MD MEDICINE UNIVERSITY EXAM NOTES
QUESTION 1: CONGESTIVE HEART FAILURE (CHF) — 20 Marks
DEFINITION
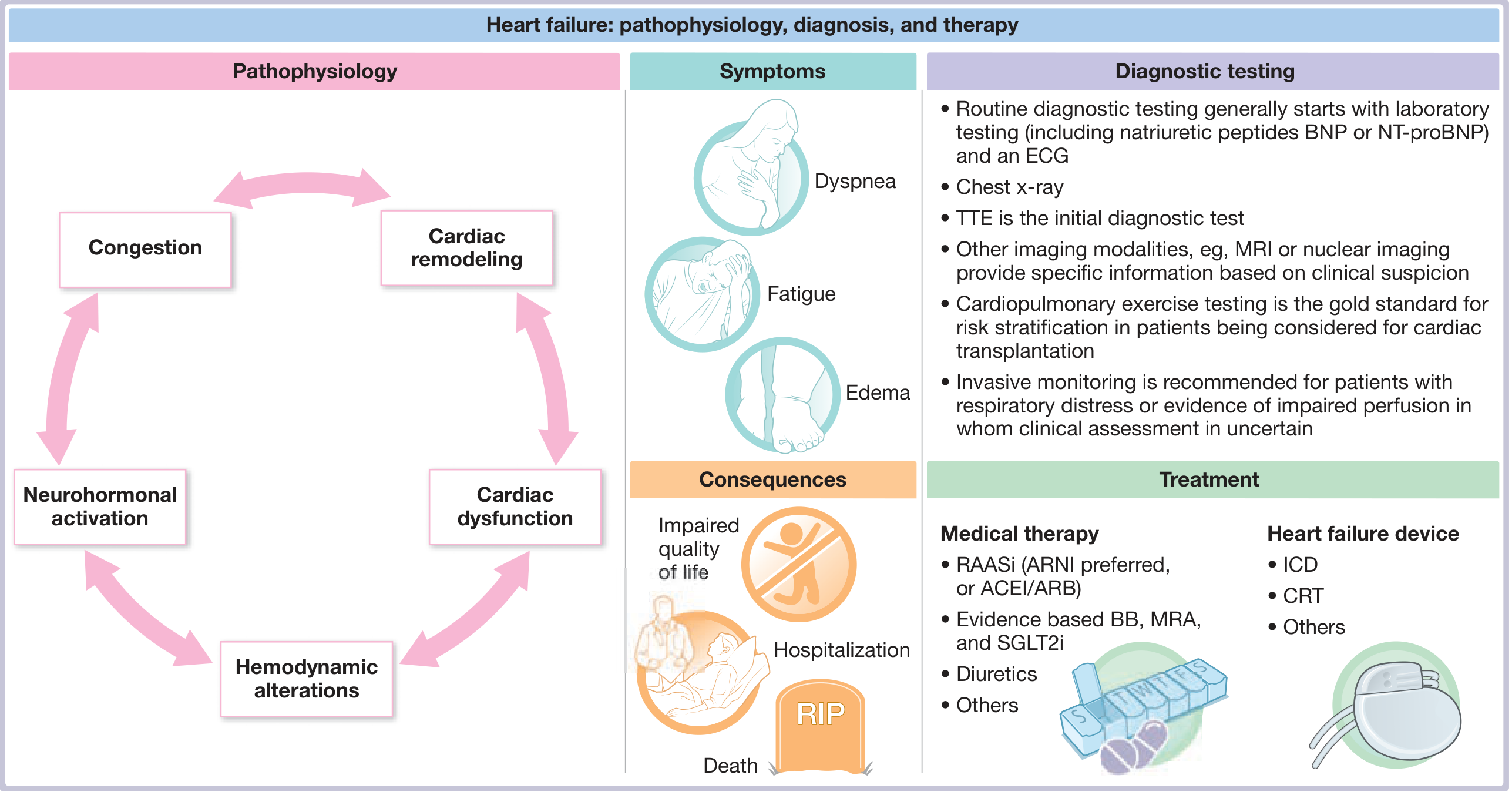
Heart failure (HF) is a clinical syndrome resulting from the inability of the heart to meet the metabolic requirements of the body at normal filling pressures. The term "congestive heart failure" (CHF) is still widely used, though "heart failure" is preferred because fluid congestion may not always be present.
