Congenital anomalies of the kidney: Hydronephrosis. Ureterohydronephrosis-PD-D Explain properly definition causes pathogenesis clinical manifestations diagnosis classification treatment differential diagnosis and ages and diffrence between male and female explain everything properly
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive, structured account of Hydronephrosis / Ureterohydronephrosis covering every dimension you asked about.
Hydronephrosis & Ureterohydronephrosis
Congenital Anomalies of the Kidney — Complete Review
1. Definition
Hydronephrosis is the dilation of the renal pelvis and calyces, with accompanying atrophy of the renal parenchyma, caused by obstruction to the outflow of urine. The obstruction may be sudden or insidious and can occur at any level of the urinary tract — from the urethra to the renal pelvis.
Ureterohydronephrosis (hydroureteronephrosis) is the combined dilation of the ureter and the pelvicalyceal system, indicating that obstruction lies below the ureteropelvic junction (UPJ) — typically at the ureterovesical junction (UVJ) or lower.
From a pediatric surgical standpoint, Koff's definition remains the gold standard: "Any restriction to urinary outflow that, if left untreated, will lead to progressive kidney damage." This is important because dilation ≠ obstruction — many dilated systems never cause damage.
— Robbins & Kumar Basic Pathology, p. 530; Campbell Walsh Wein Urology, Vol. 3
2. Etiology (Causes)
Causes are divided into congenital and acquired, and further by the level of obstruction:
A. Congenital Causes
| Level | Cause |
|---|---|
| Ureteropelvic junction (UPJ) | Intrinsic stenosis (most common in neonates/infants — failure of circular muscle development), aberrant/accessory lower-pole vessel kinking the ureter (most common in older children/adults) |
| Mid-ureter | Ureteral valves, strictures, benign fibroepithelial polyps, retrocaval ureter |
| Ureterovesical junction (UVJ) | Ureterovesical junction obstruction, ureteroceles, vesicoureteral reflux (VUR), prune-belly syndrome |
| Bladder | Bladder diverticula, neurogenic bladder (spina bifida) |
| Urethra | Posterior urethral valves (PUV) — most important cause of bilateral obstruction in boys; urethral diverticula, anterior urethral valves, urethral atresia, labial fusion (females) |
B. Acquired Causes
- Foreign bodies: calculi, sloughed necrotic papillae
- Proliferative lesions: benign prostatic hyperplasia (BPH), carcinoma of the prostate, bladder tumors (papilloma, carcinoma), retroperitoneal lymphoma, carcinoma of the cervix or uterus
- Inflammatory: prostatitis, ureteritis, urethritis, retroperitoneal fibrosis
- Neurogenic: spinal cord damage causing bladder paralysis
- Pregnancy: physiological mild hydronephrosis (right > left due to uterine dextrorotation and right ovarian vein compression)
— Robbins & Kumar Basic Pathology, p. 530
3. Pathogenesis
The sequence of events following obstruction:
- Glomerular filtration continues for some time even after complete obstruction
- Urine accumulates — the filtrate diffuses back into renal interstitium and perirenal spaces, returning via lymphatics and venous system
- Pelvicalyceal dilation — progressive increase in intrapelvic pressure
- Back-pressure transmission to collecting ducts → compresses renal vasculature → arterial insufficiency + venous stasis
- Papillary effects first: the papillae, under greatest pressure, show the earliest damage
- Initial functional defect = tubular — manifested by impaired urinary concentrating ability
- Later: glomerular filtration begins to fall
- Interstitial inflammatory reaction → interstitial fibrosis
- With sudden complete obstruction, glomerular filtration is compromised early and renal function may cease with relatively mild dilation
- With subtotal or intermittent obstruction, the kidney may enlarge massively (up to 20 cm)
— Robbins & Kumar Basic Pathology, p. 530
4. Morphology / Gross & Microscopic Pathology
Gross findings:
- Massively enlarged kidney (up to 20 cm) with subtotal/intermittent obstruction
- The organ consists almost entirely of the greatly distended pelvicalyceal system
- Renal parenchyma compressed and atrophied
- Obliteration of papillae and flattening of pyramids
- If obstruction is below ureters → bilateral hydroureter + hydronephrosis

Microscopic findings:
- Early: tubular dilation and atrophy
- Late: loss of glomeruli, replacement of parenchyma by fibrous tissue
- Minimal inflammation in uncomplicated cases
- Superimposed pyelonephritis is common
5. Classification
A. By Laterality
- Unilateral: obstruction at or above the level of one ureter
- Bilateral: obstruction is distal to the bladder (e.g., PUV, BPH) — only bilateral obstruction leads to anuria and renal failure
B. By Time of Onset
- Congenital/Antenatal: detected on prenatal ultrasound (most common presentation today)
- Acquired: develops later due to stones, tumors, strictures, etc.
