Congenital anomalies of the kidney: Hydronephrosis. Ureterohydronephrosis-PD-D
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Loading Image
I now have comprehensive pathological and clinical information from authoritative sources. Here is a complete structured answer:
Congenital Anomalies of the Kidney: Hydronephrosis / Ureterohydronephrosis
Definition
Hydronephrosis is dilation of the renal pelvis and calyces, with accompanying atrophy of the parenchyma, caused by obstruction to the outflow of urine. When the ureter is also dilated, the condition is called ureterohydronephrosis (hydroureteronephrosis). The obstruction may be sudden or insidious and can occur at any level of the urinary tract — from the urethra to the renal pelvis.
— Robbins & Kumar Basic Pathology, p. 529–530
Causes
Congenital (relevant to this topic)
- Atresia of the urethra
- Valve formations in the ureter or urethra
- Aberrant renal artery compressing the ureter
- Abnormal kidney position with torsion or kinking of the ureter
Acquired
| Category | Examples |
|---|---|
| Foreign bodies | Calculi, sloughed necrotic papillae |
| Proliferative lesions | Benign prostatic hyperplasia, carcinoma of the prostate, bladder tumors, retroperitoneal lymphoma, carcinoma of the cervix/uterus |
| Inflammatory | Prostatitis, ureteritis, urethritis, retroperitoneal fibrosis |
| Neurogenic | Bladder paralysis from spinal cord damage |
| Physiologic | Pregnancy (mild) |
Key anatomical rule: Bilateral hydronephrosis occurs only when obstruction is below the level of the ureters. Unilateral hydronephrosis = ureteral or above obstruction.
Pathogenesis
Even with complete obstruction, glomerular filtration persists for some time — filtrate diffuses back into the renal interstitium and perirenal spaces, returning via lymphatic and venous systems. This continued filtration causes progressive dilation of the calyces and pelvis.
The resulting elevated intrapelvic pressure transmits back through collecting ducts, compresses the renal vasculature → arterial insufficiency + venous stasis. The papillae suffer the most (greatest pressure increase).
Sequence of functional injury:
- Initial: Tubular impairment — especially impaired concentrating ability
- Later: Glomerular filtration decreases
- Chronic: Interstitial inflammatory reaction → interstitial fibrosis
— Robbins & Kumar Basic Pathology, p. 530
Morphology (Gross & Microscopic)
Gross Pathology
With subtotal or intermittent obstruction:
- Kidney massively enlarged (may reach 20 cm)
- Organ consists almost entirely of greatly distended pelvicalyceal system
- Renal parenchyma compressed and atrophied
- Papillae obliterated; pyramids flattened
- One or both ureters also dilated (hydroureter) depending on obstruction level
With sudden, complete obstruction:
- Glomerular filtration compromised early → renal function ceases while dilation is comparatively mild

Microscopic Pathology
- Early: Tubular dilation and atrophy
- Progressive: Loss of glomeruli
- Late: Replacement of renal parenchyma by fibrous tissue
- Inflammatory reaction minimal in uncomplicated cases
- Superimposed pyelonephritis is common
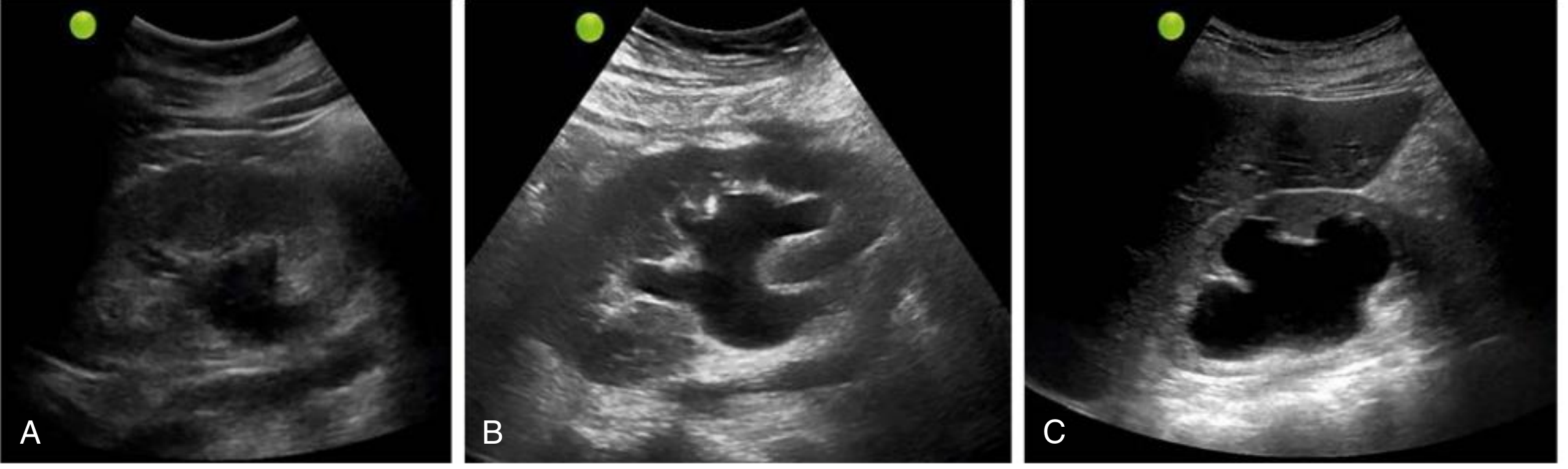
Ultrasound Grading (Diagnostic Imaging — PD)
On ultrasound, hydronephrosis appears as anechoic (black) branching, interconnected areas in the renal collecting system — backlogged urine amid the echogenic sinus fat.
| Grade | US Findings |
|---|---|
| Mild | Dilation of renal pelvis and calyces; overall parenchymal architecture retained |
| Moderate | Medullary pyramids begin to flatten due to back pressure; increasing pelvicalyceal dilation |
| Severe | Ballooned renal pelvis and calyces (occupying most of kidney); corticomedullary differentiation lost; parenchyma thin |
Important: If the hydronephrotic area shows internal echoes, consider pyonephrosis (pus in the collecting system), especially with fever and flank pain.
False negatives for hydronephrosis on ultrasound occur with:
- Acute or partial obstruction
- Volume depletion
- Retroperitoneal fibrosis
— Comprehensive Clinical Nephrology, 7th Edition, p. 81
Clinical Features
| Scenario | Presentation |
|---|---|
| Bilateral hydronephrosis | Anuria and renal failure |
| Obstruction distal to bladder | Bladder distension symptoms |
| Incomplete bilateral obstruction | Polyuria (paradoxical — due to tubular concentrating defect) — may obscure the diagnosis |
| Unilateral hydronephrosis | May remain silent for long periods; often found incidentally; may present due to underlying cause (calculi, tumor) |
Prognosis: Removal of obstruction usually permits full return of function within weeks. With longstanding obstruction, changes become irreversible.
Summary of Key Points
- Hydronephrosis = obstruction → back-pressure → pelvicalyceal dilation + parenchymal atrophy
- Congenital causes include urethral atresia, ureteral valves, aberrant vessels, and renal malposition
- Bilateral disease = obstruction below ureters; unilateral = ureteral or higher
- The papillae bear the greatest pressure injury
- Functional sequence: tubular dysfunction first → glomerular failure later
- Gross: massive renal enlargement with destroyed papillae; microscopic: tubular atrophy → fibrosis
- US is the first-line diagnostic tool; severity graded mild/moderate/severe by pelvicalyceal dilation and parenchymal thinning
This is a shared conversation. Sign in to Orris to start your own chat.