I. ETIOPATHOGENESIS
A. Etiology (Causes)
| Category | Common Causes |
|---|
| Ischemic | CAD, MI (most common cause ~70%) |
| Pressure Overload | Systemic HTN, aortic stenosis, coarctation of aorta |
| Volume Overload | MR, AR, VSD, PDA |
| Cardiomyopathy | Dilated, hypertrophic, restrictive, PPCM |
| Metabolic | Diabetes mellitus, hypothyroidism, hyperthyroidism |
| Toxins | Alcohol, anthracyclines (adriamycin), cobalt |
| Infections | Viral myocarditis (coxsackie B), Chagas disease, diphtheria |
| Infiltrative | Amyloidosis, sarcoidosis, hemochromatosis |
| High-output causes | Anaemia, thyrotoxicosis, beriberi, AV malformations, Paget's disease |
| Arrhythmias | AF, complete heart block, sustained VT |
| Pericardial | Constrictive pericarditis, cardiac tamponade |
| Congenital | Septal defects, complex CHD |
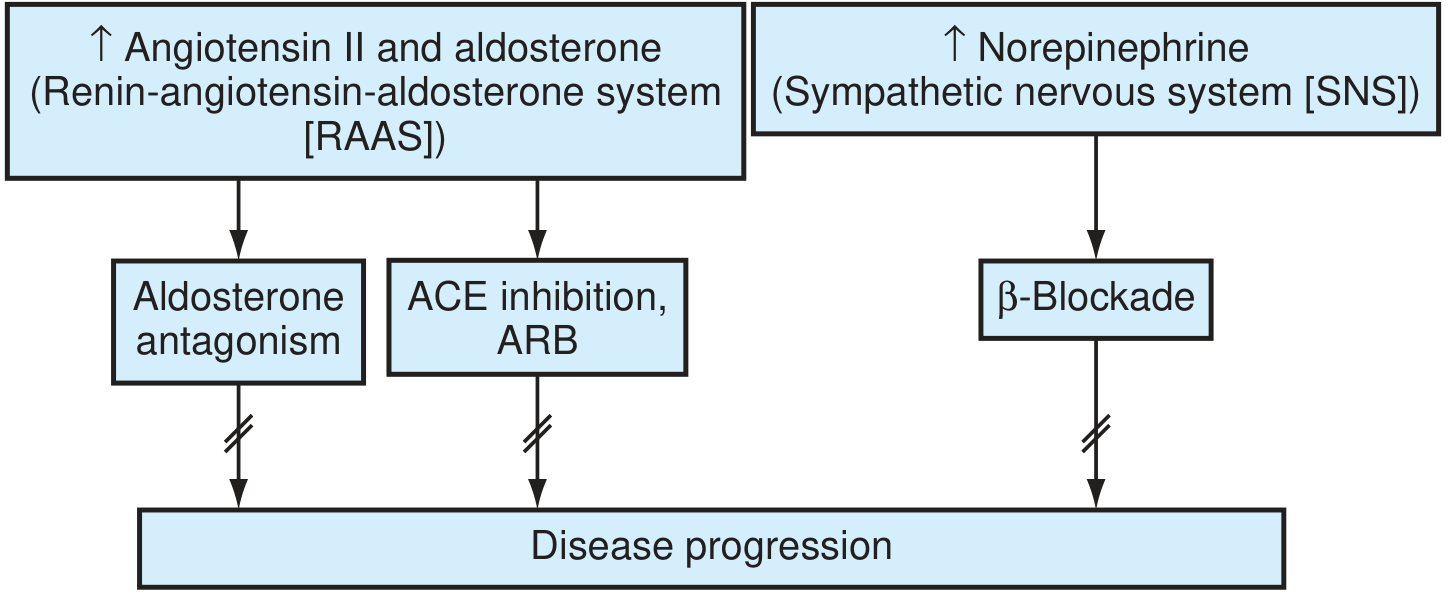
B. Pathogenesis — Neurohormonal Model (Current Concept)
The old hemodynamic model (pump failure only) has been replaced by the neurohormonal model incorporating LV remodeling.