C. By Level of Obstruction
- Pelviureteric (UPJ) obstruction → hydronephrosis only
- Ureterovesical (UVJ) obstruction → ureterohydronephrosis (hydroureteronephrosis)
- Bladder/urethral obstruction → bilateral ureterohydronephrosis
D. SFU (Society for Fetal Urology) Grading System
The most widely used clinical grading system, based on calyceal dilation and parenchymal integrity:
| Grade | Finding |
|---|---|
| Grade 0 | No hydronephrosis |
| Grade 1 | Renal pelvis visible, no calyceal dilation |
| Grade 2 | Dilation of major calyces, parenchyma preserved |
| Grade 3 | Dilation of major + minor calyces, parenchyma preserved |
| Grade 4 | As Grade 3 + parenchymal thinning |
- SFU Grade 3: most common finding in those observed conservatively (78%)
- SFU Grade 4: most common in those requiring delayed surgical intervention (62%)
-
90% resolution for SFU Grade 1 and 2 at 12 and 18 months, respectively
E. UTD (Urinary Tract Dilation) Classification System (2014 — Multidisciplinary Consensus)
Developed to standardize nomenclature and combine APD measurement + SFU grading:
| Time | Normal APD Cutoff |
|---|---|
| 16–27 weeks gestation | < 4 mm |
| ≥ 28 weeks gestation | < 7 mm |
| Postnatal (> 48 h) | < 10 mm |
The UTD system uses a 6-point template combining APD and SFU, includes ureter and bladder assessment, and provides standardized risk stratification (UTD-1 low risk → UTD-3 high risk).
— Campbell Walsh Wein Urology, p. 478
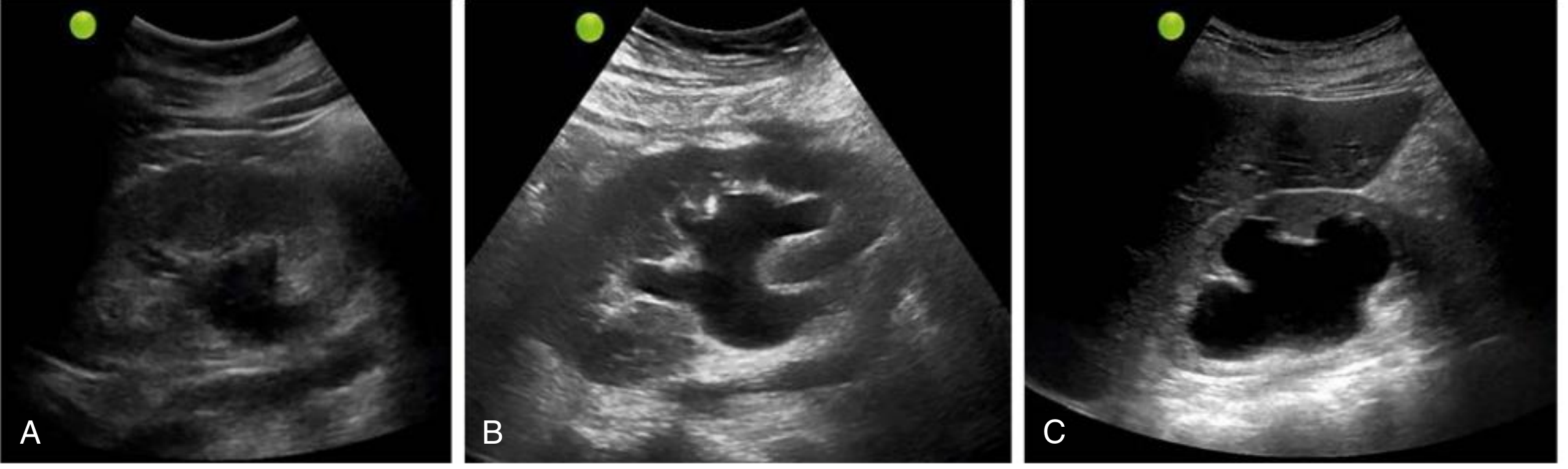
F. Ultrasound Grading (Comprehensive Clinical Nephrology)
- Mild: dilation of renal pelvis and calyces; parenchymal architecture preserved
- Moderate: medullary pyramids begin to flatten; increasing pelvicalyceal dilation
- Severe: ballooned renal pelvis and calyces (occupying most of kidney); corticomedullary differentiation lost; parenchyma thin
6. Clinical Manifestations
By Age Group
| Age | Presentation |
|---|---|
| Fetal/Antenatal | Detected on routine anomaly ultrasound (~20 weeks); most common urogenital anomaly found prenatally |
| Neonate/Infant | Palpable abdominal/flank mass (most common neonatal presentation); febrile UTI; incidental finding |
| Child/Adolescent | Loin pain (especially with lower-pole accessory vessel), nausea, vomiting, recurrent UTI, hematuria, hypertension |
| Adult | Flank pain, colicky pain, hematuria; may remain silent for long periods if unilateral |
By Laterality
- Unilateral hydronephrosis: may remain silent for long periods, especially if the other kidney is functional; the enlarged kidney may be discovered on routine examination
- Bilateral hydronephrosis (distal obstruction): leads to oliguria/anuria and renal failure
- Paradoxically, incomplete bilateral obstruction causes polyuria (not oliguria) due to defective tubular concentrating mechanisms — this may obscure the true diagnosis
- Bladder distension symptoms: dominant when obstruction is distal to the bladder
General Symptoms
