Ureterohydronephrosis
Congenital Anomalies of the Kidney and Urinary Tract
1. Definitions
- Hydronephrosis — dilation of the renal pelvis and calyces with accompanying progressive atrophy of the kidney parenchyma, caused by obstruction to the outflow of urine
- Ureterohydronephrosis (Hydroureteronephrosis) — combined dilation of the ureter (hydroureter) and the renal pelvis/calyces; results when obstruction lies at the ureterovesical junction (UVJ) or below, rather than at the UPJ
Obstruction may be sudden or insidious, partial or complete, unilateral or bilateral, and can occur at any level of the urinary tract from the urethra to the renal pelvis.
2. Causes of Obstruction
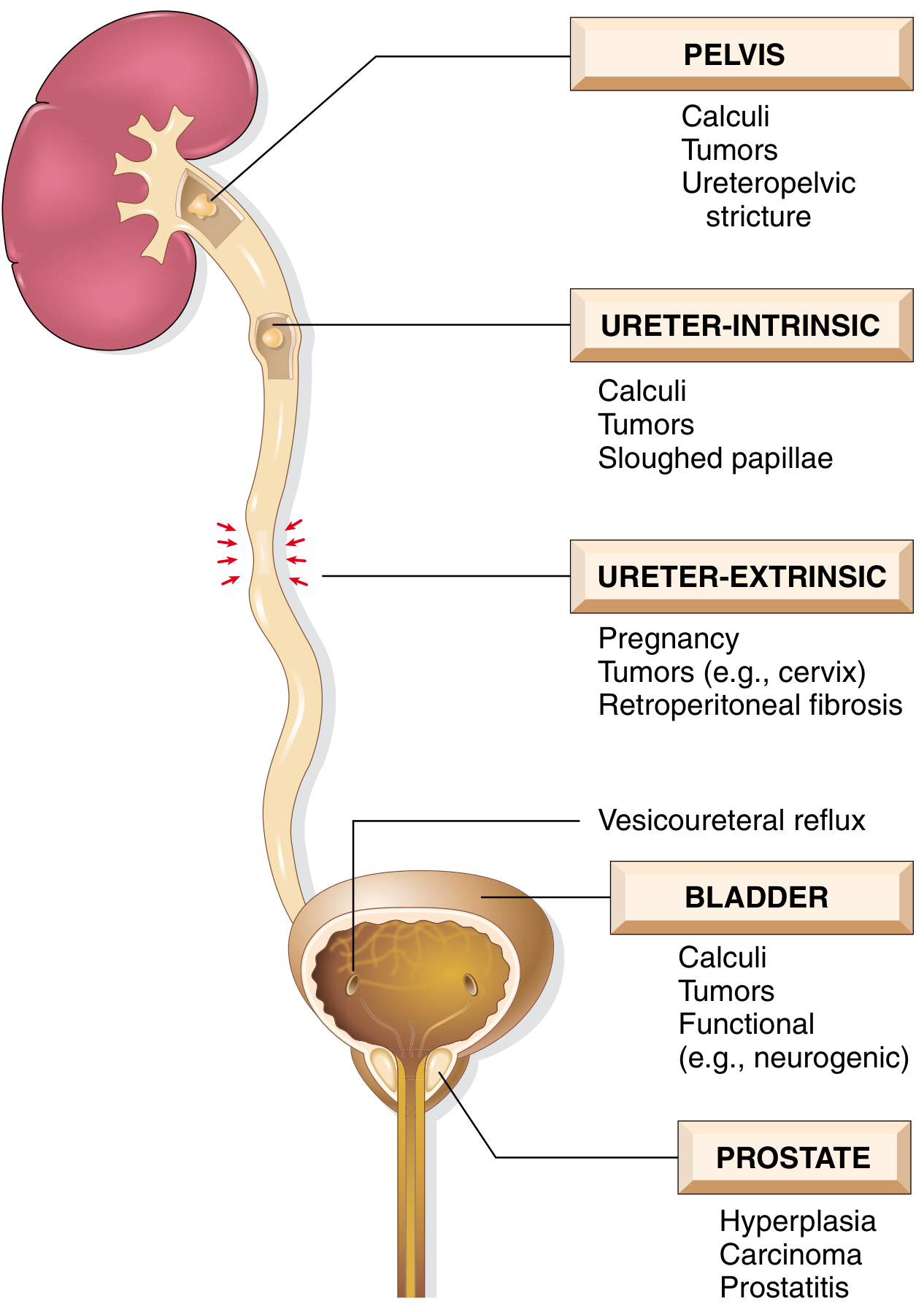
Congenital Causes (most relevant here)
| Anomaly | Notes |
|---|---|
| Ureteropelvic junction (UPJ) obstruction | Most common cause of hydronephrosis in infants and children; ~1 in 500 live births |
| Posterior urethral valves (PUV) | Major cause of bilateral ureterohydronephrosis in boys |
| Urethral atresia / meatal stenosis | Complete or near-complete outflow obstruction |
| Bladder neck obstruction | Causes bilateral hydronephrosis |
| Ureteral valve formations | Rare intrinsic ureteral obstruction |
| Aberrant renal artery compressing the ureter | Extrinsic UPJ obstruction |
| Abnormal kidney position — torsion/kinking of the ureter | |
| Severe vesicoureteral reflux (VUR) | Reverse-flow dilation; associated with complicated uropathies |
| High insertion of ureter into the renal pelvis | Promotes functional obstruction |
Acquired Causes (for comparison)
- Calculi, sloughed necrotic papillae
- Benign prostatic hyperplasia, carcinoma of the prostate
- Bladder tumors, retroperitoneal lymphoma, cervical/uterine carcinoma
- Retroperitoneal fibrosis
- Neurogenic bladder (spinal cord damage)
- Pregnancy (mild, physiologic)
3. UPJ Obstruction — The Dominant Congenital Form
Epidemiology:
- Incidence ~1 in 500 live births on routine antenatal ultrasound
- Preferentially affects males when presenting early in life
- Bilateral in ~20% of early-presenting cases
- Contralateral renal agenesis in a minority
- In adults, more common in females, usually unilateral
Pathologic mechanisms:
- Abnormal organization of smooth muscle bundles at the UPJ
- Excess stromal collagen deposition between smooth muscle bundles → impaired peristalsis
- Thin-walled or hypoplastic proximal ureter segment
- Kinking/angulation at the junction of dilated pelvis and ureter
- Extrinsic compression by a lower pole renal artery (particularly in horseshoe kidney)
- Decreased BMP4 signaling → disruption of smooth muscle investment of the ureter
- Overexpression of extracellular matrix + depleted nerve supply