Step-by-step pathogenesis:
INITIAL CARDIAC INJURY
(MI / HTN / Valvular disease / Cardiomyopathy)
|
v
LV DYSFUNCTION
(Reduced CO / Increased filling pressures)
|
v
COMPENSATORY MECHANISMS ACTIVATED
/ \
RAAS SNS
activated activated
(Ang II, Aldosterone) (↑ Norepinephrine)
\ /
\ /
v v
┌─────────────────────────────────────┐
│ LV REMODELING │
│ - Myocyte hypertrophy │
│ - Myocyte apoptosis │
│ - Interstitial fibrosis │
│ - Chamber dilation │
│ - Collagen deposition (↑ MMPs) │
└─────────────────────────────────────┘
|
v
↓ LV function → ↑ Wall stress
|
v
PROGRESSIVE CARDIAC DECOMPENSATION
(↑ EDV, ↑ EDP, Pulmonary congestion)
|
v
CLINICAL HF
Key neurohormonal mediators:
| Mediator | Source | Effect |
|---|
| Angiotensin II | RAAS | Vasoconstriction, myocyte apoptosis, aldosterone secretion, fibrosis |
| Aldosterone | Adrenal cortex | Na+ retention, K+ loss, myocardial fibrosis |
| Norepinephrine | SNS | Vasoconstriction, tachycardia, direct myocardial toxicity, down-regulation of β-receptors |
| Endothelin-1 | Vascular endothelium | Vasoconstriction |
| BNP / ANP | Ventricles/atria | Counter-regulatory (vasodilation, natriuresis) |
| TNF-α / IL-6 | Myocardium | Cytokine-mediated myocardial depression |
II. CLASSIFICATION
A. ACC/AHA Staging (Progressive, irreversible)
| Stage | Description | Equivalent NYHA | Management |
|---|
| A | At risk (HTN, DM, CAD, FH) - NO structural disease | - | Risk factor modification |
| B | Structural disease, NO symptoms | NYHA I | ACEi/ARB + Beta blocker |
| C | Structural disease WITH symptoms | NYHA II-III | Full GDMT |
| D | Refractory symptoms at rest | NYHA IV | Advanced therapies (VAD, transplant) |
Memory tip: A = At risk, B = Before symptoms, C = Clinical HF, D = Death approaching
B. NYHA Functional Classification (Symptomatic, reversible)
| Class | Symptoms | MVO2 (mL/kg/min) |
|---|
| I | No symptoms with ordinary activity | >20 |
| II | Slight limitation; comfortable at rest, symptoms on ordinary exertion | 16-20 |
| III | Marked limitation; symptoms on less than ordinary activity | 10-16 |
| IV | Unable to carry on any activity; symptoms at rest | <10 |
C. By Ejection Fraction
| Type | EF | Mechanism |
|---|
| HFrEF (Systolic HF) | <40% | Impaired contractility |
| HFmrEF (Mildly reduced) | 40-49% | Mixed |
| HFpEF (Diastolic HF) | ≥50% | Impaired relaxation/filling; increased stiffness |
D. By Onset
- Acute HF - new onset or rapid decompensation
- Chronic HF - stable, persistent symptoms
E. By Side
- Left HF - pulmonary congestion (dyspnea, orthopnea, PND)
- Right HF - systemic venous congestion (edema, JVD, hepatomegaly)
- Biventricular HF (most common in clinical practice)
F. By Output
- Low-output HF - most cases (CAD, cardiomyopathy, HTN)
- High-output HF - thyrotoxicosis, beriberi, anaemia, Paget's disease
III. CLINICAL PRESENTATION
Symptoms
LEFT HEART FAILURE RIGHT HEART FAILURE
| |
Dyspnea on exertion (earliest) Ankle swelling / pitting edema
Orthopnea (2-3 pillow) Right upper quadrant pain
Paroxysmal nocturnal dyspnea (PND) Anorexia, nausea, bloating
Cardiac cough (dry, nocturnal) Weight gain (fluid)
Fatigue, exercise intolerance Abdominal distension
Haemoptysis (pink frothy - severe) Oliguria (daytime), nocturia
Signs on Examination
Vital signs:
- Tachycardia (compensatory)
- Low BP or narrow pulse pressure
- Pulsus alternans (severe LV dysfunction)
- Cheyne-Stokes respiration (severe)
Cardiovascular exam:
- Displaced apex beat (LVE - shifted down and out)
- S3 gallop (ventricular filling sound) - pathognomonic
- S4 gallop (stiff/hypertrophied ventricle)
- Murmurs of underlying cause (AS, MR, AR)
- Raised JVP (right HF)
- Hepatojugular reflux positive
Respiratory exam:
- Bibasilar fine crepitations (pulmonary oedema)
- Dullness at bases (pleural effusion - usually right-sided)
Abdomen:
- Hepatomegaly (tender, pulsatile in TR)
- Ascites (chronic RHF)
- Splenomegaly (portal hypertension)
Periphery:
- Pitting pedal edema (bilateral)
