I’m a orthopaedics resident in 1st year teach me basics of it
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I have rich, comprehensive foundational content from Miller's Review of Orthopaedics. Now let me compile a thorough, well-organized answer for a 1st-year orthopaedics resident.
Orthopaedics Basics for the 1st Year Resident
Welcome to orthopaedics! Here is a structured primer covering the foundational science you need as a base for everything else you will learn.
Source: Miller's Review of Orthopaedics, 9th Edition
1. BONE - The Core Tissue
Types of Bone
Microscopic classification:
| Type | Characteristics | Clinical Example |
|---|---|---|
| Lamellar | Normal bone; stress-oriented; organized; stronger | Femoral shaft (cortical), distal femur (cancellous) |
| Woven | Immature/pathologic; random organization; high turnover; weaker | Fracture callus, embryonic skeleton, osteosarcoma |
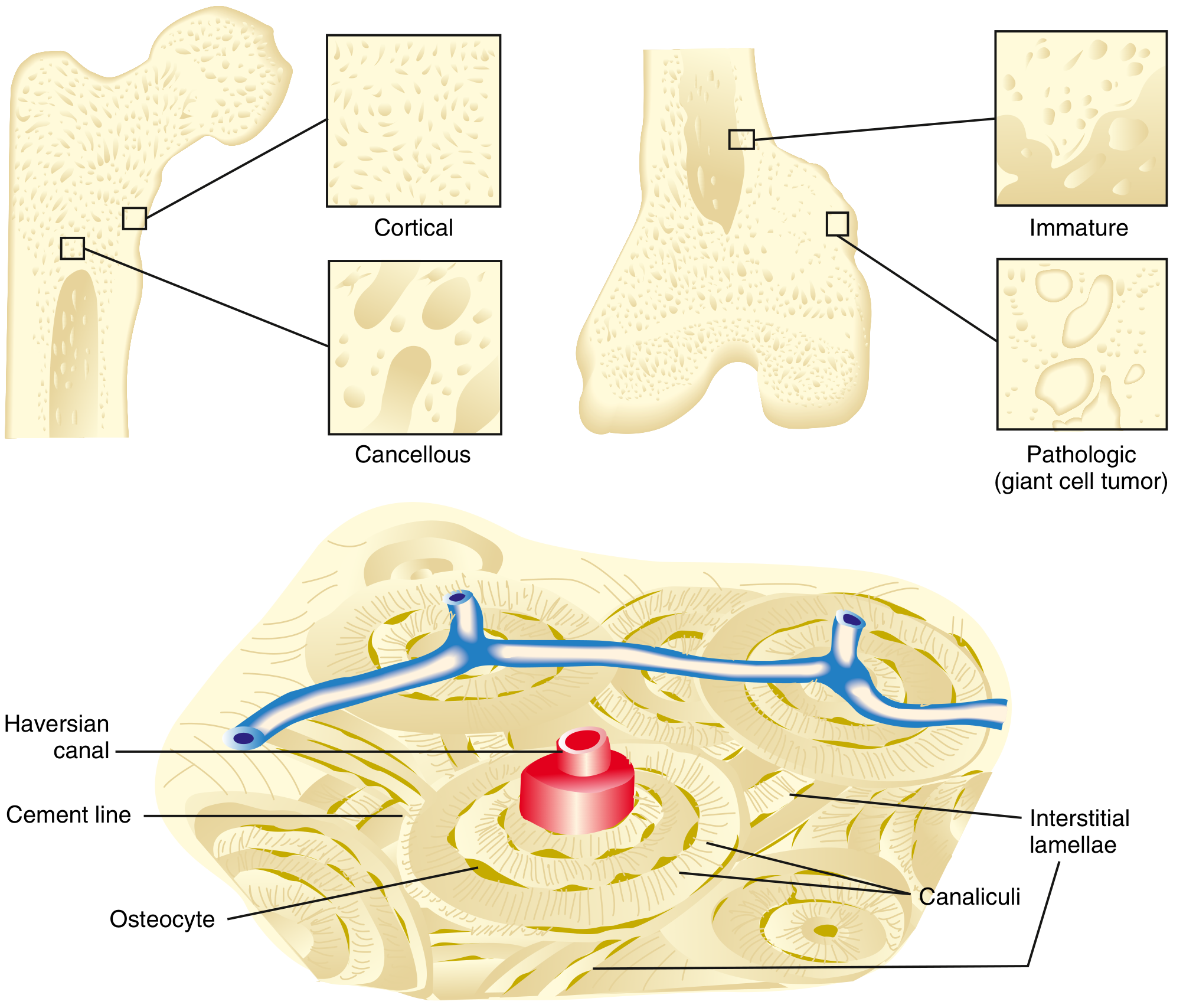
Macroscopic classification:
-
Cortical (compact) bone - 80% of skeleton
- Slow turnover; high Young's modulus; stiff
- Made of tightly packed osteons (Haversian systems)
- Haversian canals (longitudinal) connect to Volkmann canals (transverse)
- Cement lines = outer border of each osteon
- Nutrition via intraosseous circulation through canaliculi (osteocyte cell processes)
-
Cancellous (trabecular/spongy) bone - 20% of skeleton
- High surface area; faster turnover; more elastic than cortical
- Found at metaphyses and epiphyses
Bone Cells (the "BLAST-CLAST" concept)
| Cell | Origin | Function |
|---|---|---|
| Osteoblast | Mesenchymal stem cell | Bone formation; produces type I collagen + osteoid |
| Osteocyte | Mature osteoblast embedded in matrix | Mechanosensing; regulates remodeling via lacunocanalicular network |
| Osteoclast | Hematopoietic monocyte lineage | Bone resorption; ruffled border secretes acid + proteases |