4. Pathogenesis of Renal Damage
Even with complete obstruction, glomerular filtration persists initially. The filtrate diffuses back into renal interstitium and perirenal spaces, returning to lymphatic and venous systems. Ongoing filtration progressively distends the collecting system, and elevated intrapelvic pressure is transmitted back through the collecting ducts, with the following effects:
- Compresses renal vasculature → arterial insufficiency + venous stasis; medullary inner blood flow is diminished
- Maximum pressure at the papillae → papillary necrosis is the earliest structural lesion
- Initial tubular dysfunction → impaired urinary concentrating ability (earliest functional sign)
- Later: GFR begins to fall
- Interstitial inflammatory reaction → progressive interstitial fibrosis
5. Morphology
Gross Pathology
| Type of Obstruction | Gross Appearance |
|---|---|
| Subtotal / intermittent | Kidney massively enlarged (up to 20 cm); organ is almost entirely distended pelvicalyceal system; parenchyma compressed and atrophied; papillae obliterated; pyramids flattened |
| Sudden complete | GFR is compromised early; renal function ceases while dilation remains mild |
| Advanced chronic | Kidney transformed into a thin-walled cystic structure, diameter up to 15–20 cm; total obliteration of pyramids; extreme cortical thinning |
- In ureterohydronephrosis: one or both ureters are also dilated (hydroureter), depending on the level of obstruction
- Bilateral hydronephrosis: obstruction must be below the level of the ureters (e.g., bladder neck, urethra, PUV)
- Unilateral: obstruction at or above the ureter
Microscopy
| Stage | Microscopic Findings |
|---|---|
| Early | Tubular dilation and atrophy; interstitial inflammation (even without infection) |
| Progressive | Loss of glomeruli; diffuse interstitial fibrosis; blunting of pyramidal apices (cupping) |
| Late | Replacement of parenchyma by fibrous tissue; cortical tubular atrophy |
| Complication | Superimposed pyelonephritis is common |
6. Clinical Features
Symptoms by Pattern of Obstruction
| Scenario | Manifestation |
|---|---|
| Unilateral (partial or complete) | May remain silent for long periods; contralateral kidney compensates; often discovered incidentally on imaging or physical exam |
| Bilateral partial obstruction | Polyuria and nocturia (earliest sign — tubular concentrating defect); distal tubular acidosis, renal salt wasting, hypertension, secondary calculi, chronic tubulointerstitial nephritis |
| Bilateral complete obstruction | Oliguria or anuria; renal failure; post-relief diuresis (massive, NaCl-rich) is characteristic |
| Obstruction distal to bladder | Bladder distention symptoms dominate |