- Cold extremities, cyanosis (peripheral)
- Cardiac cachexia (severe, chronic)
IV. DIAGNOSIS
A. Investigations
Flowchart - Diagnostic Approach:
CLINICAL SUSPICION OF HF
(Dyspnea + Edema + Fatigue)
|
v
INITIAL WORKUP (All patients)
| | |
ECG CXR BNP/NT-proBNP
(LVH, AF, (Cardiomegaly, BNP >100 pg/mL
ischemia, pulmonary NT-proBNP >300
BBB, QRS congestion, pg/mL → HF
duration) Kerley B lines, likely
pleural eff)
|
v
ECHOCARDIOGRAPHY (Key test)
- Systolic function (EF)
- Diastolic function
- Wall motion abnormalities
- Valvular disease
- LV dimensions
|
┌──────┴──────┐
EF <40% EF >50%
(HFrEF) (HFpEF)
| |
GDMT Control rate,
(see Rx) BP, risk factors
|
v
ADDITIONAL TESTS (As indicated)
- CBC (anaemia)
- RFT/EFT (renal/liver function)
- TFT (thyroid)
- Iron studies (ferritin, TSAT)
- Serum electrolytes, creatinine
- Cardiac MRI (myocarditis, amyloid, sarcoid)
- Coronary angiography (if ischemic etiology suspected)
- Radionuclide ventriculography (RNVG) - MUGA scan
- 6-minute walk test (exercise tolerance)
- Cardiopulmonary exercise testing (CPET) - gold standard for transplant evaluation
- Sleep study (OSA co-morbidity common)
B. Key Diagnostic Criteria
Framingham Criteria for CHF:
Major criteria (≥2 major OR 1 major + 2 minor):
- PND or orthopnea
- Neck vein distension
- Rales
- Cardiomegaly on CXR
- Acute pulmonary oedema
- S3 gallop
- Increased venous pressure (>16 cmH2O)
- Hepatojugular reflux
- Pulmonary oedema on CXR
- Weight loss ≥4.5 kg in 5 days with treatment
Minor criteria:
- Bilateral ankle oedema
- Nocturnal cough
- Dyspnoea on exertion
- Hepatomegaly
- Pleural effusion
- HR >120/min
- Decrease in VC by 1/3 from maximum
C. CXR Findings (Ordered by increasing severity)
Mild → Moderate → Severe
| | |
Cardiomegaly Kerley B lines Bat-wing / Butterfly
(CT ratio (septal lines) pulmonary oedema
>0.5)
Peribronchial Pleural effusions
cuffing (bilateral)
Cephalization Air-space opacities
of vessels
V. TREATMENT
A. General / Non-Pharmacological Measures
- Salt restriction (<2 g/day Na+)
- Fluid restriction (1.5-2 L/day if severe)
- Daily weight monitoring (report if gain >2 kg/week)
- Cardiac rehabilitation and regular exercise (NYHA I-III)
- Smoking cessation, alcohol abstinence
- Vaccinations (influenza, pneumococcus)
- Avoid NSAIDs, CCBs (verapamil, diltiazem), class I antiarrhythmics
B. Pharmacological Treatment - HFrEF (EF <40%)
"FOUR PILLARS" of GDMT for HFrEF:
┌─────────────────────────────────────────────────────────────────┐
│ FOUR PILLARS OF GDMT (HFrEF) │
├──────────────────┬──────────────────┬──────────────┬────────────┤
│ RAAS Blocker │ Beta-Blocker │ MRA │ SGLT2i │
│ (ACEi/ARB/ARNI) │ │ │ │
├──────────────────┼──────────────────┼──────────────┼────────────┤
│ Sacubitril/ │ Carvedilol │Spironolactone│Dapagliflozin│
│ Valsartan (ARNI) │ Metoprolol XL │Eplerenone │Empagliflozin│
│ Ramipril/Enalapril│ Bisoprolol │ │ │
│ Losartan/Valsartan│ │ │ │
├──────────────────┼──────────────────┼──────────────┼────────────┤
│ ↓ Mortality 20% │ ↓ Mortality 34% │↓ Mortality │↓ HHF+CV │
│ (PARADIGM-HF) │ (MERIT-HF, │25-30% │death 25% │
│ │ CIBIS-II) │(RALES, │(DAPA-HF, │
│ │ │EMPHASIS-HF) │EMPEROR-R) │
└──────────────────┴──────────────────┴──────────────┴────────────┘
Additional medications:
| Drug | Class | Indication |
|---|
| Furosemide / Torsemide | Loop diuretic | Fluid overload (symptom relief) |
| Hydralazine + Isosorbide dinitrate | Vasodilators | ACEi/ARB intolerant (cough, renal failure), Black patients |
| Ivabradine | If-channel blocker | HR ≥70 bpm, sinus rhythm, LVEF ≤35% |
| Digoxin | Cardiac glycoside | Persistent symptoms, AF rate control, reduce HHF |
| Vericiguat | sGC stimulator | High-risk symptomatic HFrEF (VICTORIA trial) |
| Tafamidis | TTR stabilizer | TTR-amyloid cardiomyopathy |
| IV Iron (ferric carboxymaltose) | Iron supplementation | Iron deficiency (TSAT <20%, ferritin <100) |
C. Treatment of HFpEF (EF ≥50%)
Note: Unlike HFrEF, fewer proven mortality-reducing therapies exist.