Key concept - RANKL/OPG axis:
- RANKL (on osteoblasts) activates osteoclasts
- OPG (osteoprotegerin, from osteoblasts) decoys RANKL and inhibits osteoclastogenesis
- This balance is targeted by denosumab (anti-RANKL antibody used in osteoporosis/bone mets)
2. FRACTURE BIOLOGY - What Happens When Bone Breaks
The 3 Phases of Fracture Healing
Phase 1 - Inflammation (days 1-7)
- Fracture hematoma forms; hematopoietic cells release growth factors (BMP, TGF-β, PDGF, FGF)
- Fibroblasts, mesenchymal cells, and osteoprogenitor cells recruited
- Granulation tissue forms around fracture ends
Phase 2 - Repair (weeks 2-6)
- Primary callus response within 2 weeks
- Bridging (soft) callus forms at bone ends not in continuity - via endochondral ossification (cartilage replaced by woven bone = "hard callus")
- Medullary callus forms later
- Type II collagen expressed early (unstable fractures) → followed by type I collagen
Phase 3 - Remodeling (months to years)
- Begins mid-repair phase, continues up to 7 years
- Woven bone replaced by lamellar bone
- Guided by Wolff's Law - bone remodels along lines of mechanical stress
- Piezoelectric charges from bone deformation also guide remodeling
- Complete when marrow space is repopulated
Fracture Healing by Treatment Method
| Stabilization | Healing Type |
|---|---|
| Cast (closed) | Periosteal bridging callus + endochondral ossification |
| Compression plate | Primary cortical healing (cutting-cone/Haversian remodeling) |
| Intramedullary nail | Early: periosteal bridging callus; Late: medullary callus |
| Inadequate immobilization + good blood supply | Hypertrophic nonunion |
| Inadequate immobilization + poor blood supply | Atrophic nonunion |
Key rule: Amount of callus is inversely proportional to extent of immobilization. Rigid fixation = less callus (primary healing). Flexible fixation = more callus (secondary healing).