- Dull, aching flank pain (chronic obstruction) or colicky pain (acute obstruction/stones)
- Recurrent UTI / pyelonephritis
- Hematuria
- Hypertension
- Nausea and vomiting (especially with intermittent obstruction mimicking GI disease)
- In children: failure to thrive, poor feeding
7. Diagnosis
A. Ultrasound (Primary and First-Line Investigation)
- Hydronephrosis appears as anechoic branching, interconnected areas in the renal collecting system
- Grades mild/moderate/severe based on degree of dilation and parenchymal thickness
- False negatives: acute or partial obstruction, volume depletion, retroperitoneal fibrosis
- Differential pitfall: parapelvic cysts (round, circumscribed, not connected to ureter); vascular malformations (use colour Doppler to confirm flow)
- Always include bladder assessment
- Prenatal: routine anomaly scan at ~18–20 weeks; postnatal scan at >48 hours of life (to allow physiologic adaptation)
B. Voiding Cystourethrogram (VCUG)
- Evaluates for vesicoureteral reflux (VUR) and posterior urethral valves
- Recommended based on UTD risk stratification + UTI risk assessment (not simply based on probability of diagnosing VUR)
C. Diuretic Renography (MAG3 / DTPA Scan)
- Assesses differential renal function and drainage
- Distinguishes obstructed from non-obstructed dilated systems
- Koff's functional definition of obstruction applies here
- Signs of obstruction: reduced differential function (<40% ipsilateral), delayed washout (T½ > 20 min after furosemide)
D. CT Urography / IVP
- Defines anatomy and level of obstruction
- Identifies calculi, tumors, retroperitoneal fibrosis
E. MR Urography
- Used in complex cases or when avoiding radiation (especially in children)
F. Antegrade / Retrograde Pyelography
- When retrograde stenting fails or percutaneous access is needed
- Defines exact location and length of obstruction
G. Laboratory
- Urea, creatinine (renal function)
- Urinalysis and urine culture (detect UTI/pyonephrosis)
- Serum electrolytes
8. Treatment
Conservative (Watchful Waiting)
- Appropriate for SFU/UTD low-grade dilation (Grade 1–2), especially if asymptomatic with preserved renal function
- Most (>90%) resolve spontaneously within 12–18 months
- Serial ultrasound surveillance
- Prophylactic antibiotics: considered in high-grade dilation or recurrent UTI (controversial — practice varies)
Surgical — Indications
Surgery is indicated when:
- Symptoms of obstruction (pain, recurrent UTI, calculi)
- Impaired/declining renal function in a salvageable kidney (approximately 20% of congenital hydronephrosis cases require pyeloplasty)
- High-grade (SFU 4) hydronephrosis
- APD ≥ 15 mm in the third trimester (reasonable positive predictive value for need for surgery for UPJO)
Surgical Procedures
1. Pyeloplasty (Gold Standard for UPJO)
- Anderson-Hynes Dismembered Pyeloplasty: excision of the obstructed UPJ segment + reanastomosis of the spatulated ureter to the dependent portion of the renal pelvis; allows transposition of the ureter anterior to an aberrant lower-pole vessel