- SGLT2i (dapagliflozin, empagliflozin) - EMPEROR-Preserved, DELIVER trials - reduce HHF
- Diuretics - symptom relief
- Control underlying causes: HTN, AF, CAD, DM, obesity
- Spironolactone - some benefit (TOPCAT trial, borderline)
D. Device Therapy
| Device | Indication |
|---|
| ICD (Implantable cardioverter defibrillator) | LVEF ≤35%, NYHA II-III, >3 months optimal medical therapy, life expectancy >1 year |
| CRT (Cardiac resynchronization therapy) | LVEF ≤35%, LBBB, QRS ≥150 ms, NYHA II-IV, sinus rhythm |
| CRT-D | Combined CRT + ICD |
| LVAD (Left ventricular assist device) | NYHA IV / INTERMACS 1-3, bridge to transplant or destination therapy |
E. Treatment of Acute Decompensated HF (ADHF)
ACUTE HF → ASSESS: Wet/Dry + Warm/Cold Profile
(Stevenson Classification)
|
v
┌──────────┬────────────┐
│ │ │
Wet-Warm Wet-Cold Dry-Cold
(Most (Cardiogenic (Low output,
common) shock) no congestion)
| | |
Diuretics Inotropes Volume
Vasodilators +Diuretics challenge
(IV Nitrates) (Dobutamine,
Dopamine)
Immediate management:
- Positioning - sit upright (reduces preload)
- O2 - maintain SpO2 >94%; NIV (CPAP/BiPAP) for respiratory failure
- IV furosemide - 40-80 mg IV bolus (decongestive)
- IV nitrates - sublingual/IV GTN (if SBP >90 mmHg) - reduces preload/afterload
- Morphine - 2-4 mg IV (reduces anxiety, mild venodilation) - use with caution
- Vasopressors - norepinephrine if cardiogenic shock (MAP <65)
- Inotropes - Dobutamine/Dopamine for low-output shock
F. Surgical and Advanced Therapies
- Revascularization (CABG/PCI) - ischemic HF with viable myocardium
- Valve repair/replacement - valvular cause
- Cardiac transplantation - Gold standard for end-stage HF (NYHA IV, LVEF <20%, VO2 max <10 mL/kg/min)
- LVAD - Bridge to transplant or destination therapy
- Ultra-filtration - diuretic-resistant fluid overload
- Cardiac contractility modulation (CCM) - newer device for non-LBBB patients
Overall Treatment Algorithm (Summary Flowchart)
G. Precipitating Factors (Must identify and treat) - Mnemonic: "FAILURE"
| Letter | Factor |
|---|
| F | Forgot to take medications / Fast AF |
| A | Anaemia / Arrhythmia |
| I | Ischemia / Infarction |
| L | Lifestyle - Na+/fluid excess |
| U | Uncontrolled HTN |
| R | Renal failure (cardiorenal syndrome) |
| E | Embolism (PE) / Endocarditis / Exertion |
QUESTION 2: RECENT ADVANCES IN INVESTIGATION & TREATMENT OF CAD — 20 Marks
DEFINITION
Coronary artery disease (CAD) is atherosclerotic obstruction of the coronary arteries resulting in myocardial ischemia. It encompasses stable angina, unstable angina, NSTEMI, STEMI, and sudden cardiac death.