Factors That Impair Fracture Healing
- Nicotine/smoking - increases time to healing, increases nonunion risk (up to 500% increase in lumbar pseudarthrosis), weakens callus
- NSAIDs - inhibit COX → impair prostaglandin-mediated bone healing
- Steroids - inhibit osteoblasts
- Poor nutrition, diabetes, peripheral vascular disease, radiation
Key Growth Factors
| Growth Factor | Role |
|---|---|
| BMP (Bone Morphogenetic Protein) | Osteoinductive; converts mesenchymal cells into osteoblasts via SMAD signaling |
| TGF-β | Induces type II collagen and proteoglycans; stimulates osteoblast collagen synthesis |
| PDGF | Chemotactic; stimulates fibroblast proliferation early |
| FGF | Angiogenesis; fibroblast proliferation |
| IGF-1 | Stimulates osteoblast activity and matrix synthesis |
3. ARTICULAR CARTILAGE - The Joint Surface
Key properties:
- Avascular, aneural, alymphatic - nutrients come from synovial fluid and subchondral bone by diffusion
- Coefficient of friction < ice on ice (0.002-0.04 in a healthy joint)
- Withstands impact loads up to 25 N/mm²
- Viscoelastic - properties change with rate of force application
- Anisotropic - properties vary with direction of force
- Heals poorly - this is why articular damage is so significant clinically
Composition of Hyaline Cartilage
| Component | Amount | Notes |
|---|---|---|
| Water | ~75% | Highest at superficial zone (80%); decreases with aging; increases in OA |
| Type II collagen | ~15% dry weight (90-95% of cartilage collagen) | Triple helix from COL2A1 gene; defects cause SED, achondrogenesis |
| Proteoglycans | ~10% dry weight | Aggrecan (main), lubricin (surface friction) |