- Success rate >90–95%
- Approaches: open (flank/dorsal lumbotomy), laparoscopic, retroperitoneoscopic, robotic-assisted (increasingly preferred)
- Complications: prolonged urinary drainage, failure to improve washout, occasional worsening of hydronephrosis
2. Endopyelotomy (Minimally Invasive)
- Antegrade (percutaneous) or retrograde (ureteroscopic) incision of the UPJ
- Lower success rate than pyeloplasty (~60–85%) — preferred in select adults; less favoured in children
- Lower cost than minimally invasive pyeloplasty in some analyses
3. Ureteral Reimplantation
- For UVJ obstruction (distal ureteral stenosis)
- Intravesical (e.g., Cohen, Politano-Leadbetter) or extravesical (e.g., Lich-Gregoir) approaches
- Aims for a 5:1 submucosal tunnel length-to-diameter ratio (Paquin's rule)
4. Percutaneous Nephrostomy
- Emergency decompression for infected hydronephrosis (pyonephrosis), urosepsis, or acute obstructive renal failure
- Bridge to definitive repair
5. Ureteral Stent (JJ/Double-J Stent)
- Short-term decompression before or after surgery
- Also used diagnostically to assess impact of obstruction on function
6. Ablation / Valve Fulguration
- For posterior urethral valves (cystoscopic ablation)
7. Nephrectomy
- For a non-functioning kidney (split function < 10–15%) with a normal contralateral kidney
— Campbell Walsh Wein Urology; Brenner and Rector's The Kidney
9. Differential Diagnosis
| Condition | How to Distinguish |
|---|---|
| Parapelvic renal cysts | Round, circumscribed, not connected to ureter; no branching pattern; no hydroureter |
| Renal vascular malformations | Anechoic on US; colour Doppler shows flow |
| Multicystic dysplastic kidney (MCDK) | Non-communicating cysts of varying size; no renal pelvis visible; no function on renography |
| Polycystic kidney disease | Bilateral, multiple cysts throughout parenchyma, family history |
| Pyonephrosis | Hydronephrosis + internal echoes on US + fever + flank pain; requires urgent drainage |
| Prune-belly syndrome | Dilated, tortuous, non-obstructed ureters + bilateral cryptorchidism + absent abdominal musculature |
| Megaureter (non-obstructive) | Dilated ureter without functional obstruction on renography; may resolve spontaneously |
| Vesicoureteral reflux | Demonstrated on VCUG; dilation present during voiding, not at rest |
| Retroperitoneal fibrosis | Bilateral medial ureteral deviation + contrast CT showing periaortic soft tissue |
| Renal tumor | Solid mass ± calcification on CT; hydronephrosis secondary |
10. Age-Specific Patterns
| Age Group | Dominant Cause | Typical Presentation |
|---|---|---|
| Fetus | UPJ obstruction, posterior urethral valves, ureterocele | Antenatal US finding |
| Neonate (0–1 mo) | UPJ obstruction (intrinsic stenosis), PUV | Abdominal mass, oligohydramnios history |
| Infant/Toddler | UPJ obstruction, VUR | Febrile UTI, abdominal mass |