PART A: RECENT ADVANCES IN INVESTIGATION OF CAD
1. Coronary CT Angiography (CCTA)
Key advances:
| Feature | Details |
|---|
| Indication | Intermediate pre-test probability of CAD (10-70%), low-risk acute chest pain |
| Technique | Multi-detector CT (64-slice, 256-slice, dual-source CT) |
| Sensitivity/Specificity | ~95-99% sensitivity for significant stenosis |
| Calcium scoring | Agatston score; CAC=0 near-zero event risk |
| Advantage | Non-invasive, rapid, no arterial puncture |
| SCOT-HEART trial | CCTA-guided strategy reduced MI at 5 years vs standard care |
| PROMISE trial | CCTA non-inferior to functional testing for outcomes |
2. CT-Derived Fractional Flow Reserve (FFR-CT / HeartFlow)
CCTA Images → 3D coronary model → Computational fluid dynamics
|
v
FFR-CT value per vessel
(≤0.80 = hemodynamically significant)
|
┌─────────────────────┴────────────────┐
FFR-CT >0.80 FFR-CT ≤0.80
(Medical therapy) (Proceed to invasive
coronary angiography)
- PLATFORM trial: FFR-CT reduced unnecessary invasive angiography by 61%
- DISCOVER-FLOW, DeFACTO, NXT trials: FFR-CT more accurate than anatomical CTA
3. Invasive Coronary Physiology
| Test | Principle | Cut-off | Use |
|---|
| FFR (Fractional Flow Reserve) | Pd/Pa during maximal hyperaemia (adenosine) | ≤0.80 = significant | Guides revascularization in intermediate stenoses |
| iFR (Instantaneous Wave-Free Ratio) | Diastolic pressure ratio, no adenosine | ≤0.89 = significant | Equivalent to FFR (DEFINE-FLAIR, iFR-SWEDEHEART trials) |
| CFR (Coronary Flow Reserve) | Hyperaemic vs resting flow | <2.0 = abnormal | Microvascular disease |
| IMR (Index of Microvascular Resistance) | Distal pressure × transit time | >25 = abnormal | Microvascular disease post-PCI |
| Resting Full-cycle Ratio (RFR) | Resting Pd/Pa | ≤0.89 | Avoids adenosine |
4. Intravascular Imaging
| Modality | Principle | Resolution | Key Use |
|---|
| IVUS (Intravascular Ultrasound) | Sound waves | 100-150 μm | Plaque burden, stent sizing, stent expansion, calcium |
| OCT (Optical Coherence Tomography) | Near-infrared light | 10-15 μm (10x better than IVUS) | Plaque morphology, thrombus, fibrous cap thickness, stent apposition |
| NIRS (Near-Infrared Spectroscopy) | Lipid detection | - | Lipid-rich plaque (NIRS-IVUS combined) |
ILUMIEN IV trial (2022): OCT-guided PCI superior to angiography-guided PCI for stent expansion.
ULTIMATE trial: IVUS-guided PCI reduced MACE vs angiography-guided.
5. Advanced Non-Invasive Imaging
| Test | Key Feature | Recent Advance |
|---|
| Cardiac MRI | Gold standard for viability, function, scar | T1 mapping, ECV fraction - quantify diffuse fibrosis |
| PET (Myocardial Perfusion PET) | Absolute flow quantification | Rb-82 or N-13 ammonia PET; detects microvascular disease |
| SPECT (Myocardial Perfusion Imaging) | Perfusion defects | CZT cameras - higher resolution, lower dose, faster |
| Echocardiography | Wall motion | Strain imaging (GLS); 3D echo; contrast echo (LVO, perfusion) |
6. Novel Biomarkers
| Biomarker | Significance |
|---|
| High-sensitivity Troponin I/T (hs-cTnI/T) | Detects MI at 0h/1h (0h/1h rule-out algorithm) - ESC 2023 guidelines |
| Copeptin | Combined with troponin - rapid rule-out in <2 hours |
| BNP/NT-proBNP | Identifies concurrent HF in ACS |
| hsCRP / IL-6 | Inflammatory risk markers |
| Lp(a) | Emerging genetic risk marker; target for newer therapies |
| PCSK9 levels | Target biomarker for lipid-lowering therapy |
| GDF-15 | Prognostic marker in NSTE-ACS |
7. Wearable Technology and AI
- Continuous ECG wearables (Apple Watch, Zio Patch) - detect silent AF, ischemia
- AI-based ECG interpretation - detect LV dysfunction, CAD, HF from 12-lead ECG
- Deep learning applied to CCTA - automated stenosis quantification
- Remote monitoring - implantable hemodynamic sensors (CardioMEMS for HF-CAD overlap)
PART B: RECENT ADVANCES IN TREATMENT OF CAD
1. Pharmacological Advances
A. Lipid-Lowering Therapy
LDL-C Reduction Strategy (Escalating approach)
|
Statin therapy (first-line)
(Atorvastatin 40-80mg, Rosuvastatin 20-40mg)
|
If LDL not at goal (< 1.4 mmol/L in very high risk)
|
Add Ezetimibe 10mg (IMPROVE-IT trial)
|
If still not at goal
|
PCSK9 inhibitors
(Evolocumab 140mg Q2W - FOURIER trial)
(Alirocumab 75-150mg Q2W - ODYSSEY OUTCOMES trial)