| Chondrocytes | <5% | Only cells; maintain ECM; no regenerative capacity after damage |
Cartilage Layers (Zones)
- Superficial zone - collagen fibers parallel to surface; highest water content; most cells
- Middle (transitional) zone - oblique collagen; larger cells
- Deep zone - collagen perpendicular to surface; lowest water content; largest proteoglycans
- Calcified zone - separated from deep zone by tidemark; type X collagen; anchors to subchondral bone
4. MUSCLE - The Motor
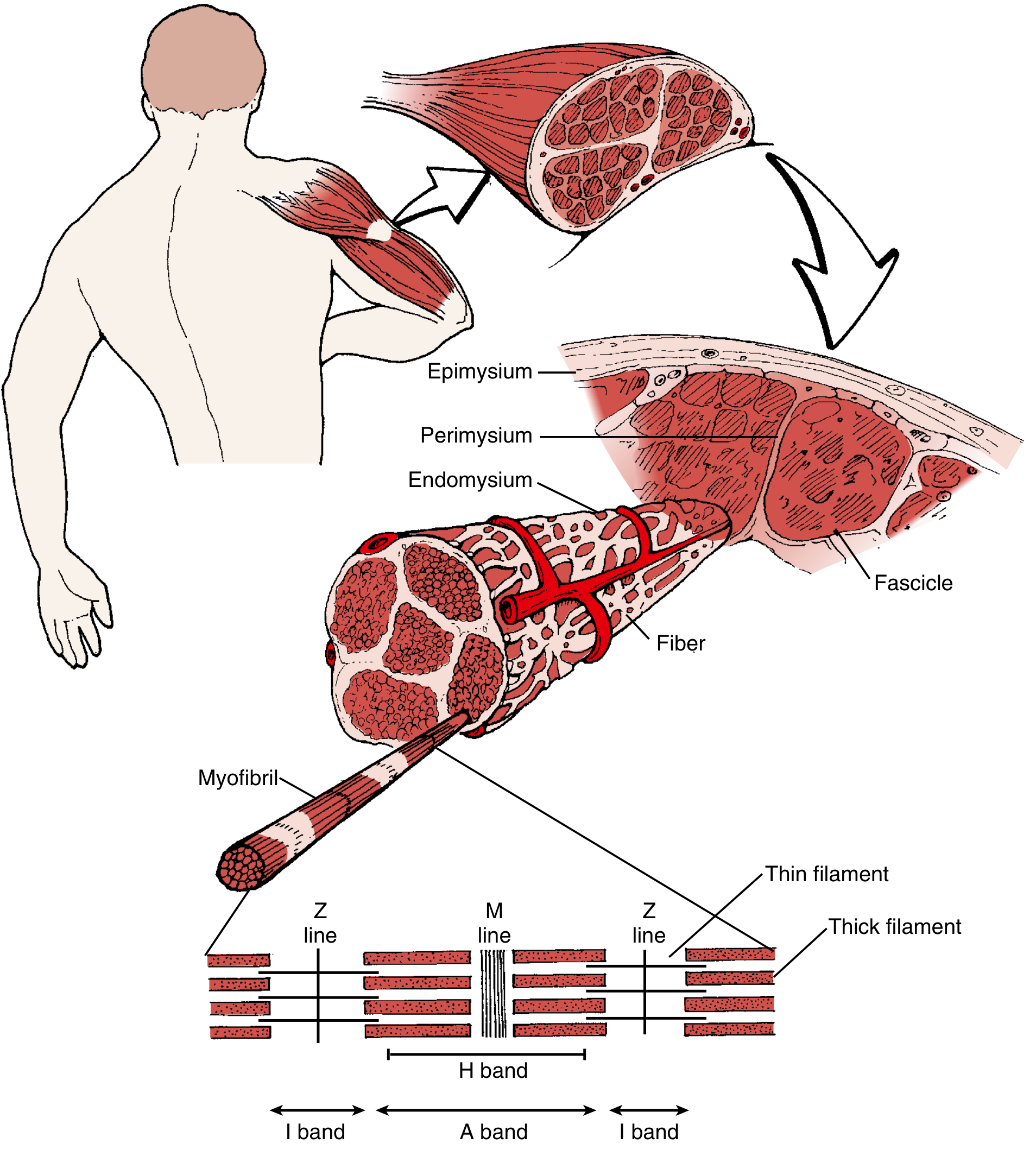
Structural Hierarchy (outside to inside)
Muscle → Epimysium → Fascicles (surrounded by Perimysium) → Fibers → Endomysium → Myofibrils → Sarcomeres
The Sarcomere (basic contractile unit)
- A-band (dark) = thick filaments (myosin) - does NOT shorten during contraction
- I-band (light) = thin filaments (actin) - shortens during contraction
- H-band = myosin only (between two I-bands)
- Z-line = borders the sarcomere; contains desmin, α-actinin, filamin
- M-line = center of sarcomere
Sliding filament mechanism: Calcium released from sarcoplasmic reticulum → binds troponin → tropomyosin shifts → actin-myosin cross-bridge forms → ATP-driven power stroke → contraction
Muscle Fiber Types
| Type | Speed | Fatigue | Metabolism | Example |
|---|---|---|---|---|
| Type I (slow twitch) | Slow | Fatigue-resistant | Oxidative | Postural muscles (soleus) |
| Type II A | Fast | Intermediate | Oxidative + glycolytic | Mixed use muscles |
| Type II B/X | Fastest | Fatigues quickly | Glycolytic | Sprinting muscles |
Malignant hyperthermia - caused by abnormality of ryanodine receptors (RYR-1) → uncontrolled calcium release → hyperthermia, muscle rigidity. Treat with dantrolene (decreases Ca²⁺ release from SR).