| Child/Adolescent | Accessory lower-pole vessel (extrinsic UPJ), calculi | Loin pain, nausea, vomiting, haematuria |
| Adult | Calculi, BPH, ureteral stricture, malignancy, retroperitoneal fibrosis | Flank pain, renal colic, urinary symptoms |
| Pregnant female | Physiological compression (right >> left) | Mild bilateral or right-sided dilation; resolves postpartum |
11. Sex Differences (Male vs. Female)
| Feature | Male | Female |
|---|---|---|
| Incidence | More common — hydronephrosis (especially UPJO) is more frequent in males, particularly in infants and toddlers | Less common overall |
| Predominant cause in neonate | UPJ obstruction (intrinsic); Posterior urethral valves (unique to males — most severe cause of bilateral obstruction) | UPJ obstruction, ureterocele, duplex system anomalies |
| Unique obstructive lesions | Posterior urethral valves, anterior urethral valves, urethral diverticula | Labial fusion (rarely causes obstruction), urethral diverticula |
| Laterality | Left-sided predominance for UPJO | Similar |
| Acquired in adults | BPH and prostate carcinoma are major causes | Carcinoma of the cervix/uterus, pregnancy, labial fusion |
| Pregnancy | — | Physiological ureteral compression → mild hydronephrosis (right > left); usually resolves postpartum |
| Prognosis | PUV can cause bilateral damage and chronic kidney disease | Generally more favourable in congenital forms without PUV equivalent |
Key statistic: UPJO predominates on the left side and is bilateral in 10–40% of cases; there may be an increased familial incidence. Males account for the majority of presentations in infancy.
— Campbell Walsh Wein Urology, Vol. 3; Brenner and Rector's The Kidney
Summary Table
| Feature | Key Points |
|---|---|
| Definition | Dilation of pelvis ± calyces ± ureter due to obstruction |
| Most common congenital cause | UPJ obstruction (intrinsic narrowing in infants; accessory vessel in older children/adults) |
| Most severe cause in boys | Posterior urethral valves (bilateral obstruction, renal failure) |
| Pathogenesis key | Tubular damage first → glomerular failure late; complete obstruction → parenchymal atrophy |
| Gold standard diagnosis | Ultrasound + MAG3 renography (function + drainage) |
| Gold standard treatment for UPJO | Anderson-Hynes dismembered pyeloplasty (>95% success) |
| Observation appropriate | SFU Grade 1–2; >90% resolve by 18 months |
| Surgery indicated | Declining function, symptoms, SFU Grade 4, APD ≥15 mm (3rd trimester) |
| Male predominance | Boys affected more, especially infants/toddlers; PUV exclusive to males |
| Female-specific | Physiological hydronephrosis in pregnancy; cervical/uterine malignancy in adults |
Sources: Robbins & Kumar Basic Pathology (p. 530); Campbell Walsh Wein Urology, 3-Volume Set; Comprehensive Clinical Nephrology, 7th Edition; Brenner and Rector's The Kidney, 2-Volume Set; Mulholland and Greenfield's Surgery, 7th Edition
This is a shared conversation. Sign in to Orris to start your own chat.