↓LDL by 50-60% additional; ↓MACE by 15-20%
|
Inclisiran (siRNA) - 2x yearly injection (ORION-10, ORION-11)
|
Bempedoic acid - ACL inhibitor, oral, for statin-intolerant
(CLEAR Outcomes trial - ↓MACE 13%)
B. Antiplatelet Therapy Advances
| Strategy | Evidence |
|---|
| Dual Antiplatelet Therapy (DAPT) - Aspirin + P2Y12i | Standard post-ACS/PCI |
| Ticagrelor (90 mg BD) vs Clopidogrel | PLATO trial: ↓ mortality 19% in ACS |
| Prasugrel (10 mg OD) vs Clopidogrel | TRITON-TIMI 38: ↓ CV death/MI/stroke (↑ bleeding) |
| De-escalation of DAPT | TROPICAL-ACS, HOST-REDUCE: potent → clopidogrel after 1 month |
| DAPT duration | 1-3 months in high bleed-risk (ARC-HBR); 6-12 months standard |
| P2Y12 monotherapy after 1-3 months DAPT | TWILIGHT, TICAGRELOR-SOLO trials |
| Cangrelor (IV P2Y12i) | Bridging therapy, peri-PCI |
| Vorapaxar (PAR-1 antagonist) | TRACER: reduces recurrent MI in stable CAD (↑ ICH risk) |
C. Anticoagulation in CAD
| Drug | Indication | Trial |
|---|
| Rivaroxaban 2.5 mg BD + Aspirin | Stable CAD / PAD (vascular dose) | COMPASS trial - ↓MACE 24% |
| Betrixaban, Apixaban | Post-ACS extended VTE prophylaxis | |
| Reviparin / LMWH | ACS bridge to PCI | |
D. Anti-Anginal Drugs
| Drug | Mechanism | Evidence |
|---|
| Ranolazine | Late Na+ channel blocker | Reduces angina frequency without affecting HR/BP (CARISA trial) |
| Ivabradine | If-channel blocker (HR reduction) | SIGNIFY trial (CAD with angina, HR ≥70) |
| Trimetazidine | Metabolic (shifts to glucose oxidation) | Reduces angina, improves LV function |
| Nicorandil | K-ATP opener + nitrate | IONA trial: ↓ coronary events |
| Colchicine 0.5 mg OD | Anti-inflammatory | COLCOT trial: ↓MACE 23% post-MI; LoDoCo2: stable CAD |
E. Diabetes Drugs with CV Benefit
| Drug | Trial | Benefit |
|---|
| SGLT2 inhibitors (Empagliflozin, Canagliflozin, Dapagliflozin) | EMPA-REG, CANVAS, DECLARE | ↓ CV death, HHF, renal outcomes |
| GLP-1 RAs (Liraglutide, Semaglutide, Dulaglutide) | LEADER, SUSTAIN-6, REWIND | ↓ MACE, CV death |
2. Interventional Advances (PCI)
A. Generation of Coronary Stents
Bare Metal Stents (BMS) - 1st gen
↓ (high restenosis - 20-30%)
Drug Eluting Stents (DES) 1st gen - Sirolimus, Paclitaxel
↓ (reduced restenosis to 5-10%; late ST concern)
DES 2nd gen - Everolimus, Zotarolimus, Biolimus
(Thinner struts, biocompatible/biodegradable polymer)
↓ (current standard)
Bioresorbable Vascular Scaffolds (BVS/BRS)
- Absorb BVS (Abbott) - fully dissolves in 3 years
- Concern: ↑ late scaffold thrombosis - use cautious
Drug-coated balloons (DCB) - no permanent implant
- For ISR, small vessels, bifurcations
B. Complex PCI Techniques
| Technique | Use |
|---|
| Rotational atherectomy (Rotablator) | Heavily calcified lesions, undilatable plaque |
| Orbital atherectomy | Calcified CAD |
| Intravascular lithotripsy (Shockwave IVL) | Severe calcification - sonic pressure waves |
| Laser atherectomy (EXCIMER) | Ostial lesions, ISR, SVG lesions |
| Bifurcation PCI | "Provisional T" stenting vs DK-Crush |
| CTO-PCI | Chronic total occlusion - retrograde approach, ADR |
| CHIP (Complex High-risk Indicated PCI) | Protected PCI with hemodynamic support (Impella) |
C. Hemodynamic Support Devices (for High-Risk PCI)
| Device | Mechanism | CO support |
|---|
| IABP (Intra-aortic balloon pump) | Counterpulsation | 0.5-1.0 L/min |
| Impella (CP, 5.0, 5.5) | Axial flow catheter, LV to aorta | 2.5-5.5 L/min |
| TandemHeart | Extracorporeal centrifugal pump, LA to femoral artery | 3.5-5.0 L/min |
| VA-ECMO | Full cardiopulmonary bypass | 4-6 L/min |
PROTECT II trial: Impella superior to IABP for high-risk PCI outcomes.
3. Surgical Advances - CABG
| Advance | Details |
|---|
| Off-pump CABG (OPCAB) | Avoids cardiopulmonary bypass; less systemic inflammation |
| Minimally invasive CABG (MIDCAB, TECAB) | Smaller incisions, robotic-assisted |
| Bilateral IMA grafting (BIMA) | Better long-term patency vs single IMA; ART trial |
| Radial artery grafts | Superior to saphenous vein at 10 years (RAPS trial) |
| Hybrid revascularization | LIMA-LAD (surgical) + PCI of non-LAD |
| No-touch saphenous vein harvesting | Better vein conduit quality, ↓ atherosclerosis |
EXCEL trial: PCI with 2nd-gen DES vs CABG for left main CAD (comparable outcomes at 5 years).