5. TENDON & LIGAMENT
Tendon Composition
- Water: 50-60% total weight
- Type I collagen: 75% of dry weight (85% of the collagen fraction)
- Elastin: 1-2% - responsible for the "toe region" of the stress-strain curve
- Proteoglycans: up to 5% (decorin is the most predominant)
Tenocytes (fibroblasts): synthesize ECM, produce MMPs, detect strain via cell cilia
- In response to rupture: produce type III collagen (weaker → predisposes to re-rupture)
- Greater proportion of type III in Achilles tendon = explains high rupture rate
Structure: Hierarchy
Tropocollagen → Microfibrils → Fibrils → Fascicles (surrounded by endotendon) → Tendon (surrounded by epitendon/paratenon)
Tendon-Bone Insertion (Enthesis)
Four zones: tendon → uncalcified fibrocartilage → calcified fibrocartilage → bone
- Separated by a tidemark (same concept as cartilage)
- This gradual transition reduces stress concentration
6. THE STRESS-STRAIN CURVE - Biomechanics You Must Know
Every orthopaedic tissue has a stress-strain curve with:
- Toe region - collagen fibers uncrimping (elastin dominant)
- Linear (elastic) region - reversible deformation; follows Hooke's law
- Yield point - transition to plastic deformation
- Plastic region - irreversible deformation (microfractures)
- Failure point - complete rupture
Young's modulus (E) = stiffness = slope of linear region
- Cortical bone: high E (very stiff)
- Cancellous bone: lower E (more elastic)
- Cartilage: lowest E (most deformable)
7. NERVE INJURIES - Seddon & Sunderland Classification
| Seddon | Sunderland | What's Injured | Recovery |
|---|---|---|---|
| Neuropraxia | Grade I | Myelin only; axon intact | Complete, weeks-months |
| Axonotmesis | Grades II-IV | Axon disrupted; endoneurium intact (II), perineurium disrupted (III), epineurium intact (IV) | Possible; grows 1 mm/day |
| Neurotmesis | Grade V | Complete nerve division | Poor without surgery |
Nerve regrowth rate: ~1 mm/day or 1 inch/month - use this to predict recovery timelines clinically.
8. BONE METABOLISM - Key Hormones
| Hormone | Effect on Bone | Other Effects |
|---|---|---|
| PTH (excess/chronic) | Resorption (activates osteoclasts) | ↑ Ca²⁺, ↓ PO₄ in blood |
| PTH (pulsatile/low dose) | Anabolic (teriparatide mechanism) | Used in osteoporosis |
| Vitamin D | ↑ Ca²⁺ absorption (gut), ↑ mineralization | Deficiency → rickets/osteomalacia |
| Calcitonin (thyroid C-cells) | Inhibits osteoclasts; ↓ Ca²⁺ | Nasal calcitonin used in Paget's disease |
| Estrogen | Inhibits osteoclasts | Loss at menopause → osteoporosis |
| Cortisol (excess) | Inhibits osteoblasts; ↑ resorption | Steroid-induced osteoporosis |
9. QUICK CLINICAL PEARLS FOR DAILY WARD WORK
-
Compartment syndrome - 5 P's: Pain (worst, especially with passive stretch), Pressure, Pallor, Paresthesia, Paralysis. Treat with emergent fasciotomy when compartment pressure >30 mmHg or within 30 mmHg of diastolic BP.
-
Open fractures - Gustilo-Anderson classification (I, II, IIIA, IIIB, IIIC). IV antibiotics (cephalosporin ± aminoglycoside ± penicillin for soil contamination). Irrigation and debridement within hours.
-
Fat embolism syndrome - triad of respiratory failure, neurological dysfunction, petechial rash. Occurs 24-72 hrs post long bone/pelvic fracture.
-
Avascular necrosis (AVN) - most common after femoral neck fractures and hip dislocations. Hip dislocations must be reduced within 6 hours to minimize AVN risk.
-
Salter-Harris classification - for physeal (growth plate) fractures in children:
- Type I: through physis (Slipped)
- Type II: through physis + metaphysis (Above - most common, best prognosis)
- Type III: through physis + epiphysis (Lower)
- Type IV: through all three (Through)
- Type V: crush injury to physis (ERasure - worst prognosis)
- Mnemonic: SALTR (Slipped, Above, Lower, Through, Rammed/ERasure)
Where to Go From Here
Your foundational reading priorities in order:
- Miller's Review of Orthopaedics (9th Ed) - work through Section 1 (Basic Sciences) systematically
- Campbell's Operative Orthopaedics (15th Ed, 2026) - reference for surgical approaches and techniques
- Rockwood & Green's Fractures in Adults (10th Ed, 2025) - your fracture bible
The basic science you have learned above - bone biology, fracture healing, cartilage, muscle, tendons, biomechanics, and nerve injuries - underpins every clinical decision you will make. When you understand why a fracture fails to heal (smoking, instability, poor blood supply), you make better treatment choices.
- Miller's Review of Orthopaedics, 9th Ed, Section 1 (pp. 20-72)
This is a shared conversation. Sign in to Orris to start your own chat.