| Acute obstruction | Pain from distention of collecting system or renal capsule; renal colic if calculus |
Prenatal / Fetal Hydronephrosis
- Increasingly diagnosed on routine fetal ultrasonography (dilated collecting system may be the only sign)
- Two mechanisms: VUR (reverse flow) or obstruction (impaired forward flow)
- Most common site: ureteropelvic junction
- Majority are transient and resolve spontaneously
- UPJ cases tend to be intrinsic; many resolve without surgery
- Massive hydronephrosis, diminished renal function, infection, or stones → early surgical intervention recommended
7. Diagnosis
| Method | Role |
|---|---|
| Renal ultrasound | First-line, noninvasive; grades severity (mild/moderate/severe); detects hydroureter |
| VCUG (voiding cystourethrogram) | Evaluates VUR and bladder outlet obstruction |
| Diuretic renography (MAG3 or DTPA + furosemide) | Assesses differential renal function and degree of functional obstruction |
| CT urography / IVU | Defines anatomy; localizes obstruction level |
| Antegrade urography + pressure-flow studies (Whitaker test) | Reserved for equivocal cases |
Postnatal surveillance protocol for prenatally detected hydronephrosis:
- Renal ultrasound in first week of life
- If normal, repeat at 4 weeks and 1–2 years
- Urinalysis, urine culture, basic metabolic panel (if bilateral), VCUG
- If VCUG normal → furosemide renography to quantify obstruction
8. Treatment
- Relief of obstruction — within the first weeks, allows full recovery of renal function
- Longstanding obstruction → irreversible changes; prognosis for recovery is poor
- UPJ obstruction (symptomatic) → surgical repair (pyeloplasty):
- Dismembered pyeloureteroplasty (Anderson-Hynes) — most popular; mandatory when obstruction is caused by a dyskinetic proximal ureteral segment or when ureter hooks over a lower pole vessel
- Foley Y-V plasty — used when there is a dilated extrarenal pelvis
- Culp-De Weerd pelvic flap — suited when UPJ remains dependent despite pelvic dilation; preserves ureteral blood supply
- Asymptomatic / mild congenital hydronephrosis: nonoperative surveillance is safe; ~25% ultimately require surgery for pain, UTI, or reduced function on nuclear scan
- Post-obstruction diuresis after relief of complete bilateral obstruction — may be massive; requires careful fluid and electrolyte management
Sources:
- Robbins & Kumar Basic Pathology — pp. 529–531
- Robbins, Cotran & Kumar Pathologic Basis of Disease — pp. 876–878
- Smith and Tanagho's General Urology, 19th Ed. — pp. 589–591
- Textbook of Family Medicine, 9th Ed. — p. 1189
- Grainger & Allison's Diagnostic Radiology
- Comprehensive Clinical Nephrology, 7th Ed. — p. 81
This is a shared conversation. Sign in to Orris to start your own chat.