SYNTAX trial: CABG superior in complex 3VD (SYNTAX score >32).
4. Cardiac Rehabilitation (CR)
- Exercise-based CR reduces all-cause mortality by ~20% post-MI/PCI
- Telecardiac rehabilitation and digital CR platforms (new development)
5. Emerging / Future Therapies
| Therapy | Mechanism | Stage |
|---|
| Inclisiran | siRNA targeting PCSK9, 2x/year injection | Approved (FDA/EMA) |
| Pelacarsen | Antisense oligonucleotide against Lp(a) | Phase 3 (OCEAN(a)-OUTCOMES trial) |
| Obicetrapib (CETP inhibitor) | ↑ HDL, ↓ LDL | Phase 3 |
| Gene therapy | PCSK9 CRISPR editing, single lifetime dose | Early trials |
| CAR-T for HF/CAD | Anti-fibrotic immune cells | Preclinical |
| Coronary gene therapy | Angiogenesis (VEGF, HGF) | Trials ongoing |
| Colchicine 0.5 mg | Anti-NLRP3 inflammasome | Practice-changing (COLCOT, LoDoCo2) |
| Ziltivekimab (IL-6 inhibitor) | Anti-inflammatory in CKD+CAD | Phase 3 |
KEY TRIALS SUMMARY (CAD - for exam)
| Trial | Drug/Intervention | Key Finding |
|---|
| PLATO | Ticagrelor vs Clopidogrel | Ticagrelor ↓ mortality 19% in ACS |
| TRITON | Prasugrel vs Clopidogrel | Prasugrel ↓ MACE but ↑ bleeding |
| FOURIER | Evolocumab | ↓ LDL 59%, ↓ MACE 15% |
| ODYSSEY | Alirocumab | ↓ LDL 62%, ↓ all-cause mortality |
| COMPASS | Rivaroxaban 2.5mg + ASA | ↓ MACE 24% in stable CAD |
| IMPROVE-IT | Ezetimibe + Statin | ↓ MACE 6.4%; lower LDL = better |
| COLCOT | Colchicine post-MI | ↓ MACE 23% |
| LoDoCo2 | Colchicine stable CAD | ↓ MACE 31% |
| ISCHEMIA | PCI vs Medical therapy (stable CAD) | No difference in outcomes (landmark) |
| SYNTAX | CABG vs PCI in 3VD/LM | CABG superior in complex disease |
| EXCEL | PCI vs CABG left main | Comparable 5-year outcomes |
| PARADIGM-HF | Sacubitril/Valsartan | ↓ CV death 20% in HFrEF |
| DAPA-HF | Dapagliflozin | ↓ CV death/HHF 26% in HFrEF |
| EMPEROR-R | Empagliflozin | ↓ CV death/HHF 25% in HFrEF |
QUICK REVISION - HIGH-YIELD POINTS
CHF
- Most common cause: CAD/IHD
- Best initial test: Echocardiography
- Best biomarker: BNP/NT-proBNP
- Pathognomonic sign: S3 gallop
- Drug reducing mortality most: Beta-blocker (carvedilol, metoprolol XL)
- Newest 4th pillar: SGLT2 inhibitor (dapagliflozin/empagliflozin)
- Best for LBBB + EF<35%: CRT-D
- End-stage treatment: Cardiac transplant
CAD - Recent Advances
- Best investigation for intermediate risk: CCTA
- Gold standard for ischemia physiology: FFR (≤0.80 = significant)
- Best intravascular imaging resolution: OCT
- Strongest new anti-anginal: Ranolazine
- Newest statin-independent lipid drug: Inclisiran (2x/year siRNA)
- Anti-inflammatory proven: Colchicine 0.5 mg (COLCOT/LoDoCo2)
- Best for complex 3VD: CABG (SYNTAX score >32)
- SGLT2i benefit in CAD: Empagliflozin reduces CV death in T2DM+CAD
Sources: Braunwald's Heart Disease (11e), Fuster and Hurst's The Heart (15e), Textbook of Family Medicine (9e), Goodman & Gilman's Pharmacology (13e), Katzung Pharmacology (16e), ACC/AHA 2022 HF Guidelines, ESC 2023 ACS Guidelines. Recent PubMed: DAPA ACT HF-TIMI 68 (2025, PMID 40884036), Inclisiran ORION trials, CLEAR Outcomes (bempedoic acid).